
Case Report | DOI: https://doi.org/10.31579/2690-8794/110
1 Radiology Department, Usmanu Danfodiyo University, Sokoto.
2 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
3 Radiography Department, Usmanu Danfodiyo University, Sokoto.
*Corresponding Author: SULE Muhammad Baba, Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule M.B., Gele I.H., Faruk K.U., Ribah M.M., Aliyu A.Z., Abacha M (2022) Giant Urinary Bladder Calculus In a Male Child With Features of Urethral Stricture: Radiologic Findings and A Case Report, J, Clinical Medical Reviews and Reports. 4(1); DOI: 10.31579/2690-8794/110
Copyright: © 2022, SULE Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2021 | Accepted: 16 December 2021 | Published: 05 January 2022
Keywords: dysuria; urinary bladder; giant calculus; hematuria
Bladder calculi usually occur in settings of chronic urinary retention, bladder outlet obstruction or urinary tract infection. Giant bladder calculus is defined as a calculus measuring greater than 4cm in its widest diameter or weighing greater than 100grams. The male gender is more affected than the female gender.
This is a case of an 11 year old male child with complaint of suprapubic pain, dysuria, hematuria, decreased urinary stream and increased frequency of micturition for more than three years prior to presentation.
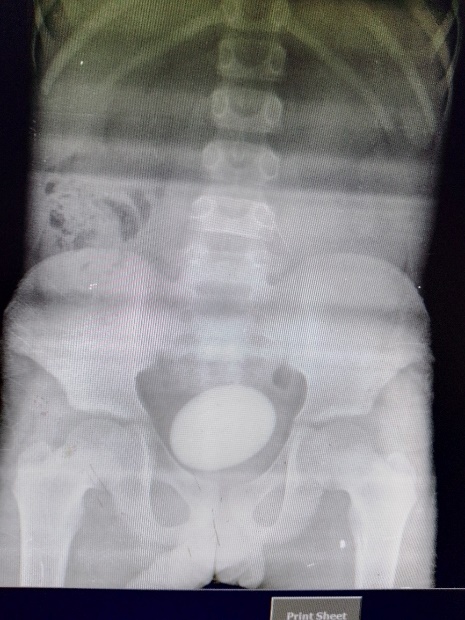
The patient had plain abdominal radiograph showing the region of the kidneys, ureters and urinary bladder (KUB) with an abdominopelvic ultrasonography. These demonstrated a calculus in the urinary bladder measuring about 70mm x 50mm in mediolateral and craniocaudal dimensions. The patient is yet to have a surgical extraction (extraperitoneal cystolithotomy) with of the entire calculus.
We present a case of a giant calculus in a child due to its rare nature and peculiar presentation.
Urinary bladder stones are a rare clinical entity accounting for about 5% of all urinary calculi, with the giant ones measuring more than 100grams even rarer [1].
Urinary bladder calculus is very uncommon and often associated with lower urinary tract obstruction as the etiology but a significant cases may come without obstruction, with the male gender been more affected than the female gender [2-5].
Giant bladder calculus is thought to develop from the nidus of an infected material or from a single ureteric calculus with associated progressive layer-wise deposition of calcified matrix most often in a setting of bladder outlet obstruction1.
Diet such as animal protein and sucrose especially in young adults, and amount of fluid intake are attributed to be important factors in the development of bladder stones [1, 6, 7].
Urinary stasis with causative factors which may either be urinary tract infection, benign prostatic hyperplasia, neurogenic bladder, urethral stricture, often lead to formation of calculi in the urinary bladder [8, 9].
Giant urinary bladder stone refers to vesical stone weighing more than 100g or measuring more than 4cm in its largest diameter, and only about 30 cases of giant bladder calculi were reported in the English literature [1, 10, 11].
Patient’s with features of bladder stone most often present with recurrent urinary tract infection, hematuria, dysuria, inability to pass urine, azotaemia and complaints of suprapubic pain or discomfort [1, 6, 12, 13].
Majority of vesical calculi are radio-opaque, and composed of triple phosphate, calcium oxalate, and calciumcarbonate [1, 14].
Urinary stones are usually detected by imaging, and often demonstrated by plain radiograph due to the calcium composition, however, cystoscopy, ultrasonography and computed tomography also play vital roles in imaging of bladder stones [6, 15].
The management of bladder calculi is aimed at relieving obstruction, treating the associated urinary infection and surgical removal of the calculus [15, 16]. The removal of the calculus surgically follows an open lithotomy (extraperitoneal cystolithotomy) or the endourological procedures and percutaneous cystolithotripsy [6, 10, 12, 17].
This is an 11 year old male child who presented with complaints of difficult micturition, supra pubic pains, increased urinary frequency, feeling of incomplete bladder emptying and hematuria. He had a history of trauma to the groin that was managed at home about 5 years prior to this presentation, following which these symptoms started gradually, and he was referred from a peripheral centre.
On examination he was found to be in painful distress and appeared anxious. He is oriented in time, place and person, not pale nor dehydrated. His urine examination yielded red blood and white blood cells with a negative culture. He had a packed cell volume (PCV) of about 32%.
The plain abdominopelvic radiograph (KUB) showed an oval egg-shaped radio-opacity of calcific density with a laminated appearance in the pelvic cavity measuring about 70mm x 50mm in mediolateral and craniocaudal dimensions (figure 1).
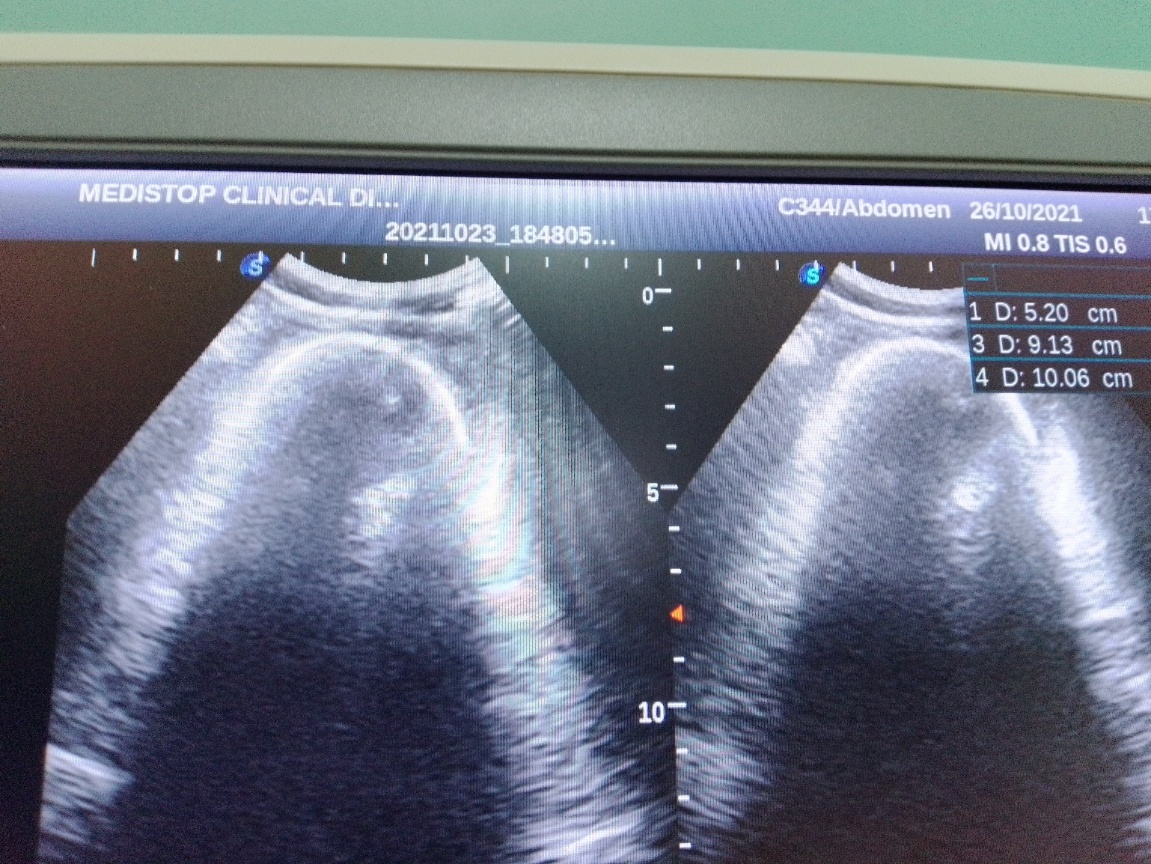
Abdominopelvic ultrasound showed a curvilinear area of increased echogenicity with associated posterior acoustic shadowing (figure 2). The ureters and calyces were not dilated currently
The patient is also advised to have a micturating cystourethrography (MCUG) or retrograde urethrocystography (RUCG) or both to rule out the possibility of a urethral stricture affecting either the posterior or anterior urethra respectively or involving both portions of the urethra.
The patient is been planned for extraperitoneal cystolithotomy with extraction of the entire calculus, however he is currently been placed on antibiotics and encouraged to have liberal fluid intake.
Urinary bladder stone is very uncommon and often associated with lower urinary tract obstruction as the etiology but a significant cases may come without obstruction, with the male sex more affected than the female sex [2-5]. The index case is a male child and had history of recurrent urinary tract symptoms with a suspicion of urethral stricture following an injury to the groin, these are in conformity to these literatures.
Giant bladder calculi are very rare and are often secondary to renal stones or to bladder outlet obstruction and bladder diverticulum [2-6]. Diet and amount of fluid intake are attributed to be important factors in the development of bladder stones [6, 7]. The case has been having adequate dietary and fluid intake, these had no contributory effect to the development of calculus in the index case.
Giant vesical calculus refers to bladder stone weighing more than 100g or measuring more than 4cm in its largest diameter [10, 11]. The index case had a bladder calculus measuring about 7cm x 5cm in its medio-lateral and cranio-caudal dimensions, thereby conforming to these documented literatures.
Patient’s with bladder calculus usually present with varying symptoms, such as recurrent urinary tract infection, hematuria, inability to pass urine, azotaemia and complaints of suprapubic pain or discomfort [6, 12, 13]. This case is not an exception, he presented with history of suprapubic pains, hematuria and difficulty following micturition, increased urinary frequency to mention but a few, thereby conforming to these literatures.
Majority of vesical calculi are radio-opaque, and composed of triple phosphate, calcium oxalate, and calcium carbonate, they are usually detected by imaging, and often demonstrated by plain radiograph due to the calcium composition, however, cystoscopy, ultrasonography and computed tomography also play vital roles in imaging of bladder stones [1, 6, 14, 15]. This case had plain radiography and ultrasonography of the abdomen and pelvis following which the calculus was demonstrated as a radio-opacity and echogenicity most likely from the calcium composition, thereby conforming to these literatures.
The treatment of bladder calculus is mainly focused at treating the urinary tract infection and relieving the obstruction by either surgical removal of the calculus or extracorporeal shock wave lithotripsy [1, 6, 12, 16, 17]. The index case is currently been planned for surgical extraction of the calculus (extraperitoneal cystolithotomy), thereby agreeing to these documented literatures.
Giant bladder calculus is rare especially in the pediatric age group, and often associated with bladder outlet obstruction. Plain abdominal and pelvic radiography with ultrasonography are appropriate radiologic examinations that can establish the diagnosis for prompt institution of management in the affected individuals.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
