
case report | DOI: https://doi.org/10.31579/2690-4861/425
1Department of Anesthesia and Intensive Care Medicine, Rikshospitalet, Oslo University Hospital, Norway.
2Department of Transplantation Medicine, Rikshospitalet, Oslo University Hospital, Norway.
3Section of Clinical Immunology and Infectious Diseases, Rikshospitalet, Oslo University Hospital, Norway.
4Department of Respiratory Medicine, Faculty of Medicine, University of Oslo, Norway.
*Corresponding Author: L. Fjellbirkeland, Department of Respiratory Medicine, Faculty of Medicine, University of Oslo, Norway.
Citation: LE. Kvarstein, A. Barratt-Due, DO. Dahle, I. Nordøy, L. Fjellbirkeland, (2024), Generalized Varicella Zoster Virus Infection with Pseudomembranous Tracheobronchitis following a high-Risk Kidney Transplant Protocol, International Journal of Clinical Case Reports and Reviews, 18(2); DOI:10.31579/2690-4861/425
Copyright: © 2024, L. Fjellbirkeland. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2024 | Accepted: 08 April 2024 | Published: 27 June 2024
Keywords: kidney transplant; immunosuppression; varicella zoster virus; pseudomembranous trachebronchitis; pseudomonas aeruginosa
Kidney transplant recipients are susceptible to infections. We present a middle-aged woman who underwent a high-risk immunosuppressive treatment protocol due to a pre-transplant immunization. Six weeks after transplantation she developed severe respiratory failure and endotracheal intubation was required. Bronchoscopy revealed extensive endobronchial membranes, and the lavage fluid tested positive for Pseudomonas aeruginosa. After repeated bronchoscopic removal of membranes, she developed a generalized vesicular rash, positive for Varicella zoster virus, later also identified in the bronchial fluid. After 34 days on mechanical ventilation, she was successfully decannulated and could be discharged from hospital three months later, although still in need of a nasogastric tube for feeding, with a functioning kidney graft. This report underscores the significance of herpes viruses as potential contributors to severe respiratory infections in organ transplant recipients, alongside highlighting the atypical manifestations of bacterial infections.
Potent immunosuppressive treatment may lead to reactivation of latent Varicella zoster virus (VZV) resulting in systemic infections and viral pneumonitis [1-3]. Pseudomembranous tracheobronchitis (PMTB) is a rare condition, but is reported in immunocompromised individuals [4]. PMTB is usually caused by Aspergillus spp., but other microbial agents have been reported [4, 5]. Stridor and serious central airway obstruction have been described, but clinical signs vary related to the extent of pseudomembranes. Bronchoscopy is essential to obtain a precise diagnosis. Treatment includes both anti-microbial agents and repeated toilet bronchoscopies [4, 6, 7]. In this case report, we describe a strongly immunosuppressed patient who developed generalized VZV infection, and P. aeruginosa superinfection, leading to the rarely described condition PTMB. Due to late emergence of the classical vesicular rash, the diagnosis of VZV and adequate treatment were delayed. In this report, we highlight the clinical presentation of a VZV infection and the uncommon diagnosis of PMTB.
A 47-year-old female with IgA nephropathy developed a severe respiratory failure six weeks after kidney transplant. The patient had high levels of human leukocyte antigen antibodies, and according to the Norwegian transplantation program, a high-risk immunosuppression regimen was required. This includes tacrolimus, mycophenolate mofetil (MMF), basiliximab, rituximab, intravenous immunoglobulins (IVIG), and high-dose methylprednisolone (500mg) [8, 9]. Additionally, the patient received prophylactic P. jirovecii treatment with trimethoprim sulfamethoxazole [10]. Postoperatively, the kidney transplantation was considered successful with a well-functioning graft. Four weeks after the transplantation, she was re-scheduled for surgical fenestration of a kidney-close lymphocele (defined as Day 0). During anaesthetic induction, intubation was disrupted due to aspiration. During the following week the patient became increasingly dyspnoeic with stridor and was transferred to the ICU for closer surveillance and non-invasive ventilation support. Her chest x-ray on Day 13 showed bilateral patchy infiltrates as in bronchopneumonia (Figure 1).

Figure 1: Chest X-ray taken on Day 13 showing bilateral patchy infiltrates. (V = left).
Despite antibiotic treatment with cefotaxime and corticosteroids for what was assumed to be an aspiration pneumonitis, her respiratory distress worsened markedly with a concomitant increase in inflammatory parameters. On Day 15, the patient was endotracheally intubated and
mechanical ventilation started, using lung-protective settings. She was highly oxygen dependent with a PaO2/FiO2 ratio of 7,6 kPa (57mmHg) but responded positively to prone positioning and removal of large amounts of pleural effusion.

Figure 2: Chest X-ray taken on Day 17, two days after intubation and on mechanical ventilation. Right upper lobe shows signs of atelectasis and consolidation (asterisk). In the left lung there are extensive patchy infiltrates with partial atelectasis (arrow).
A follow up chest x-ray on Day 17 showed increasing atelectasis (Figure 2) and repeated bronchoscopies the next days turned out to be of utmost importance. Her airways were completely covered with a continuous membranous pale layer, starting along the tracheal tube, reaching down into the bronchial segments (3rd generation bronchi) narrowing the inner lumen significantly. The membranes completely covered the entrance to the left upper lobe, while the right upper lobe bronchus was left with a small remaining lumen (Figure 3).
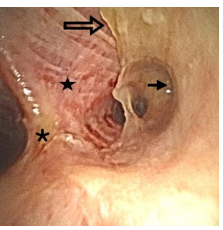
Figure 3: The right main bronchus with the carina (asterisk) to the left as seen through the bronchoscope. The membrane (open arrow) was easily detachable by forceps and revealed a raw, inflamed bronchial wall underneath (star). The bronchial orifice to the upper right lobe was significantly narrowed (arrow).
With a combination of flushing with saline and use of forceps, the membranous layers were successively removed down to the segmental level. The membranes were easily detached in large pieces from the wall. Due to their large size, the individual pieces had to be removed mechanically by retracting the bronchoscope with the forceps in place. Bronchoscopy had to be repeated over three consecutive days before the bronchial lumens were found to be satisfactorily open. The removal exposed a large wound surface, however, there were hardly any signs of reappearance of the membranes. Microbial tests of bronchial fluid demonstrated growth of P. aeruginosa despite antibiotic coverage with meropenem from the time of intubation. No Aspergillus spp. or other common respiratory pathogens were found in our patient. Due to deteriorating renal function, continuous renal replacement therapy (CRRT) was started on Day 18. On Day 20, the patient developed a generalized vesicular rash. Qualitative PCR test of fluid from vesicles and peripheral blood was positive for VZV DNA (Altona Realstar GmbH, Hamburg, Germany). New testing on blood samples taken before her transplantation came up positive for VZV IgG, indicating that the current VZV infection was caused by reactivation. Retrospective blood analyses also demonstrated VZV DNA one day ahead of the surgical fenestration of her lymphocele, and repeated chest x-rays showed progressive, scattered nodular and reticular consolidations in both lungs compatible with VZV pneumonia (Figure 1). Upon reassessment, the bronchial lavage samples collected at the time of intubation also revealed the presence of VZV DNA in the patient's airways. Intravenous acyclovir was started on Day 20, and considering her critical state, immunosuppression and prolonged hospitalization, linezolid and anidulafungin were empirically added. Regarding her immunosuppression, the dosages of tacrolimus and MMF were held stable during her intensive care course, and additional corticosteroids were initially added, based on the suspected aspiration pneumonitis. However, after the findings of VZV, the methylprednisolone dosage was lowered to baseline level of 15 mg. After a distinct increase in plasma levels of tacrolimus on Day 21, the dosages of tacrolimus and MMF were both reduced. From Day 22 her respiratory failure gradually improved, sedatives could be reduced, and linezolid and CRRT were terminated on Day 25. Due to an unsuccessful extubation on Day 27, she was tracheostomized to ease further weaning from the ventilator. Her vesicular rash had developed into crusty lesions, but blood tests showed persisting VZV viremia. Antiviral treatment was therefore continued, while antibiotics and antifungal treatment were discontinued. The further weaning of the ventilator was complicated by new infections and recurring need of broad-spectrum antibiotics. On Day 49, after 34 days of mechanical ventilation, she could finally be decannulated and transferred to a hospital ward for rehabilitation with a well-functioning kidney graft. VZV DNA was detected in her blood until Day 60. She was discharged from the hospital on Day 118, still in need of a nasogastric tube feeding and further rehabilitation.
It is evident that transplant patients are especially susceptible to infections due to use of a broad spectre of immunosuppressive medication. Drugs associated with T-cell depletion predispose to viral infections, candidemia and Pneumocystis pneumonia. B-cell depletion make patients vulnerable to certain capsulated bacterial airway infections, and corticosterioids to a broad range of bacterial, viral, and fungal infections (1, 11). VZV infections are typically characterized by a vesicular rash. A recent literature review emphasizes the late presence, up to three weeks, or even complete absence of skin eruption in kidney transplant patients subjected to systemic VZV infection (12). As the herpes viruses are usually not part of a standard airway multiplex PCR, conscious diagnostics are needed. Both P. aeruginosa and VZV were identified in our patient. VZV can indeed lead to severe pneumonitis (13), but bronchial pseudomembranes are not described. PMTB, however, has been reported in intubated, immunocompromised patients suffering a P. aeruginosa infection (4).
We conclude that our patient most likely developed a VZV pneumonia following an ongoing viremia with a subsequent P. aeruginosa driven PMTB. The current case is a reminder of atypical presentations of viral and bacterial infections in immunocompromised patients. Balancing infectious control and immunosuppression is challenging and requires a vigilant practice to prevent serious complications. In our case an initial aspiration and the late presence of the vesicular rash delayed the correct diagnosis and effective treatment.
PCR: Polymerase chain reaction.
VZV: Varicella zoster virus.
BAL: Bronchoalveolar lavage.
PMTB: Pseudomembranous tracheobronchitis.
CRRT: continuous renal replacement therapy.
MMF: Mycophenolate mofetil.
IVIG: Intravenous immunoglobulins.
Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this case report.
Written consent for publication was obtained from the patient prior to submission of this manuscript in line with Oslo University Hospital consent form.
The authors declare that they have no competing interests.
Not applicable.
All authors participated in the treatment of the patient. LEK has written the initial draft of the manuscript. All authors have reviewed and approved the final version of the manuscript. LF is the last and corresponding author of the case report.
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
