
Research Article | DOI: https://doi.org/10.31579/2641-5194/007
Department of Pharmaceutics, Jangaon Institute of Parmaceutical Sciences
*Corresponding Author: Stalin reddy Challa, Department of Pharmaceutics, Jangaon Institute of Parmaceutical Sciences, Jangaon,India.
Citation: Stalin reddy Challa, Prasad Garrepally, Gastric ULCER Prevention by Lansoprazole., J. Gastroenterology Pancreatology and Hepatobilary Disorders. 3(1). DOI: 10.31579/2641-5194/007
Copyright: © © 2019 Stalin reddy Challa. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November -0001 | Accepted: 22 December 2018 | Published: 02 January 2019
Keywords: microspheres; lansoprazole; hydroxypropyle methyle cellulose; ethyl cellulose; double emulsion solvent evaporation method; FTIR;SEM; DSC
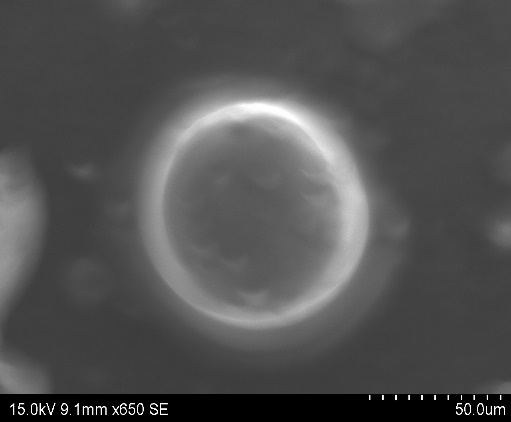
The objective of the current investigation is to formulate ethyl cellulose and hydroxypropyle methyle cellulose based sustained release microspheres, containing lansoprazole as model drugs. lansoprazole is type II anti-ulcer agent when administered shows synergetic effect in their action. Microspheres were prepared by W/O/O double emulsion solvent evaporation method with different stabilizer concentration and at different speeds of emulsification while maintaining constant amount of lansoprazole. Drug excipient compatibility study was performed prior to formulation development and only compatible excipients were used in the fabrication of microspheres. Prepared microsphere formulations were characterized by percentage yield, particle size analysis, entrapment efficiency, invitro release behavior, differential scanning colorimetry (DSC) and scanning electron microscopy (SEM). SEM studies showed that the microspheres were spherical with rough surface morphology. The drug loaded microspheres showed 10.4-57.9% entrapment capacity for lansoprazole and The invitro release profile showed a slow and steady release pattern for lansoprazole. A 95-98% was releases within a period of 12 hrs . The drug release was found to be diffusion controlled mechanism. The n value of Korsmeyer Peppas equation indicated non Fickian type of diffusion.
Sustained Release Formulation
For decades an acute or chronic illness is being clinically treated through delivery of drugs to the patients in form of some pharmaceutical dosage forms like tablets, capsules, liquids, creams, pills, aerosols, injectable, and suppositories with their main discrepancy to maintain drug levels within the therapeutic range. However, these conventional dosage forms have some drawbacks. Multiple daily dosing is inconvenient to the patient and can result in missed doses, made up doses and patient incompliance with the therapeutic regimen. When conventional immediate release dosage forms are taken on schedule and more than once daily, there are sequential therapeutically blood peaks and valley associated with taking each dose. It should be emphasized that the plasma level of a drug should be maintained within the safe margin and effective range. For this, proper and calculated doses of the drug need to be given at different time interval by conventional dosage form.1
This is possible through administration of conventional dosage form in a particular dose and particular frequency to provide a prompt release of drug. Therefore to achieve as well as to maintain the concentration within the therapeutically effective range needed by the treatment by repeated administration a day, results in a significant fluctuation in a plasma drug level, leads to several undesirable toxic effects, and poor patient compliance.2The loopholes of the conventional dosage forms lie in their inability:
Controlled drug delivery systems have been introduced to overwhelm the drawback of fluctuating drug levels associated with conventional dosage forms. Various terms like 'smart', intelligent', 'novel', therapeutic have been assigned to controlled release systems.
The following materials of Pharma grade or the best possible Laboratory Reagent grade were used as supplied by the manufacturer.
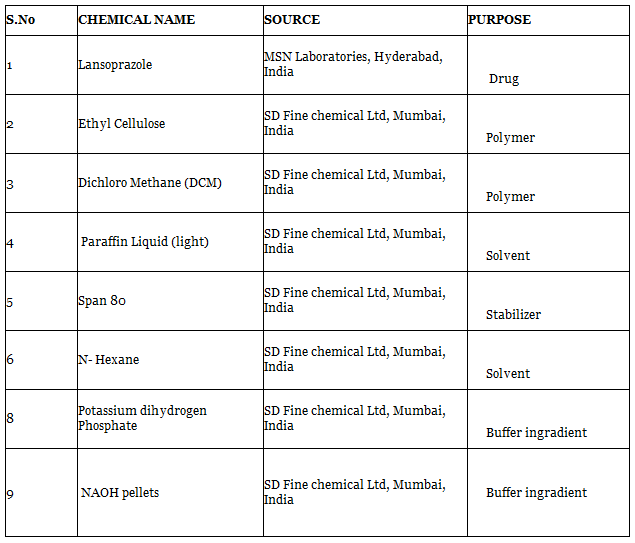
Lansoprazole belongs to class of antisecretory compounds, the substituted benzimidazoles that donot exhibit antocholinergic or histamine H2 receptor antagonist properties but rather supress gastric acid secretion by inhibition of the H+, K+ ions.
Lansoprazole has been charecterised as a gastric acid pump inhibitor in that it blocks the final step of acid production. This effect is dose related and leads to inhibition of both basal and stimulated gastric acid secretion irrespective of the stimulus.
Preparation of buffer pH 6.8
50ml of the potassium dihydrogen phosphate (0.2M) was placed in 200ml volumetric flask and to it 22.4ml of sodium hydroxide solution (0.2M) was added and the volume was made upto 200ml with distilled water.
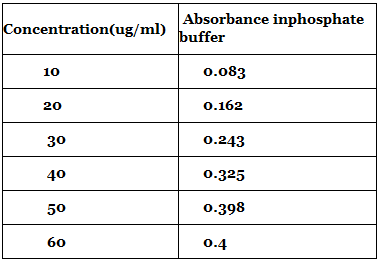
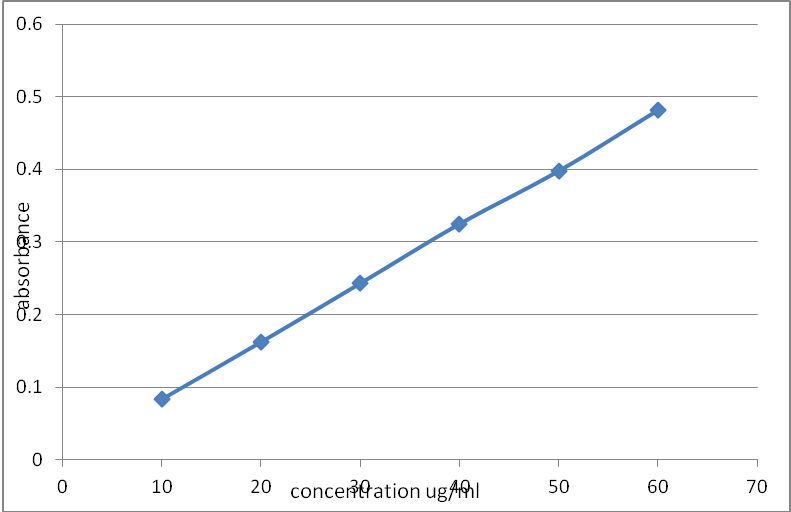
Preparation of standard solution of lansoprazole:
Procedure: Accurately weighed 100 mg of lansoprazole drugwas dissolved in 100 mL of (Conc. 1000 µg/mL). From this solution, 10 mL was pipetted out into 100 mL volumetric flask and volume was made up to with methanol (Conc. 100 µg/mL). Further 10ml aliquot was taken from this solution (100μg/ml) and diluted to 100ml with methanol to give 10μg/ml standard solution of drug.
Similarly, standard stock solution was prepared in phosphate buffer pH 6.8 and methonol.
Preparation of microspheres
For the preparation of microspheres the double emulsion method was used as suggested by Rama Rao et al. (2005) with slight modifications. The polymer was dissolved in a mixed solvent system (MSS) of acetonitrile and dichloromethane. To this polymer solution glipizide was added and mixed. Then metformin was dissolved separately in 3 ml of distilled water and added to the polymer solution while stirring to form a primary emulsion. This primary emulsion was stirred at 450 rpm for 15 min using a mechanical stirrer. Then, this w/o emulsion was poured into liquid paraffin containing Span180 as the surfactant. This was stirred using a mechanical stirrer for 3 h, for the complete evaporation of the solvent. 10 ml of n-hexane was added as the non solvent after 2 h of the stirring process. 47
Treatment and randomization
All patients who met the inclusion and exclusion criteria received a 1 week course of antihelicobacter therapy containing lansoprazole 30 mg, amoxicillin 1 g and clarithromycin 500 mg, given twice daily. This was followed by treatment with lansoprazole 30 mg, given daily for 4 weeks. Repeat endoscopy was performed at the end of treatment to check for healing of ulcers and eradication of H. pylori using the methods described above. Patients with unhealed ulcers would be given 30 mg of lansoprazole daily for another 4 weeks. Patients who failed H. pylori eradication, defined as a positive rapid urease test or histology, would receive another 1 week course of triple therapy containing ranitidine bismuth citrate 400 mg, amoxicillin 1 g and metronidazole 400 mg, given twice daily. Patients with unhealed ulcers and two unsuccessful eradication treatments of H. pylori were taken out of the study.
In the present investigation an attempt has been made to formulate microspheres of lansoprazole by using biocompatible polymer like ethyl cellulose and hydroxypropyle methyle cellulose as carrier for sustained release. Microspheres were prepared by double emulsion solvent evaporation method. Prepared microspheres are subjected for characterization and evaluation studies.
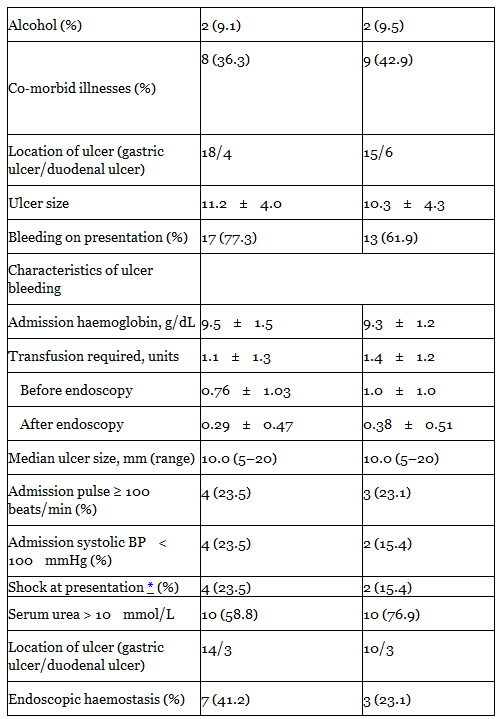
Among 102 patients screened during the study period, 45 were suitable for entry into the trial and were given a 1 week course of triple therapy, followed by treatment with lansoprazole. Reasons for exclusion are given in Figure 1. Two patients had persistent H. pylori infection after the first course of eradication therapy; they received the second antihelicobacter therapy and H. pylori was eradicated in both patients. Two patients had persistent ulcers after repeated anti‐ulcer treatment and were excluded from the study. The remaining 43 patients were given naproxen 750 mg daily and randomly assigned to receive lansoprazole treatment (n = 22) or no treatment (n = 21).
PREFORMULATION STUDIES
Preformulation study for lansoprazole has been performed to know the drug physical properties so as to design it to a suitable formulation.
SURFACE MORPHOLOGY BY SEM

From the study it is evident that promising sustained release microspheres of lansoprazole may be developed by W/O/O double emulsion solvent diffusion technique by using ethyl cellulose and hydroxyl prople methyle cellulose polymer.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
