
case report | DOI: https://doi.org/10.31579/2690-4861/485
1Internal Medicine Department Corewell Health Dearborn.
2Rollins School of Public Health, Emory University.
3Department of Hematology and Oncology, Corewell Health Dearborn.
*Corresponding Author: Antoine Egbe, Internal Medicine Department Corewell Health Dearborn.
Citation: Antoine Egbe, Niharika Ikkurthy, Khurram Arshad, Hussein Gaith, Ahmed Subahi, et al, (2024), Gastric Outlet Obstruction as the Presenting Sign of Duodenal Adenocarcinoma, International Journal of Clinical Case Reports and Reviews, 18(1); DOI:10.31579/2690-4861/485
Copyright: © 2024, Antoine Egbe. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 June 2024 | Accepted: 17 June 2024 | Published: 24 June 2024
Keywords: duodenal adenocarcinoma, gastric outlet obstruction, gastrointestinal malignancy
Introduction
Duodenal adenocarcinomas (DA) are rare cancers, that represent less than 1% of gastrointestinal cancers. Patients typically present with weight loss, nausea/vomiting, and jaundice.
Case presentation
In our 58-year-old lady, her inability to tolerate any food, plus associated incessant nausea/vomiting prompted her to report to the emergency department. During her hospital stay, esophagogastroduodenoscopy, endoscopic ultrasound and CT scan of the abdomen revealed that she had a duodenal mass complicated by duodenal stricture. Pathology revealed that the duodenal mass was indeed a duodenal adenocarcinoma. CT of the chest and abdomen revealed possible metastases to the lungs and liver.
Conclusion
In older patients with symptoms that bear a resemblance to a gastric outlet obstruction, it is necessary to rule out gastrointestinal cancer as a possible etiology of the symptoms.
We report the interesting case of a 58-year-old lady who presented with incessant nausea and vomiting to her primary care doctor. She was later found to have a gastric outlet obstruction secondary to a stage IV DA. Early diagnosis of small bowel tumors is difficult despite the significant progress that has been made in radiographic and endoscopic imaging. The presenting symptoms are vague and usually can mimic other gastrointestinal pathologies.
A 58-year-old lady with a past medical history of hyperlipidemia, essential hypertension, and a current smoker presented to the emergency department with reports of abdominal pain. She reports incessant nausea for the last 2 weeks which has consequently led to decreased oral intake for the last 2 weeks. She is unable to tolerate any food whether solid or liquid. She also reports being constipated and has only passed a very tiny amount of stool over the last couple of days despite having taken bisacodyl. She reports a 40Ibs weight loss over the last 3 weeks.
Physical exam upon arrival to the emergency department was unremarkable. Vital signs showed a BP of 118/78 mmHg, pulse 68bpm, temp 98.5 °F (36.9 °C) (Oral), a respiratory rate of 18cycles per minute, an oxygen saturation of 96%, and a BMI of 34.06 kg/m².
Lab work revealed she had
CT scan of the abdomen/pelvis (Figure 1) revealed a heterogeneous mass measuring approximately 5.8 x 3.4 x 5.6 cm involving the third portion of the duodenum and pancreatic head with subjacent enlarged lymph nodes. It also revealed several hypodense-like masses scattered throughout the liver
CTA chest (Figure 2) showed numerous pulmonary nodules.
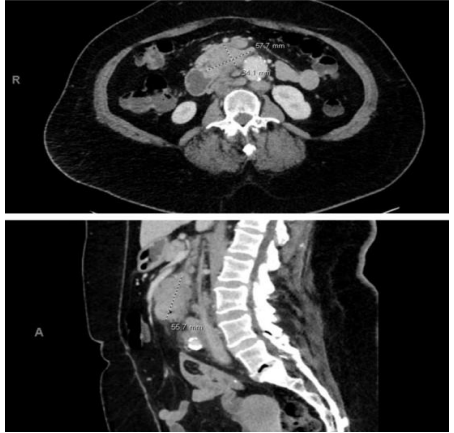
Figure 1: CT abdomen/pelvis showing 57.7mm mass in the third portion of the duodenum. In the transverse view, the mass measures 57.7mm x 34.1mm in size. It abuts the pancreas. The sagittal view shows a heterogeneous mass with irregular borders with the longest diameter of 55.7 mm.
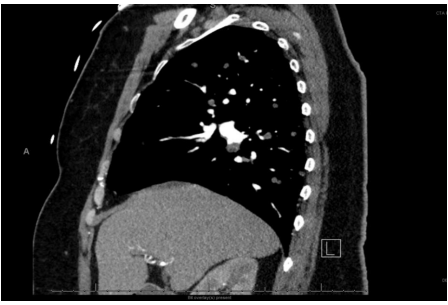
Figure 2: CT chest. Sagittal (Side) view of the Chest showing numerous pulmonary nodules.
The pulmonary nodules are of varying sizes with the largest being about 7mm in size. The nodules are believed to be secondary to metastasis from the primary duodenal mass.
With the above findings, the patient was scheduled for a liver biopsy. A right hepatic lobe biopsy was done on Day 2 of hospitalization. CA 19-9 was 61,408.96 U/ml(normal:0.0 -37.0 U/ml), while CEA was also elevated at 27ng/ml (normal: 0.0-3.0ng/ml). The biopsy revealed she had moderate to poorly differentiated adenocarcinoma that is cytokeratin 20 positive but CK7 negative.
The patient was subsequently admitted for dehydration, nausea, and vomiting. She had esophagus-gastro-duodenoscopy and EUS. It revealed a large duodenal mass in the second and third portions of the duodenum resulting in duodenal stricture. EUS showed normal pancreatic parenchyma and the pancreatic duct diameter was 1mm in the head and 1mm in the body. Due to the EGD findings, she was placed on a clear liquid diet and the plan was palliative duodenal stenting vs chemotherapy/radiation. EGD biopsy pathology report showed invasive adenocarcinoma involving the duodenum.
In collaboration with the medical team, the patient opted for chemotherapy and she was started on the FOLFOX regimen (folinic acid, fluorouracil, and oxaliplatin). The patient was also started on total parenteral nutrition since she was unable to tolerate any food. The patient received her first chemotherapy session, started feeling better, and was able to tolerate some liquid intake. She was then discharged, and she is supposed to follow/up with her oncologist for additional chemotherapy treatments
Discussion
Small bowel carcinomas are a rare form of cancer, contributing to only around 0.3% of the cancers in the US[1]. Of those, duodenal adenocarcinomas (DA) constitute approximately half[2]. Within the duodenum, 1-15% of the tumors occur in the first portion of the duodenum, 50-75% in the second portion, 14-33% in the third portion, and 5-17% in the final portion[3]. It is understood that small bowel adenocarcinomas follow the same pathologic path as colon cancer, arising in the presence of a combination of environmental and genetic factors[4].
In most cases, the diagnosis of duodenal adenocarcinoma becomes delayed due to nonspecific symptoms and signs[5]. Common initial presentations of duodenal adenocarcinoma are abdominal pain (39%), weight loss (35%), jaundice (25%), duodenal obstruction (25%), and upper GI bleeding (24%) [6]. These non-specific symptoms are usually attributed to more common benign conditions, as the rarity of duodenal adenocarcinoma makes it a more unlikely diagnosis. This results in an average diagnosis delay of 2-15 months, and poorer prognostic outcomes [7]. Surgery is the gold standard of treatment for the condition despite the poor outcomes still seen. Carcinoembryonic antigen (CEA) and carbohydrate antigen (Ca 19-9) are commonly tested. However, their prognostic or predictive value is unknown[8]. Similarly, the biomarkers CK20 and CK7 have shown variable positivity in detecting DA. This may be due to the mixed subtype tumors present. In the future, it may be useful to use a combination of markers such as MUC1, CK20, and CDX2 to attain a higher predictive value [9].
Gastric outlet obstruction is most commonly associated with H. pylori infection and peptic ulcers[10]. The incidence of gastric outlet obstruction due to H. pylori has decreased after the advent of proton pump inhibitors, and other benign causes have become more associated with GOO, such as strictures from chronic pancreatitis, surgical anastomosis scarring, or adhesions. As the rate of gastric outlet obstruction due to peptic ulcers is decreasing, small bowel tumors have become a more commonly considered cause of the condition. However, even in the cases where small bowel tumors are the cause of GOO, the lesions are usually asymptomatic[11].
In a similar case, gastric outlet obstruction was found as a presentation of duodenal adenocarcinoma, in a tumor arising from the duodenal bulb[11]. Other cases of DA present with similar vague symptoms, late into the disease [12].
As the causality of gastric obstruction is changing and the diagnosis of duodenal adenocarcinoma is often delayed, this unique presentation may help in further understanding of possible clinical pathways of DA and the variability of presentation. The prognosis of patients with DA remains poor, but a heightened suspicion of DA among physicians seeing these kinds of presentations may help hasten diagnosis and improve outcomes in the future.
DAs are rare gastrointestinal cancers that make up less than 1% of gastrointestinal malignancies. They typically present with vague symptoms hence it is of utmost importance for physicians to remain vigilant when clerking patients with uncontrollable nausea and vomiting sometimes associated with abdominal pain. The disease process is insidious and patients typically present when the malignancy has already spread to surrounding/distant organs.
Statement of ethics
Ethical approval is not required for this study following local or national guidelines.
All HIPAA identifiers(unique patient characteristics) have been removed.
Both written and verbal consent were taken from the patient.
The authors have no conflicts of interest to declare.
No funding was received before, during or after the production of this manuscript
Antoine Egbe, Niharika Ikkurthy, Khurram Arshad – Conception, design, and drafting of the manuscript
Hussein Gaith, Mariam Jamil, Ahmed Subahi and Wafa Ahmed— Conception, Critiquing, Reviewing and proofreading.
Faisal Musa— Conception, Editing, Proofreading and Reviewing of intellectual content.
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
