
Research Article | DOI: https://doi.org/10.31579/2692-9392/009
*Corresponding Author: Jaafar Nakhli, Department of Plastic Surgery Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER) Pondicherry India-605006.
Citation: Nakhli J, Yousri E. kissi., Braham A., Mtiraoui A., Bochra N. Saguem., Selma B Nasr. (2020) Gender Differences in Sexual Dysfunction of Patients with Schizophrenia. J. Archives of Medical Case Reports and Case Study. 3(1); DOI:10.31579/2692-9392/009
Copyright: © 2020 Jaafar Nakhli,This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
Received: 26 December 2019 | Accepted: 18 January 2020 | Published: 27 January 2020
Keywords: sexual dysfunction;schizophrenia
The prevalence of sexual dysfunction in patients with schizophrenia ranged from 50 to 85%. One hundred outpatients with schizophrenia had participated in this study. All these patients had remission criteria. We used sociodemographic and clinical characteristics from medical files and we passed to our patients PANSS and ASEX. Comparison was between female and male groups. Sexual dysfunction was present in 55% of patients with schizophrenia. Women had higher total ASEX score than men especially in Arousal disorders and orgasm. There was a relationship between the ASEX total score and dose of treatment and with the severity of symptoms.
Schizophrenia is a chronic and disabling mental illness of the young. It has a pronounced impact on the sexual abilities of patients. In the literature, the prevalence of sexual dysfunction in these patients ranged from 50 to 85% [1-3]. Many factors can explain this high prevalence such as hyperprolactinemia, sedation and antagonism of neurotransmitter receptors induced by antipsychotic drugs [4,5].
These sexual dysfunctions can affect their quality of life, self-esteem, attitude toward taking medication and compliance during therapy [5].
Detecting and treating this problem could improve the course and the quality of life of patients with schizophrenia.
This study aimed to assess the prevalence of sexual dysfunction in patients with schizophrenia and to investigate associated gender factors.
This study was approved by the ethics committee of the Faculty of Medicine in Sousse. We have performed this study with one hundred first outpatients with a diagnosis of schizophrenia (DSM-IV TR criteria) from the outpatient psychiatric service of Farhat Hached Hospital in Sousse. All these patients met remission criteria of “The Remission in schizophrenia Working Group” with Positive and Negative Syndrome Scale score < 90 and without any admission in psychiatry since the past 6 months [6].
We administered to our patients a record exploring the sociodemographic and clinical characteristics, the Positive and Negative Syndrome Scale (PANSS) [7] and Arizona Sexual Experience Scale (ASEX) to assess sexual dysfunction. ASEX scale was translated and validated into Arabic language [8]. Arabic version of ASEX had good internal consistency (α=0.82) and excellent reliability (r=0.92, p<10(-3) [8].
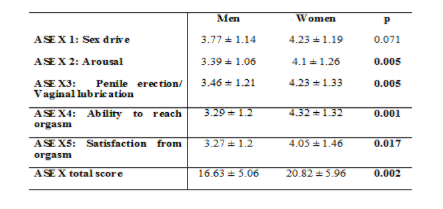
The ASEX scale is commonly used to evaluate sexual dysfunction scales in patients with mental disorders. It’s a five-item rating scale that quantifies sex drive, arousal, vaginal lubrication/penile erection, ability to reach orgasm, and satisfaction from orgasm. Possible total scores range from 5 to 30, with the higher scores indicating more sexual dysfunction. The patient has sexual dysfunction when the ASEX total scores ≥ 19 or has an item with a score ≥ 5 or 3 items with a score ≥ 4 [8,9].
The mean age of our sample was 37.6 ± 10.2 years. 70% were male, 57% were single and 73% were unemployed.
The mean age of onset illness was 24.8 ± 6.1 years. Undifferentiated schizophrenia subtype was the most prevalent (58%). The mean PANSS score was 51.8 ± 12.8.
43% of this patient has received second generation antipsychotics and the average of Chlorpromazine equivalent dose was 279 ± 475 mg/day.
The mean ASEX total score was 17.7 ± 5.6. Sexual dysfunction was present in 55% of patients with schizophrenia (total score ≥ 19 or ASEX Item ≥ 5 or ≥ 3 items with a score ≥ 4).
The two gender groups was comparable regarding age, age of onset, years of onset of schizophrenia, the mean PANSS score and dose of treatment.
Women had higher total ASEX score than men (20.8 ± 5.9 vs 16.6 ± 5; p = 0.002). Scores of arousal disorders, vaginal lubrication, orgasm and sexual satisfaction were higher in women than men (p respectively was 0.005, 0.005, 0.001 and 0.017) (Table I).
There was a relationship between the ASEX total score and dose of treatment (r = 0.36, p = 0.001) and with the severity of symptoms (r = 0.31, p = 0.005).
The prevalence of sexual dysfunction in patients with schizophrenia in our study was 55%. This result was similar to the literature with prevalence between 30 to 80% [1-3,8]. In a tunisian sample, Ben Mahmoud and al. found a frequency of 93% [9]. Many studies have shown that the sexuality of patients with schizophrenia is more impaired than general population [1-3,10,11].
In China’s study using ASEX in patients with schizophrenia, sexual dysfunction was found in 61.9% of men’s and 79.2% in women’s [12]. The high rates and gender differences we observed are consistent with other studies [13,14]. According to Harley et al., women with schizophrenia experienced more problems in desire and men were more likely to report problems in arousal [15].
Ben Mahmoud had found a decrease in desire and arousal in women with schizophrenia [11]. Miclutia pointed the importance of the relational component, sentimental and emotional sexuality in women compared to men [16].
In Fujii’s study, the most sexual dysfunctions in men were sexual desire, erectile dysfunction and ejaculation problem. It was sexual desire in women [17].
Literature data states that all sexual dysfunction can be observed in schizophrenia. They can be attributed to many factors such as the disease [18], the precarious social situation of patients, and the adverse effects of prescribed antipsychotic medications [1,19].
In our study, we found correlation between the severity of symptoms, particularly negative symptoms, and the severity of sexual dysfunction. It has been observed in many studies that cognitive deficit in schizophrenia predicts a progressive deterioration of sexual function [2,3,20].
For the relationship found between sexual disorders and antipsychotic daily intake, Devraux reported no difference between first and second generation antipsychotics [21]. Many studies have found a relationship between blocking D2 receptor, desire and orgasm. In the same way, hyperprolactinemia and low plasma testosterone causes lower desire and erectile dysfunction [15,22,23].
Variety of mechanisms are likely to contribute to antipsychotic-related sexual dysfunction, including hyperprolactinemia, sedation, and antagonism of a number of neurotransmitter receptors (α-adrenergic, dopaminergic, histaminic and muscarinic) [4,5,23]. Hyperprolactinemia is a major cause of sexual dysfunction. Based on the blockade of dopamine D2 receptors, haloperidol, risperidone, and amisulpride are classed as prolactin-elevating antipsychotics, while olanzapine, clozapine, quetiapine, ziprasidone, and aripiprazole are classed as prolactin-sparing drugs [4,5].
Conclusion:
Sexual dysfunction is prevalent among schizophrenia patients especially among women. This problem seems to be affected from both the disease and its treatment. The high prevalence and the interference with quality of life combine to make sexual dysfunction an important area for clinical assessment and appropriate intervention in the community management of schizophrenia.
No conflict of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
