
Case Report | DOI: https://doi.org/10.31579/2693-2156/021
1 Radiology Department, Usmanu Danfodiyo University, Sokoto.
2 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
*Corresponding Author: Sule Muhammad Baba; Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule MB, Joshua GK, Dalha A, Ribah MM, Gidado S, et al. (2021) Gallstone Ileus in an Adult Male Patient: Computed Tomographic Findings and A Case Report. J Thoracic Disease and Cardiothoracic Surgery, 2(2); DOI: 10.31579/2693-2156/021
Copyright: © 2021, Sule Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 April 2021 | Accepted: 22 May 2020 | Published: 31 May 2021
Keywords: mechanical bowel obstruction; computed tomography; ileus; pneumobilia; cholelithiasis; gallstone impaction; terminal ileum; ileocecal valve
Gallstone ileus is a mechanical intestinal obstruction due to gallstone impaction within the gastrointestinal tract, and responsible for less than 1% of cases of intestinal obstruction.
This is a case of a 50-year-old male who was referred for computed tomography of the abdomen on account of abdominal pain, abdominal swelling and discomfort, restlessness, vomiting, constipation, easy fatigability, excess sweating and restlessness.
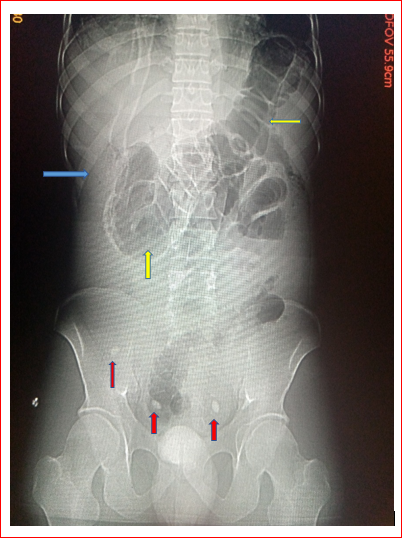
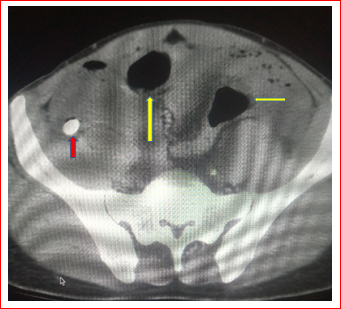
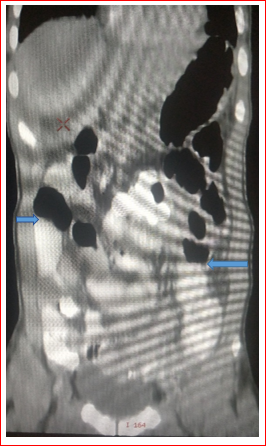
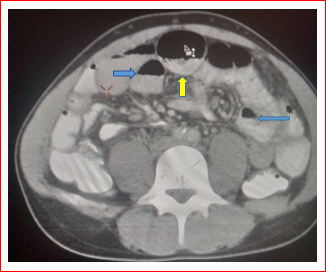
The scout image of the computed tomography (CT) demonstrated linear streaks and foci of radiolucency beneath and around the 10th and 11th anterior ribs on the right most likely pneumobilia. Air distended bowel loops were also demonstrated. Serial axial slides demonstrated an impacted calculus measuring about 30mm in widest transverse diameter in the right iliac region most probably the ileocecal valve region extending in to the cecum with associated dilated bowel loops showing multiple air-fluid levels raising a suspicion of mechanical bowel obstruction. The gall bladder measures about 50mm x 30mm in cranio-caudal and mediolateral diameter, with turbid contents and thickened walls of about 4mm most likely from cholecystitis. A diagnosis of mechanical bowel obstruction following an impacted calculus at the ileocecal valve was entertained; Gallstone ileus in a 50-year-old man.
The patient had surgical treatment, this comprised of exploratory laparotomy with entero-lithotomy, fistula repair and cholecystectomy. The patient did well post-operatively and was discharged home subsequently and advised on follow-up visits.
We present a case of mechanical bowel obstruction following an impacted gall stone at the ileocecal valve in a 50-year-old male patient.
Gallstone ileus is a mechanical intestinal obstruction due to gallstone impaction within the gastrointestinal tract, and responsible for about1-4% of cases of intestinal obstruction and predominantly occurs in females [1-3].
The most common site of gallstone impaction is the terminal ileum and the ileocecal valve, this follows a biliary enteric fistula following inflammation, the gallstones must measure about 2-2.5cm in diameter to cause obstruction [2-4].
Gallstone ileus has shown a constant incidence of 30-35 cases/1000000, admissions over a forty-five-year period and develops in 0.3-0.5% of patients with cholelithiasis [1,5,6]
Gallstone ileus is predominantly a geriatric disease, and as many as 80-90% of patients have concomitant medical illnesses which include hypertension, congestive cardiac failure, diabetes, chronic pulmonary disease and anemia [1, 7].
This condition has predilection for older female subjects with cholelithiasis over their male counterparts [7, 8].
Gallstone ileus has nonspecific symptoms and sign, most patient do have signs of acute cholecystitis preceding symptoms and signs of intestinal obstruction which may be partial or complete [1, 9, 10]. The main clinical presentation of gallstone ileus often depends on the site of impaction and most times include abdominal pain, distension, nausea, vomiting and constipation2.
Plain abdominal radiographs and computed tomography are important in establishing the diagnosis of gall stone ileus, though CT scan remains the gold standard with sensitivity and specificity rates of 3% and 100% respectively [2,3].
In 1941, Rigler et al [10] described four radiographic signs of gallstone ileus, these are; partial or complete intestinal obstruction, pneumobilia or contrast material in the biliary tree, an aberrant gallstone and change of position of the gallstone on serial films.
The presence of two of the three first radiographic signs has been considered pathognomonic and found in about 20-50% of cases [1, 11, 12].
The study is aimed at demonstrating the computed tomographic features of gallstone ileus with mechanical obstruction.
Case Report
This is a case of a 50-year-old male civil servant who was referred from a health facility in the neighboring settlement for an abdominal computed tomographic scan on account of abdominal pain, abdominal swelling and discomfort, restlessness, vomiting, constipation, easy fatigability, excess sweating and restlessness. These were preceded by frequent history of right upper quadrant colicky abdominal pain and discomfort with occasional vomiting especially after fatty meals and milk containing feeds raising a suspicion of cholecystitis.
The patient appeared in painful distress, with tenderness over the right hypochondrial region and a positive Murphy’s sign, not pale, anicteric, acyanosed, mildly dehydrated, no finger clubbing and no pedal swelling.
The blood pressure was about 110/65mmHg, pulse rate was about 72beats per minute, the respiratory rate was 12 cycles per minute. The blood electrolyte, blood urea and blood creatine levels were also normal; with values of about 12milligram per deciliter and 1.1milligram per deciliter of blood for urea and creatine respectively. The packed cell volume was about 38%, the white blood cells were elevated and about 13500 white blood cells per microliter in favor of the lymphocytes having a count of about 6500 lymphocytes in 1 microliter of blood. The erythrocyte sedimentation rate was also normal and about 10 millimeters per hour. The liver function test was also normal for the patient’s age.
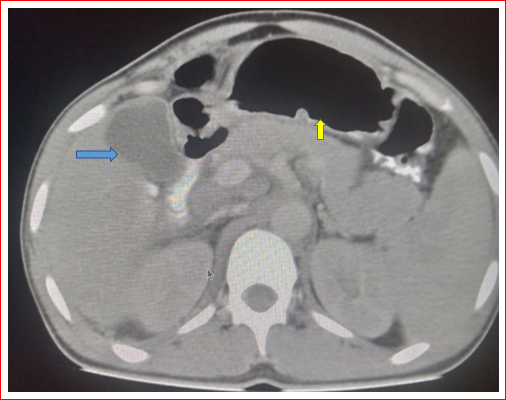
The scout image of the computed tomography (CT) demonstrated linear streaks and foci of radiolucency beneath and around the 10th and 11th anterior ribs on the right most likely pneumobilia. Oval calcific density opacities with surrounding lucency were also demonstrated in the region of the right iliac fossa most likely calculi within the bowel loops. Air distended bowel loops were also demonstrated (Figure 1). Serial axial slides demonstrated an impacted oval hyper-density measuring about 30mm in widest transverse diameter most likely a calculus in the right iliac region most probably the ileocecal valve region extending in to the cecum (Figures 2&3) with associated dilated bowel loops showing multiple air-fluid and air-contrast levels raising a suspicion of mechanical bowel obstruction (Figures 4&5). The other calcific density areas were noted within the bowel loops and appear not impacted. The gall bladder measures about 50mm x 30mm in cranio-caudal and mediolateral diameter, with turbid contents and thickened walls of about 4mm most likely from cholecystitis (Figure 6). No gall bladder calculus was demonstrated. Hepatomegaly with a liver span of about 159mm was also demonstrated (Figure 5). The pancreas was also demonstrated, it showed normal size and outline with no calculus within its ducts and no feature to suggest pancreatitis noted. A diagnosis of mechanical bowel obstruction following an impacted calculus at the ileocecal valve was entertained; Gallstone ileus in a 50-year-old man.
The patient had surgical treatment, this comprised of exploratory laparotomy with entero-lithotomy, fistula repair and cholecystectomy. The patient did well post-operatively and was discharged home subsequently and advised on follow-up visits.

Gallstone ileus is a disease of the elderly and more frequently seen among the female subjects [1-3], the index case is a 50-year-old conforming to that reported in the literature but happens to be a male patient contrary to the documented prevalence in the female gender.
Gallstone ileus is a rare disease and accounts for 1-4% of mechanical obstruction, prevalent in the elderly with associated high mortality rate, and difficult diagnosis, though early diagnosis however reduces the mortality [13]. The index case was however diagnosed early following imaging, with prompt institution of managing thereby conforming to this literature.
The most common site of gallstone impaction is the terminal ileum and the ileocecal valve, this follows a biliary enteric fistula following inflammation, the gallstones must measure about 2-2.5cm in diameter to cause obstruction [2-4]. The index case had an enteric calculus impacted at the ileocecal region/valve and measures about 30mm in widest diameter, thereby conforming to these literatures.
Most literatures document the preceding features of symptoms of cholecystitis in individuals with gallstone ileus [1,5,6], the index case also had features highly suspicious of cholecystitis conforming to that documented in the literature.
Patients presenting with features of gallstone ileus do occasionally have associated ailments like hypertension, diabetes mellitus to mention a few [1,7], the index case had no comorbidity invariance to these documented literatures.
The classical presenting features of abdominal pain and discomfort, abdominal distension and associated features of intestinal obstruction are those documented in the literature [1,2,9,10], the patient also presented with these features conforming to these literatures.
Plain radiograph and CT go a long way in establishing the diagnosis of gallstone ileus, though CT is the gold standard modality in establishing this diagnosis as mentioned by most researchers [2,3], the index case was also diagnosed following clinical presentation and CT scan of the abdomen conforming further to that documented in these literatures.
The classical radiographic features and finding of distended bowel loops, gallstone within the bowel lumen, pneumobilia and free intraperitoneal air with bowel loops having air-fluid levels are those documented in the literatures [2,3,10], these plain radiographic findings were also demonstrated in the index case conforming to that documented in the literature.
Rigler et al [10] described four radiographic signs of gallstone ileus, these are; partial or complete intestinal obstruction, pneumobilia or contrast material in the biliary tree, an aberrant gallstone and change of position of the gallstone on serial films. The presence of two of the three first radiographic signs has been considered pathognomonic and found in about 20-50% of cases [1,11,12]. The case under review had features of intestinal obstruction, pneumobilia, and presence of an impacted calculus at the right iliac fossa; ileocecal valve region, thereby conforming to these literatures.
Patients with gallstone ileus do have surgical intervention as a treatment modality as documented in the literature [2], the index case also had surgical operation; exploratory laparotomy with cholecystectomy as treatment option further conforming to most literatures.
Computed tomographic scan of the abdomen should be carried out on patients with high suspicious of gallstone ileus as it regarded the gold standard in establishing such diagnosis for prompt institution of management with subsequent reduction in morbidity and mortality associated with the condition.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
