
Case Report | DOI: https://doi.org/10.31579/2690-4861/110
*Corresponding Author: Berrin Erok, Universtiy of Health Sciences, Department of Radiology, Prof Dr Cemil Tascıoglu City Hospital, İstanbul, Turkey.
Citation: Nu N Win, B Erok. (2021) Giant Joints in Association with Chronic Renal Failure. International Journal of Clinical Case Reports and Reviews. 6(4); DOI:10.31579/2690-4861/110
Copyright: © 2021 Berrin Erok, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2021 | Accepted: 08 March 2021 | Published: 11 March 2021
Keywords: tumoral calcinosis; chronic renal failure; sedimentation sign
Tumoral Calcinosis (TC) is an uncommon benign entitiy characterized by solitary or multiple tumorlike densely calcified periarticular masses located typically in the extensor surfaces of the large joints. TC can be primary or secondary. The primary TC is a rare hereditary familial disorder of phosphate regulation. On the other hand, secondary TC is associated with an underlying disease, most frequently, chronic renal faliure (CRF). Herein, we present a case of 40 year old male patient with CRF and 10 years history of hemodialysis, presenting with swellings around the right hip and left shoulder joints. The diagnosis of secondary TC has been made with typical computed tomography (CT) and magnetic resonance imaging (MRI) findings. Secondary TC is an uncommon condition particularly occuring in association with CRF. Typical radiologic findings and clinical history are leading in the diagnosis and prevent unnecessary further evaluations.
Tumoral Calcinosis (TC) is an uncommon benign condition characterized by solitary or multiple tumorlike periarticular/juxtaarticular depositions of calcium. Presentation occurs with solitary or multiple swellings typically located in the extensor surfaces of the large joints like hip, shoulder and elbow with less common involvement of knee and small joints [1]. TC can be primary or secondary. The primary TC is a rare hereditary familial disorder presenting in the first or second decade of life and it is further subclassified as primary hyperphosphatemic TC and primary normophosphatemic TC according to the underlying metabolic dysfunction of phosphate regulation [2, 3]. On the other hand, in secondary TC, there is an associated underlying disease causing multiple soft tissue calcifications, most frequently, chronic renal faliure (CRF) [3]. The underlying etiological mechanism for these massive periarticular calcifications in CRF is not clearly defined. Secondary hyperparathyroidism is suggested however, TC is also reported in the absence of secondary hyperparathyroidism [4]. Primary hyperparathyroidism, sarcoidosis, hypervitaminosis D and milk-alkali syndrome are among the other possible causes of secondary calcinosis [5]. We present a case of 40 year old male patient with CRF and 10 years history of hemodialysis presenting with secondary calcinosis of both hip and shoulder joints.
CASE PRESENTATION
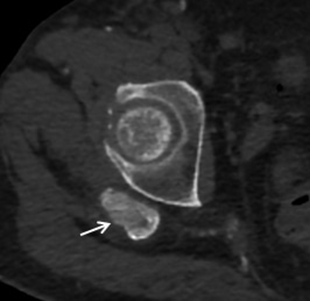
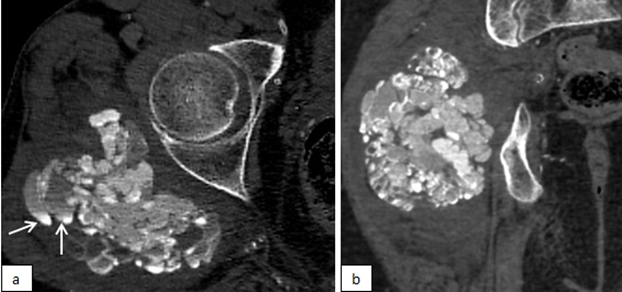
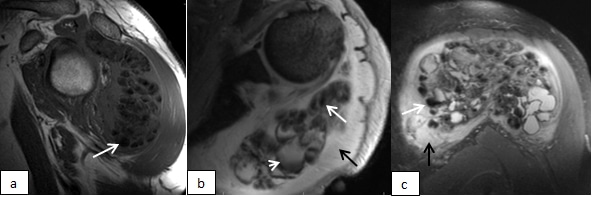
A 40 year-old male patient with CRF who had been undergoing hemodialysis for 10 years had an abdominopelvic computed tomography (CT) scan 2 years before and a small soft tissue calcification was found incidentally around his right hip joint (fig.1), which growed up to 10 cm without pain within 2 years. At that time, the lesion was a multilobulated, cystic, amourphous, densely calcified mass with multiple scattered fluid-fluid levels (fig. 2). There was no periosteal reaction or bony destruction. With history of CRF and typical CT features, the diagnosis of secondary TC was made. During this time another swelling around his left schoulder joint started to be grown up slowly without any symptom until the recently appeared pain which is aggrevated by movements of the joint. On magnetic resonance imaging [MRI], a periarticular soft tissue mass located in the subdeltoid bursa with the size of 14x11x8 cm was revealed. The lesion was heterogeneously hypointense on T1w and T2w images with scattered fluid-fluid levels (fig. 3). The adjacent bones had normal signal intensity but, prominent perilesional soft tissue edema was present, which is probably the cause of recently appeared pain in the slowly growing lesion. This second lesion was also diagnosed radiologically as secondary TC and confirmed by histopathological evaluation.
*Informed consent was taken from the patient.
Secondary TC is an uncommon complication observed in patients with CRF, particularly in patients on hemodialysis with an incidence of 0.5%–1.2% [4,6]. TC has a cahracteristic appearance on radiological imaging studies. Radiography and CT scans show multilobulated, amorphous, cystic and calcified periarticular soft tissue masses typically located in a bursal distribution [3,7]. These cystic areas often demonstrate fluid-calcium levels on CT scans, which is caused by layering of milk of calcium and named also as sedimentation sign [8]. On MRI, TC show heterogeneous low signal intensity on T1w images. On T2w images, it may show low signal intensity pattern as would be expected from calcifications or may show bright, nodular pattern having heterogeneous areas of high signal intensity and signal voids. After IV gadolinium administration, some enhancement may be seen as a result of hypervascularity in the walls of the cystic areas [9]. In CRF patients, these masses typically grow slowly over months or years without pain, and may become symptomatic as a result of mass effect on adjacent tissues. Our case, presented with a recently appeared shoulder pain in the slowly growing lesion and perilesional edema/inflammation demonstrated on MRI, which is a very rare finding in association with TC. In the absence of bony destruction, the main differential diagnoses for soft tissue calcifications include metastatic calcifications which are associated with abnormal calcium and/or phosphate levels and dystrophic calcifications which are often secondary to trauma, underlying inflammatory processes like connective tissue diseases or atypical infections [3]. The big globs of calcifications near the joints in TC is differentiated from the metastatic and dystrophic calcifications which appear finely speckled calcifications throughout many other organs, such as kidneys, lungs, gastric mucosa, eyes, skin, vessels and also in joints. Although not expected from primary TC, osseous destruction and/or intraosseous penetration is a rare but possible challenging feature in some cases of secondary TC in CRF patients reported in the literature. Steinbach et al. reported bony erosion along the humeral head and femoral neck in association with secondary calcinosis in CRF patients [10]. Girard et al. reported a case of secondary tumoral calcinosis with intraosseous penetration into the medullary space of the humerus [11]. The presence of osseous destruction poses a risk for pathological fractures and sometimes makes its differentiation from malignancy difficult. TC can show obvious FDG uptake on positron emission tomography which therefore is not useful for its differentiation from malignancy [12]. However, in secondary TC, clinical history, multifocality of the lesions, and also the absence of non-calsified components which are present in soft tissue sarcomas are generally helpful in differentiation from malignancy [13]. In equivocal cases, particularly in patients with solitary lesions with atypical findings like osseous destruction or perilesional edema, histopathological evaluation may be needed.
Secondary TC is an uncommon condition particularly occuring in association with CRF. Typical radiologic findings and clinical history are leading in the diagnosis and prevent unnecessary further evaluations. However, the presence of some atypical features, if present, can be challenging while making the diagnosis and histopathological evaluation may be needed in equivocal cases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
