
Case Report | DOI: https://doi.org/10.31579/2768-2757/150
Department GI Surgery,Vamshodaya Hospital, Kolar, India.
*Corresponding Author: Vinay H G., Department GI Surgery,Vamshodaya Hospital, Kolar, India.
Citation: Vinay H G., (2024), Giant Hydronephrosis Due to Ureteropelvic Junction Obstruction in A 53-Year-Old Male: A Case Report., Journal of Clinical Surgery and Research., 5(9); DOI:10.31579/2768-2757/150
Copyright: © 2024, Vinay H G., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2024 | Accepted: 08 November 2024 | Published: 13 December 2024
Keywords: giant hydronephrosis; uretero-pelvic junction obstruction; abdomen; kidney
The hydronephrotic kidney, resulting from an uretero-pelvic junction obstruction (UPJO), presents commonly as a clinical condition, with the presence of usually no more than 1‑2 liters in the collecting system, but a very small number of cases of giant hydronephrosis (GHs) has been reported in adults. In this case report a 53-year-old male was admitted to the Vamshodaya Hospital Kolar, Karnataka, India in November 2023 with an abdominal pain since 15 days and abdominal distention since 6-months. Computed tomography was performed, finding large thin walled cystic mass in right side of abdominopelvic region (40x32x27cm) showing few incomplete septations, fluid density within lesion and causing significant mass effect and displacing the rest of the abdominal contents. Such cases are rarely presented; therefore the aim of the present case study was to document a clear case of GH resulting from UPJO.
The overall definition of hydronephrosis is dilatation of the renal pelvis and calyces as a result of partial and sporadic restriction of the urine's flow [1].Hydronephrosis can be unilateral or bilateral, depending on where the urine flow restriction occurs. A unilateral hydronephrosis happens when the blockage is higher than the bladder's level. Between the ages of one and eighty, the incidence of unilateral hydronephrosis was determined to be 1:100. The right side is more frequently afflicted by unilateral hydronephrosis, which is most frequently caused by idiopathic pelvi-ureteric junction (PUJ) blockage or calculus. The female to male ratio of this condition is 2:1. It might be the consequence of aberrant smooth muscle growth at PUJ [2, 3].With a range of treatment programs, it is now possible to detect the etiology of stone illness in over 95% of patients, and most individuals with recurrent calculi can have their stone production stopped or delayed. The advent of extracorporeal shock wave lithotripsy (ESWL) and percutaneous lithotripsy has led to a most remarkable and amazing accomplishment [4]. The symptoms of GH can vary from vague symptoms like nausea, constipation, dyspepsia, fever, asthenia, mild diffuse abdominal pain or flank discomfort, chronic low back pain, recurrent urinary tract infections, and hematuria to asymptomatic abdominal distension until the late stages of the disease [5]. Most cases of this illness will be identified in the early stages of childhood and infancy. Prolonged irritation can lead to progressive and gradual consequences such hypertension, renal failure, ruptured kidneys, and malignant transformation if left untreated [6]. Although the clinical signs of these patients are not particular, they frequently involve a bloated abdomen and an elevated belly circumference. Hematuria, persistent stomach pain, flank pain, and recurrent UTIs are some other symptoms. Despite having ambiguous and broad clinical signs, massive hydronephrosis has only ever been properly diagnosed in 50% of cases [7]. Our objective is to report a case ofrare entity as the giant hydronephrosis.
Case Report:
A 53-year-old male was admitted to the Vamshodaya Hospital Kolar, Karnataka, India in November 2023 with an abdominal pain since 15 days and abdominal distention since 6 months. Patient was apparently normal 6 months back, later he developed abdominal distention associated with minimal pain, then gradually abdomen uniformly distended. Hence came to hospital for further evaluation and management. Patient had no complaints of dysuria, discoloration of urine or any other irritative urinary symptoms. There was negative history of nausea, vomiting, constipation, fever, weight loss, and anorexia. Also he had no history of stone disease and, or any other urologic problem. In physical examination there was no positive finding except gross abdominal distention. On Ultrasound of Abdomen showed huge cystic lesion with thick internal echoes and septations in abdomino pelvic region measuring (37 X 33 X 27 cm) and it is causing significant mass effect and displacement of all the abdominal organs. No sonological evidence of solid component/ calcification/ internal vascularity. No free fluid in pleural spaces. Visualized bowel loops show normal peristalsis. On Renal cortical scan was performed by injecting 5mci 99m TC- DMSA intravenously and delayed static planer images were acquired in posterior projections using High Definition detectors with low energy high-resolution collimation (Dual head SPECT system).There was significant SOL occupying most of the anterior abdomen, especially in the right side that is observed to push the left kidney more laterally to the left. Computed tomography was performed, finding large thin walled cystic mass in right side of abdominopelvic region (40x32x27cm) showing few incomplete septations, fluid density within lesion and causing significant mass effect and displacing the rest of the abdominal contents (intra and retroperitoneal contents), Figure 1.The lesion is causing significant mass effect and displacing the rest of the abdominal contents. The entire bowel loops are displaced to left side of abdomen.It is also displacing the retroperitoneal structures like aorta and IVC. Right kidney is not visualized separately from the mass lesion. Right lower ureter is seen and upper ureter blending with the lesion Features likely suggestive of right non-functioning kidney with gross hydronephrosis occupying entire right side of abdomen and pelvis probably due to PUJ obstruction. Enlarged prostate with back pressure changes in bladder, Figure 2. Using technique suspended respiration 2 mm contrast enhanced (with oral & IV contrast) sections of the pelvis and abdomen were obtained.
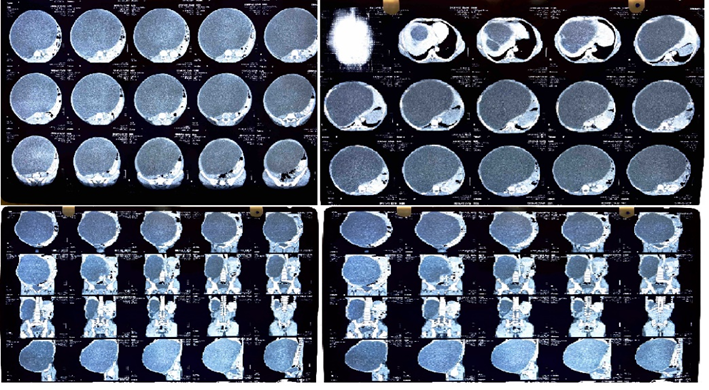
Figure 1: Abdominal computed tomography.
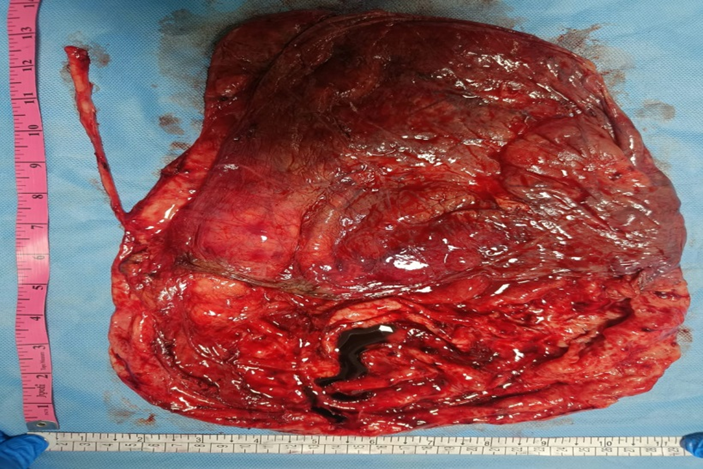
Figure 2: Gross appearance of right Kidney after nephrectomy,
shows large kidney with huge pelvis.
On histopathology report showed right nephrectomy specimen measuring 27 x 15 x 6 cm. Ureter measures 12 cm in length. External surface of kidney is enlarged and cystic. Capsule is adherent at places and areas of congestion noted. Cut section - Entire kidney is cystically dilated. Cortico-medullary junction and pelvi calyceal system cannot be made out. Cortical thickness measures 0.1 cm to 0.5 cm. No stones noted. Cut section of ureter is unremarkable. No stricture is seen.
Microscopic study:
Sections studied from kidney show atrophic glomeruli and atrophic tubules lined by attenuated epithelium and lumen filled with eosinophilic material (thyroidisation), Figure 3. Few of the tubules were cystically dilated. Many congested blood vessels and areas of hemorrhage noted. Stroma show mixed inflammatory infiltrate comprised of neutrophils,lymphocytes and plasma cells. Focal area showed hemosiderin laden macrophages. Lymphoid follicles were also noted. Section studied from pelvi calyceal region showed urothelial lining and underlying stroma showing dense mixedinflammatory infiltrate rich in neutrophils. Section studied from ureter appears unremarkable.Sections were negative for granulomas or malignancy.
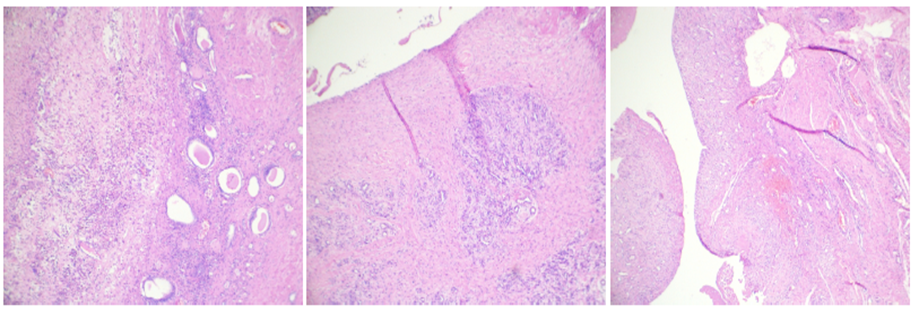
Figure 3: Features are of Acute on chronic pyelonephritis with hydronephrosis - Right kidney.
Post-operative period was uneventful. Patient was shifted to wards in view of symptomatic improvement. Drain removed on pod 4. Patient was improved clinically during the course of stay in the hospital. Hence patient was being discharged.
Since abdominal CT lowers the risk of needless surgery and treatment expenses, it is a gold standard diagnostic technique for patients experiencing lower back discomfort [8]. While USG is the preferred procedure for treating patients with radiation exposure, pregnant patients, and children despite CT's superior accuracy, USG is also more affordable, easier to administer, and doesn't use ionizing radiation [9]. Congenital hydronephrosis is most commonly caused by occlusion of the ureteropelvic junction. A dilated renal pelvis and calyces devoid of ureteral dilatation will be shown on a USG or IVP. Prolonged washout half time, or an obstructive pattern, will be shown on diuretic renography or renal scan. Some children with UPJ blockage may also have vesicoureteral reflux. Congenital hydronephrosis has ureteropelvic junction blockage as its second most common etiology. On renal USG and/or IVP, hydronephrosis is observed together with concomitant ureteral dilatation. There may be an obstructive pattern on a renal scan. Three main categories of dilated ureters (megaureters) exist: non-obstructed, non-refluxing megaureters, refluxing megaureters, and obstructed megaureters [10]. The multicystic, dysplastic kidney, ectopic ureter, megacalycosis, simple renal cyst, urachal cyst, ovarian cyst, hydrocolops, sacrococcygeal teratoma, bowel duplication, duodenal atresia, anterior meningocele, and prune belly syndrome are additional causes of hydronephrosis or apparent hydronephrosis [11]. The percentage of cases with bilateral hydronephrosis varies quite a bit, while it is just 3% in the study of Haralambous et al [12]. The study by Hawthorne et al. still shows a greater male predominance, 76:24 [13]. According to research by Johnston et al., the left side has about 70% of the patients with ureteropelvic junction obstruction that are discovered antenatally [14]. The study by Kass et al. indicates that approximately 55% of the cases were resolved postnatally [15]. This is a quite significant rate. On the other hand, only a relatively small percentage of instances were documented in a study done by Keller and colleagues. In addition to identifying hydronephrosis, the antenatal Ultrasonography should record the amount of amniotic fluid, the degree of bladder distension, the ureter's wall thickness and emptying, the presence of any abnormalities in the opposing kidney, and the kidneys' echogenicity [16].
| Author | Age/gender | Size of mass (cm)/ quantity of fluid (ml) | Initial symptoms | Treatment | Cause of GH |
| Schrader AJ, et al, [17] | 78/F | 35x30x25/30,000 | Nausea, vomit, fatigue, fever, weight loss | Puncture/drainage, Nephrectomy | Tumor |
| Vishwanath M et al. [18] | 65/F | 30x20x25/15,000 | Fatigue, fever | Nephrectomy | Obstruction |
| Wu CC and Sun GH [19] | 45/M | 30x20x20/15,000 | Anemia, liver dysfunction | Nephrectomy | Stone |
| Tazi MF et al. [20] | 42/M | 44x32x30/20,000 | Weight loss | Nephrectomy | Bladder neck obstruction |
| Mediavilla E et al. [21] | 82/M | 30x21x10/4,500 | Fever | Nephrectomy | Tumor |
| Golcuk Y et al. [22] | 83/M | 20x16x22/4,000 | Nausea, vomit, fatigue, fever, weight loss | Puncture/drain nephrectomy | Ureteral stone |
Table 1: Following cases of GHs reported in the study.
The primary modality for diagnosis was USG abdomen. Surgical intervention is used to treat hydronephrosis, depending on its etiology and grade. The most appropriate surgical procedure for treating GH, a rare illness linked to the development of cystic abdominal masses, is a nephrectomy.
No funding sources .
None declared .
The study was approved by the Institutional Ethics Committee.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
