
Research | DOI: https://doi.org/10.31579/2690-8794/230
General Surgeon ,Assistant professor, Department of Surgery , Medical Faculty , Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
*Corresponding Author: Ahmad Reza Shahraki, General Surgeon ,Assistant professor, Department of Surgery , Medical Faculty , Zahedan University of Medical Sciences and Health Services, Zahedan, Iran
Citation: Ahmad Reza Shahraki, (2024), Gall bladder perforation in a 15 days old infant, an extremely rare case: A case report ,Clinical Medical Reviews and Reports; 6(7): DOI: 10.31579/2690-8794/230
Copyright: © 2024 Ahmad Reza Shahraki, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 September 2024 | Accepted: 13 September 2024 | Published: 20 September 2024
Keywords: Perforated gallbladder; Pneumoperitonium ; Neonatal jaundice; Surgery,Infants
Neonatal perforated gallbladder is a rare and implausible surgical emergency. Pneumoperitonium and neonatal intestinal obstruction are the main clinical presentations. Many cases of neonatal perforated gallbladder had no clear pathology. Most proper treatment is cholecystectomy during formal exploration. Gallbladder perforation due to cholecystitis is usually seen in the elderly population but is uncommon among the pediatric population. Mortality rate can be as high as 26 % hence early diagnosis is vital. Management is mostly surgical as seen in the index case.
Our case is a 15 days old infants after falling from hand of parents more less 1 meter from earth admit with crying, abdominal sensivity and Us shows liquids and pneumoperitonium,in laparotomy we find rupture of gall bladder and do cholecyctectomy for her, and discharge her healthy.
Although perforated gallbladder is a rare entity and in most of cases does not cause pneumoperitonium, but perforated gallbladder should be taken in account of all cases of pneumoperitonium.
Spontaneous bile duct perforation in infants has been reported in the literature; however, gallbladder perforation in infants is extremely rare [2-3]. In the vast majority of cases, the underlying etiology still seems to be unknown, vascular and metabolic compromise were accused on its occurrence [3]. It has insidious presentations in the form of neonatal intestinal obstruction manifestations including billous vomiting, constipation, abdominal distention, abdominal tenderness and pneumoperitonium, making preoperative diagnosis challenging [4]. Perforated gallbladder is also uncommon in adults. It occurs in 2 % to 10 % of adult patients with acute cholecystitis, it could be diagnosed through computerized tomography, and on the other hand in neonates the diagnosis is elusive due to multiplicity of differential diagnosis [5]. With this data we report this case that shows it is a complications of infants.
Case presentation:
Our case is a 15 days old infants after falling from hand of parents more less 1 meter from earth one hours before and admit with crying, abdominal sensivity , nausea and vomiting . We start lab data and Us perform for her that shows liquids and pneumoperitonium,in abdomen. Laparotomy planed for her (figure1) we check liver,spleen,stomach and bowels and finally we find rupture of gall bladder(figure2) and do cholecyctectomy (Figure2) for her, After surgery we observe her and after2 days she starts water and then milk eating and discharge her healthy after3 days.

Figure1: Laparatomy
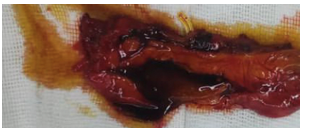
Figure2: Perforated gall blader
Rupture of the bladder is extremely rare in the newborns. Neonatal gallbladder perforation is rare, just 1.5 neonates every 1,000,000 live births [6-7]. The fundus is the least vascularized area supplied by blood, so it is the most susceptible area in the gallbladder to perforation [8]. Niemeier classified perforation in gallbladder into three categories in 1934: type I, acute perforation in the free peritoneal cavity which agreed with reported case; type II, subacute perforation with abscess formation; and type III, chronic perforation with fistula formation between the gallbladder and other organs [9-10]. Open cholecystectomy is the treatment of choice in this condition where some surgeons preferred a tube cholecystostomy [11-12]. Surgical exploration and cholecystectomy was done in this case with no intraoperative complications [13-14]. Gallbladder perforation due to cholecystitis is usually seen in the elderly population but is uncommon among the pediatric population. Mortality rate can be as high as 26 % hence early diagnosis is vital. Management is mostly surgical as seen in the index case [15]. Traumatic gallbladder perforations are exceeding rare and consist of only 1.9 to 2 % of all abdominal traumas [16-17]. The diagnosis is made through the clinical presentation, with patients presenting with localized or diffuse abdominal pain owing to biliary peritonitis and often diagnosed intra-operatively as seen in our case and most cases of GBP published [18]. Imaging modalities include USS and abdominal CT scans which are more sensitive as confirmed in the index case. More recently, contrast-enhanced ultrasound (CEUS) has been developed with a diagnostic accuracy for detecting solid organ injuries comparable to that of CT-scans, and has the capability of giving a more detailed description of traumatic cases [16]. Other modalities include Magnetic Resonance Cholangiopancreatography (MRCP) and drip-infusion cholangiography (DIC-CT) depending on the availability. Most cases are managed according to the cause, mostly through a surgical approach than conservative as a means of clearing the biliary peritonitis as well as cholecystectomy as seen in our case. Moving forward in medicine, the use of artificial intelligence (AI) will aid clinicians to detect pathologies more accurately and hence come up with an accurate diagnosis, therefore, avoiding delays in management. Currently, the use of robotic surgery is rising to perform surgeries like cholecystectomy and microsurgery. This benefits both surgeons and patients, however, challenges include projecting an overlay on markerless deformable organs and tissue deformation therefore sensors and algorithms need to be advanced and updated regularly [19]. Patients diagnosed with acalculous cholecystitis can be managed conservatively with analgesics and antibiotics and close monitoring of clinical symptoms and signs [20].
Neonatal perforated gallbladder is a rare and implausible surgical emergency. Pneumoperitonium and neonatal intestinal obstruction are the main clinical presentations. Many cases of neonatal perforated gallbladder had no clear pathology. Most proper treatment is cholecystectomy during formal exploration [1]. Gallbladder perforation although rare, but a life-threatening clinical condition with high mortality and should always be suspected in patients with acute abdomen, early diagnosis via imaging modalities and early management prompted to reduce ongoing morbidity and enhance recovery [15].
Highlights:
•The proportion of occurrence of gallbladder perforation is very rare
•No specific pathology is cause of perforation of gallbladder
•Pneumoperitonium is one of most important signs of gallbladder perforation.
•Gallbladder perforation is classified into three types according the site of perforation.
•Surgical excision of gallbladder is most proper surgical option in perforated gallbladder.
Declarations:
Ethical Approval and Consent to participate:
The content of this manuscript are in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate was granted by her parents.
Consent for publication:
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
- Availability of supporting data
It is available.
- Competing interests:
The author declares that they have no competing financial interests and nothing to disclose.
- Funding: There is no funding.
- Authors' contributions:
Ahmad Reza Shahraki is the surgeon of patient and writes this paper.
The author declares that they have no competing financial interests and nothing to disclose.
Acknowledgements:
Neonatal perforated gallbladder is a rare and implausible surgical emergency. Pneumoperitonium and neonatal intestinal obstruction are the main clinical presentations. Many cases of neonatal perforated gallbladder had no clear pathology. Most proper treatment is cholecystectomy during formal exploration. Gallbladder perforation although rare, but a life-threatening clinical condition with high mortality and should always be suspected in patients with acute abdomen, early diagnosis via imaging modalities and early management prompted to reduce ongoing morbidity and enhance recovery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
