
Case-Report | DOI: https://doi.org/10.31579/2578-8868/130
Neurosurgery Department, Pontificia Universidad Javeriana- Hospital Universitario San Ignacio, Bogotá, Colombia.
*Corresponding Author: Alejandro Vargas, Neurosurgery Department, Pontificia Universidad Javeriana- Hospital Universitario San Ignacio, Bogotá, Colombia.
Citation: Vargas A, Lindado C, Oscar F. Zorro., María X. Rojas., (2020) Giant intracranial aneurysmal bone cyst: Case report and literature review. J. Neuroscience and Neurological Surgery. 6(5); DOI:10.31579/2578-8868/130
Copyright: © 2020 Alejandro Vargas, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 15 July 2020 | Accepted: 23 July 2020 | Published: 31 July 2020
Keywords: aneurysmal bone cyst; cavernous hemangioma; benign lesion; surgical resection; embolization; cranioplasty.
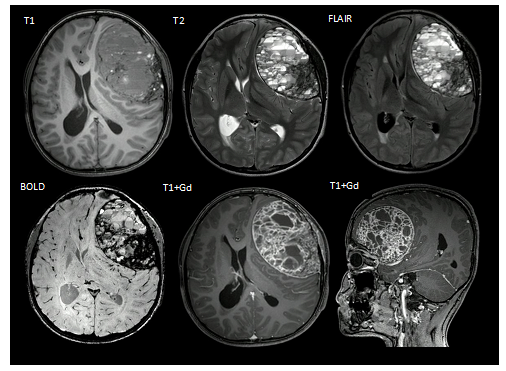
We present the case of a 13-year-old male patient with a two-month clinical picture of global headache and progressive decrease in visual acuity. Neuroimaging showed a well-defined giant left frontal lesion, hypointense in T1, with heterogenous signal in T2 and intense enhancement after gadolinium. The patient was treated with surgical resection and the lesion confirmed pathologically as Cavernous Hemangioma with focal component of aneurysmal bone cyst.
The aneurysmal bone cyst is a benign lesion of rapid growth and very destructive, which commonly occurs in metaphysics of long bones or axial skeleton, requiring radical treatment. It was first described in 1942, as an injury that occurred mostly in people under 20 years of age with a peak between 12 and 13 years, but very rarely occurs in the head and neck, mostly involving the occipital bone.
The case is presented below together with a review on the subject of Aneurysmal Bone Cyst, through databases such as EMBASE, PubMed and COCHRANE, selecting 70 articles that covered relevant aspects of its physiopathology, clinical and radiological manifestations and surgical approach.
Case report
We present the case of a 13-year-old patient with a two-month clinical picture characterized by persistent global headaches that did not improve with analgesics and progressive decrease of visual acuity compromising the ability to read and perform daily duties. No positive previous pathological history was recorded. On neurological examination: Visual acuity without correction with the use of pinhole (20/50 - 20/60), hypo-reactive mydriatic pupils and papilledema on fundoscopy. A simple and contrasted brain magnetic resonance study was indicated (Figure 1) which documented in the left frontal region, and extraaxial location, a lesion with well-defined contours and well defined hypointense capsule in T1 sequence and heterogeneous signal in T2, with multiple thin and thick septa, with intense enhancement after the administration of gadolinium together with cystic areas and with a hemorrhagic component as well as fluid levels. A cerebral arteriography was performed (Figure 2) which reported a lesion with moderate vascularization and afferent artery by middle meningeal artery, accessory meningeal artery and left superficial temporal artery, performing embolization of the arterial component of this last branch.
A surgical intervention was proposed by performing a block resection with a meticulous dissection of its cerebral parenchymal capsule requiring the resection of the bone table in the presence of evidence of infiltration at this level (Figure 3). Postoperatively, he was monitored in the intensive care unit and later transferred to the floor to continue monitoring without presenting an additional neurological deficit. He was sent home shortly after this. The pathological study (Figure 4) confirmed the presence of a cavernous hemangioma with a focal component of aneurysmal bone cyst. A follow-up imaging study was performed at 3 months that ruled out residual disease or recurrence presenting progressive recovery of visual involvement. He was electively scheduled for cranioplasty with PEEK graft, being operated without complications (Figure 5).




Aneurysmal bone cyst is a lesion that, despite being considered benign, is rapidly growing and highly destructive, most times requiring radical treatment [1,2]. Aneurysmal bone cysts are entities that commonly occur in the metaphysis of long bones or axial skeleton, and rarely occur in the head and neck. Additionally, the few cases in which part of the cranial vault has been affected, comprise mostly the occipital bone [3].
Historically, the first series of cases of Aneurysmal Bone Cysts was described in 1942 by Jaffe and Lichtenstein [4] who, due to the radiological characteristics of these tumors, which were shown to be hypervascularized bone lesions, gave it that name, which was later confirmed in several case reports; however, it always remained a rare entity that represented 1 to 5% of all primary bone tumors, and of these reported cases, only 6% were documented to be located within the skull [5].
These benign lesions usually occur in people under the age of 20, with a peak at approximately 12-13 years of age [6]. However, this does not completely eliminate the idea that these cases can sometimes occur in patients in the third decade of life, up to 49 years of age. It has also been shown that most studies do not show any preference for gender, that is, there is an equal proportion of men and women, although some studies have reported a higher rate of presentation in men.
With regard to anatomical location, as mentioned above, it is most commonly present in the metaphysis of long bones such as the femur, tibia and humerus, in a proportion of 52%; at the level of the spine it is present in 20% of cases and finally the least common location is at the level of the skull [1-6]. In fact, among the few cases in which the skull is affected, the occipital bone is known as a morphologically modified vertebra [3].
In this sites, these non-neoplastic lesions can show up in three distinct phases, an incipient, intermediate and stabilization phase; the first phase being characterized by lytic lesions and difficult to recognize when the lesion grows rapidly and becomes destructive, corresponding to the intermediate phase; and the third is when it presents a plateau or stable growth or calcified mass [7,8].
There is still controversy about the events involved in the process of formation of these cysts, it is believed that the mechanism is related precisely to these phases mentioned [3,9] That is, in the progression of the lesion, the initial phase of osteolysis of the marginal part of the bone with a discrete elevation of the periosteum is presented. The second phase is that of growth, which, as already mentioned, consists of the destruction of the affected bone, and therefore it is not easy to delimit the lesion on an imaging basis.
The third phase, known as stabilization, is where the real appearance of an aneurysmal bone cyst given by an expansive lesion with a cover or layer and bone septa is found. In some studies, a fourth phase known as recovery is added.
On the other hand, the role of genetic factors plays an important role in all this pathogenesis, since mRNA coding for insulin-like growth factor 1 has been found in the cells of these aneurysmal bone cysts, while in normal human tissue there are insignificant or very mild levels of this growth factor, for which it is believed to be related [6,9]. In addition, some studies have shown a translocation of the 16q22 and 17p11-13 genes, when the solid and extra-osseous variants of these lesions were present [5].
On occasion, the possibility has been considered that there is an abnormal increase in venous pressure, leading to congestion and bone expansion; as a result of either an arteriovenous malformation or related to a traumatic antecedent in the patient: which finally, leads to the appearance of an “egg shell” or “soap bubble”, due to the expansion of the cortical bone and periosteum [5,11]. Microscopically, the cysts present caverns filled with blood and serohematic fluid with endothelial cells and separated by septa composed of fibrous tissue, which contains multinucleated giant cells and osteoid tissue [10].
It is important to take into account that in many occasions the traumatic background is not present in the patient, therefore, it is not always an etiological factor. For example, when these injuries are deep in the anterior fossa, it is ruled out that they are the consequence of a direct injury that had sufficient trauma kinetics to produce such an injury [3.11]. For this reason, it is often considered that it is more related to the formation of arteriovenous shunt, by occlusion of the venous drainage, in addition to the genetic factors previously mentioned.
Two forms of bone cysts have been described, primary and secondary, the primary being those that occur as an isolated mass unrelated to another mass or lesion; while the secondary being those seen in association with giant cell tumors, non-ossifying fibroids, chondroblastomas, fibrous dysplasia, among others [11,12], A clear example of this is the case report presented by Stapleton [13], of a 33 year old patient who presented seizures after apparent trauma in childhood, imaging an expansive multi-cystic mass with a calcified center in the left temporal bone; when studied it was a chondroblastoma with an aneurysmal bone cyst of rare location. The same occurs in our case, in which a cavernous hemangioma with the focal component of an aneurysmal bone cyst is found.
Clinically, the symptomatology produced by aneurysmal bone cysts is related to the location in which they occur and additionally whether they are extra or intracranial [11]. In the first case, the most common, they present as masses with edema on the scalp, which distort the entire anatomical region and produce headache as the main symptom. In the second case, being intracranial, there is an elevation of intracranial pressure that can compromise the patient´s life, sometimes accompanied additionally by obstructive hydrocephalus. These two cases do not have mutually exclusive symptoms, i.e. it may occur that an extracranial mass grows to such proportions that it produces an elevation in intracranial pressure and a risk of facial-facial deterioration, as in the case of the patient presented here.
Additionally, the mass is usually painful and highly sensitive to palpation, which has grown in a short period of the time prior to diagnosis. As previously mentioned, depending on the location, in addition to the headache, it may cause neurological deficit or focusing, hearing loss, proptosis and epiphora in the case of a bone cyst in the ethmoid bone, seizures and signs and symptoms of endocranial hypertension [14]. Bone cysts in the spine or long bones can lead to pathological fractures, chronic pain and morphological alteration.
Different classification systems have been proposed for aneurysmal bone cysts. Cappana et al [15] divide them into five morphological groups, among which are Type I, which are centrally located and well-delimited lesions without external expansive lines; Type II are expansive and have cortical thinning with involvement of the bone segment; Type III involve only a cortex and are eccentric metaphysical; Type IV are subperiosteal and are the least common subgroup and finally Type V, expand peripherally penetrating the cortical bone.
On the other hand, Enneking [16] proposed to divide these bone cysts into 3 phases, the inactive, the active and the aggressive. The first of these phases is the one that is contained, and is therefore the most benign phase, because there is little expansion of the lesion and only a small amount of periosteal inflammatory reaction is present. The active phase is when the patient begins to present symptoms such as pain, in this case, headache and additionally, at the imaging level, a layer of inflammatory reaction is evident that separates the lesion from the morphology of the surrounding tissues is destroyed and the symptomatology becomes more florid.
These classifications refer not only to aneurysmal bone cysts found in the cranial vault, but also to those found in the long bones and spine. However, there is a way to classify more specifically those found at the level of the skull, based on two parameters, the first the growth phase in which the lesion is found and the second the direction of growth of the lesion. When talking about the growth phase, it must be taken into account whether the lesion is in lytic phase, stable or in calcification, which are the phases already explained above and this will lead to its classification in class I, II or III respectively. As for the direction of growth, it can be type A which is extracranial, type B intracranial or unrelated to bone structures, or type C [17].
Imaging diagnosis is very important in this entity, in the first instance a skull x-ray with or without angiography is the first crucal step to make not only a diagnosis but also an appropriate surgical plan, in order to define whether or not to perform preoperative embolization [18,19]. In the radiograph, various degrees of focal bone overproduction and the degree of surrounding morphological damage that may exist may be evident, giving the appearance of a radiolucent, destructive cystic lesion expanding to the cortical bone, with elevation of the periosteum and being contained by a layer of cortex; in other words the “soap bubble” appearance already explained above.
Likewise, when performing tomographic evaluation, it is evident whether the lesion is intra o extracranial but it is generally rare for it to invade the dura; this will serve to better define the limits of the lesion in a pre-surgical evaluation. When the study is complemented with a magnetic resonance with contrast, a multi-cystic or multi-lobed appearance will be ofund because of the septa it contains, with spaces filled with blood or serum-hematic fluid, geneatinf characteristic fluid levels. This finding suggests an aneurysmal bone cyst, but is not pathognomonic for this type of lesion [9].
When comparing conventional cranial radiography with cerebral magnetic resonance with contrast, it was found that, although the latter has better specificity, the former has better sensitivity and positive predictive value and for this reason it is considered the first crucial step at the time of diagnosis; while the resonance would be used as a complement to better define the heterogeneous lesion [9]. Angiography in long bones or spine is characterized by the demonstration of pathological circulation, with patchy distribution and occasionally forming an arteriovenous shunt; however this is not most frequent when located in the skull [20].
It is important to always keep in mind possible differential diagnoses that may share imaging characteristics with the aneurysmal bone cyst. As mentioned previously, multi-cystic imaging with fluid levels is characteristic, however, it can also occur in angiectatic osteosarcomas, giant cell tumors, among others. On the other hand, sometimes in the T1 sequence, dural tail signs appear; especially when the aneurysmal bone cyst is found to be invading the middle fossa in large numbers; therefore, a differential diagnosis with meningioma should be made [18,19]. These differential diagnoses can be complemented by an excisional biopsy, in order to rule out underlying tumors, always taking into account the risk of bleeding in the procedures. Up to 32% have been seen with benign secondary bone tumors [21].
Total surgical resection is the ideal treatment in addition to cranioplasty repair of the bone defect when necessary. Total on block resection will significantly reduce the possibility of recurrence of the lesion, and it has been shown that incomplete resection without clean margins can result in a recurrence of 20 to 70% [21,22]. In cases where the lesions are deep intracranial, for example, at the base of the skull, orbit, sphenoid bone or sinuses, it is more complicated to perform total surgical management; therefore, partial excision or curettage, in addition to adjuvant therapy such as radiotherapy, cryotherapy or embolization, is generally chosen [21,23]. In our patient, a total surgical resection of the mass could be performed, without the need for adjuvant radiotherapy, but with the need for embolization on two occasions and cranioplasty reconstruction at another surgical time.
In conclusion, aneurysmal bone cysts involving the cranial vault are extremely rare entities, however, cases have been reported that mostly involve the occipital region, although also in some proportion at the temporal and parietal level. Their diagnosis depends not only on the clinic but also on the characteristics of the multiloculated mass with fluid levels at the imaging level and on whether the lesion is primary or secondary, also remembering the importance of the conventional radiography as a first step for the diagnosis of this entity. It is necessary to perform a total resection of the same to achieve the highest success rate with the least recurrence, then requires a follow-up over a long period of time to assess the malignant transformation or recurrent appearance of symptoms.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
