
Case Report | DOI: https://doi.org/10.31579/2690-1919/440
Main Military Hospital Higher Institute (HMP/IS). Luanda, Angola.
*Corresponding Author: José Clayton Balo., Main Military Hospital Higher Institute (HMP/IS). Luanda, Angola.
Citation: © 2025, José Clayton Balo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright: José C. Balo, Loureiro J., Maquemba E, Hélida CJoão, Amaral E, (2024), Giant Neurocysticercosis, J Clinical Research and Reports, 18(1); DOI:10.31579/2690-1919/440
Received: 25 November 2024 | Accepted: 06 December 2024 | Published: 10 January 2025
Keywords: neurocysticercosis; parasitic infection of the nervous system; seizures and Taenia solium
Introduction: Neurocysticercosis is the most common parasitic infection of the central nervous system. About 50 million people are infected in developing countries and it is considered endemic mainly in Latin America, Central America, Asia and Africa. Many individuals are asymptomatic, but in symptomatic individuals, clinical findings depend on the location, size, number of cysts and autoimmune process related to parasite aggression. Headache and seizures are the most common clinical manifestations. Treatment can be medical and surgical with variable prognosis.
Objective: To report a clinical case with a pathological diagnosis of solitary and giant neurocysticercosis.
Clinical case report: A 35-year-old male patient, with no personal medical history, came in with headache and generalized tonic-clonic seizures, which were not preceded by auras, and bladder sphincter relaxation. A simple computed tomography of the skull with contrast was performed, showing a left frontoparietal hypodense rounded lesion, approximately 8 cm in diameter, with a hyperdense mural nodule that caused mass effect on the structures of the midline and adjacent gyri without contrast uptake; compatible with giant cystic neurocysticercosis. A left frontoparietal craniotomy was performed with evacuation of the cyst and removal of the mural nodule.
Conclusions: Neurocysticercosis is a prevalent disease in Angola. Generally, treatment is clinical, but in some cases surgical intervention is recommended, specifically in patients with single and giant neurocysticercosis associated with irritative and deficit symptoms, obtaining a pathological diagnosis of the lesion.
Neurocysticercosis (NCC) is the most common parasitic infection of the nervous system central nervous system (CNS) and is caused by the larva of Taenia solium, Cysticercus cellulosae. The cycle of the disease includes humans as the definitive hosts of Taenia solium and pigs as intermediate hosts infected by the larva. The parasitosis is considered a pandemic and occurs mainly in the form asymptomatic.[1]. According to the World Health Organization (WHO), the host tapeworm complex affects 50 million people worldwide and causes approximately 50.000 deaths a year.[2]. It is generated when Taenia solium eggs are ingested through contaminated water or food, a consequence of precarious environmental conditions,personal hygiene of the individual or by the mechanism of self-infection, a situation less frequent because it results from the reflux of proglottids from the intestinal contents to the stomach.[3,4]. The oncosphere in the parenchyma evolves through the following stages: vesicular, with a scolex and clear vesicular fluid; colloidal, first stage of involution,the vesicular fluid becomes cloudy and the scolex degenerates; nodular-granular, the wall of the cyst thickens and the scolex transforms into mineralized granules.[5]. Description of findings on head computed tomography (CT):First: Vesicular, of various sizes with ring enhancement that represent live cysticerci. It is a small cyst (up to 2.5 cm) with an eccentric point hyperdense corresponding to the scolex. The giant cyst is considered little frequent and usually unique. They are lesions larger than 5 cm, sometimes they can be racemosae.[3,6,7].Second: Hypopense area with interior ring reinforcement. It is considered that the decrease density with ring reinforcement is an intermediate stage between the live cyst and the calcified remnants. The resulting inflammatory reaction causes edema and arachnoiditis when there are cysts lodged in the basal cisterns. [6,7,8].Third: Parenchymal punctate calcifications (granulomas), usually without surrounding reinforcement, which correspond to dead parasites. [6,7,8]. Fourth: Hydrocephalus is the most common finding in patients with subarachnoid neurocysticercosis, sometimes accompanied by intraventricular cysts with equal density of cerebrospinal fluid (CSF), which to visualize them is Magnetic resonance imaging (MRI) is necessary. [7,8,9].Praziquantel and albendazole are frequently used drugs with antiparasitic action against Taenia solium cysticercus, effective between 60 and 85%.[6,10]. Surgery is a treatment used for cases of giant cysts, especially in those requiring a differential diagnosis.[6,7]. Intraventricular cysts or in the base cisterns do not respond well to clinical treatment, which requires, in In most cases, surgical removal that can be done with support endoscopic.[10,11]. In the case under study, treated at the Main Military Hospital Instituto Superior de Luanda, due to the magnitude of the intracranial injury and the symptoms recurrent cases, surgical intervention was the chosen therapeutic attitude associated with pharmacological treatment with albendazole for 30 days; repeated dose for 30 days after discharge. Giant single cystic neurocysticercosis is a form of rare imaging presentation. The objective was to present a clinical case with pathological diagnosis of solitary and giant neurocysticercosis.Clinical case
Complementary examsThe patient underwent a simple and contrast-enhanced head CT that showed a hypodense lesion in the left frontoparietal, approximately 8 cm in diameter, hyperdense mural nodule, discrete mass effect on the midline structures and adjacent gyri, without enhancement after contrast administration, compatible with giant cystic neurocysticercosis (figure. 1).

Figure 1: Contrast-enhanced CT of the skull with a giant cystic lesion and very little enhancement.
Treatment and evolutionFirst conduct: The patient was medicated with albendazole at 15 mg/kg, twice a day for 30 days.Secund conduct: The patient underwent a left frontoparietal craniotomy with puncture, cystic evacuation and removal of the mural nodule (fig.2).
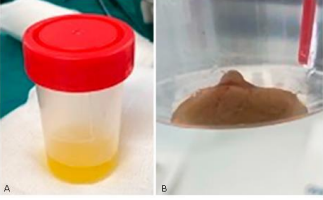
Figure. 2 - A): Aspirated cystic content; B) Anatomical piece, mural nodule removed.
Histology: In the histological examination, a cystic wall was observed with the presence of Calcified Cysticercus scolex (figure. 3)

Figure 3: Microscopic photograph of the cyst removed from surgery.
Evolution: The patient did not present headache or epileptic seizures. A CT scan was performed evolution that showed the disappearance of the cystic lesion in the craniotomy area frontoparietal and post-surgical epicranial edema. Furthermore, the examination revealed a subdural collection without mass effect on the frontoparietal brain parenchyma left (figure. 4). She was discharged with follow-up by outpatient consultation and was indicated a second course of treatment with albendazole at 15 mg/kg, twice daily for 30 more days.

Figure 4: Evolutionary computed tomography. (hyperdense image-red arrow-artifact)
Neurocysticercosis is a common cause of epileptic seizures worldwide and in In some cases it can become drug resistant, so surgical options must be present and lesionectomy with or without lobectomy is the surgery of choice. Suller et al [12]. presented a series of clinical cases of patients with epilepsy drug-resistant between the years 2008 to 2018, of them those who had one or more lesions suggestive of neurocysticercosis and who underwent surgery for epilepsy. Three patients met the selection criteria, two of them were women with an average age of 39.33 years. The mean age of onset of epilepsy was 17.33 years with a confirmed diagnosis of cysticercosis at the age of 30. One of the cases had multiple lesions of neurocysticercosis and mesial temporal sclerosis, the other two had single lesions in the temporal lobe, different from the patient under study,whose injury was left frontoparietal. In two cases of those analyzed, the lesionectomy, like the research case at hand, and in the other with multiple injuries, a temporal lobectomy. All patients are seizure-free current moment, including the patient under study. There are factors that predispose to the development of epilepsy such as susceptibility of the host, time of the pathogen evolution cycle and environmental factors that They favor infection and subsequently the development of the crisis. [12,13]. In countries where This disease is endemic, there are a large number of cases of neurocysticercosis asymptomatic and neurocysticercosis is detected in 25 to 55.2% in autopsies made for other reasons. In the same way, in these regions it is common find in neuroimaging tests calcified lesions suggestive of neurocysticercosis in asymptomatic patients or patients studied for other reasons. In these cases, neurocysticercosis represents an incidental finding without being a cause of epilepsy. [12,14].Epileptic seizures are the most common manifestation of NCC and can occur in any stage of the disease. The development of epilepsy related to NCC remains little known. Some possible explanations include a causal relationship direct, the result of an initial precipitating injury or linked to an external factor, and the remote possibility of coincidence. Several factors have been proposed that contribute to epileptogenesis, including calcified lesions, residual gliosis, response inflammatory immune system (influenced by genetic factors) and a possible association with hippocampal sclerosis. [13,14].CT and MRI are neuroimaging tests standard for the diagnosis of this disease. [8,15,16] The patient subject to investigation, a simple head CT with contrast was performed, which contributed to diagnose the disease in question. Aljure and others described the differences MRI imaging due to diffusion of brain abscesses and cystic gliomas.[17]. These lesions, according to their imaging characteristics, allow for a differential diagnosis with NCC in its cystic and giant form. [18,19,20].Colli and Carlotti (6) mention that the best treatment for the tumor form of NCC is surgical removal by direct access. In the case under study, the choice was made surgical treatment of the lesion with the objective of evacuating the cystic content and remove the mural nodule directly. Although in the case presented the treatment of choice was surgery, there is still not enough scientific evidence to prefer the surgical treatment or pharmacological treatment. [10,16,18].Although in other works Scientists describe that in the tumor form of NCC, surgical treatment by direct access is the most indicated. [21].In this report, due to the magnitude of the intracranial injury and the symptoms of compression of brain parenchyma due to giant cyst, surgical intervention was the most recommended therapeutic attitude, associated with medical treatment with albendazole at 15 mg/kg divided into two doses per day. NCC is a common nosological entity in regions with conditions precarious socioeconomic conditions and poor hygienic-eating habits. It is a problem of public health that can be prevented.In young patients with a history of seizures that are difficult to control, tests neuroimaging are of great importance for the differential diagnosis of other nosological entities such as arteriovenous malformations (AVM), whose epilepsy It is the most frequent debut symptomatology in young people. Antiparasitic drugs, such as albendazole and praziquantel, are of choice for the treatment of this disease, although in some cases with single lesions and giants with irritative and deficit symptoms, a surgical approach is recommended direct associated with antiparasitic pharmacological treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
