
Research Article | DOI: https://doi.org/10.31579/2578-8868/350
1Department of Neurosurgery, Section of Pediatric Neurosurgery, University of Ulm, Germany.
2 Department of Neurosurgery, Bezirkskrankenhaus Günzburg, Germany.
*Corresponding Author: Stefanie Deininger, MD, Department of Neurosurgery, Bezirkskrankenhaus Günzburg, Germany.
Citation: Stefanie Deininger, Marie Schuler-Ortoli, Christian Rainer Wirtz, Aurelia Peraud, (2025), Functional Outcome after Fatty and Tight Filum Sectioning in a Diverse Cohort of Children with Tethered Cord Syndrome, J. Neuroscience and Neurological Surgery, 17(1); DOI:10.31579/2578-8868/350
Copyright: ©, 2025, Stefanie Deininger. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 23 December 2024 | Accepted: 08 January 2025 | Published: 31 January 2025
Keywords: tethered cord; fatty filum; myelomeningocele; occult spinal dysraphism; spina bifida
Background: Tethered cord syndrome (TCS) encompasses a spectrum of conditions, from severe dysraphic disorders to milder forms like occult tethered cord. This study aims to evaluate the functional outcomes following surgical de-tethering in a pediatric population with TCS caused by a fatty or tight filum, including those with complex developmental anomalies.
Material and Methods: We conducted a retrospective analysis of 58 pediatric patients who underwent surgical de-tethering between January 2018 and February 2024. Data was collected on motor function, bladder and bowel dysfunction, and other preoperative symptoms. Functional outcomes were assessed via clinical exams, neurophysiological testing, and urodynamic studies.
Results: The cohort had a mean age of 5.5 years at surgery, with a follow-up period averaging 1.8 years. Preoperatively, 79.3% of patients presented with neurogenic bladder and 56.9% with bowel dysfunction. Significant improvements were observed in bladder function, with 26.1% of patients showing improvement and 73.9% maintaining stable function (p=0.04). Children with developmental anomalies, who had a higher incidence of bladder and bowel dysfunction, showed notable improvement, with 66.7% demonstrating motor function recovery and 100% achieving pain relief. No worsening of symptoms was noted during follow-up, and no cases of re-tethering were observed within the follow-up period.
Conclusion: Surgical de-tethering for TCS in children, including those with complex developmental anomalies, is safe and results in marked improvements in motor function, pain, and bladder control. Long-term follow-up is necessary to monitor potential re-tethering, particularly in patients with complex conditions. The results support a proactive approach to surgery, irrespective of the severity of preoperative symptoms.
Tethered cord syndrome (TCS) encompasses a wide range of conditions, from severe dysraphic disorders like meningomyelocele and lipomeningomyelocele to milder forms such as occult tethered cord [1,2]. In the latter, patients may present with only external stigmata, while imaging reveals a tight or fatty filum and/or a low conus position (typically below L2). Regardless of the form, TCS is frequently associated with developmental comorbidities, such as complex anorectal and urogenital malformations [3,4].
Clinically, patients often present with progressive sensory and motor deficits in the lower limbs, alongside cutaneous, urological, and musculoskeletal abnormalities [5,6,7,8]. Research suggests that the traction on the spinal cord causes hypoxia and ischemia, leading to metabolic disruption and neuronal damage [9,10,11,12]. Symptom severity is thought to correlate with the extent of these metabolic disturbances [13,14]. However, postoperative improvement rates vary significantly, ranging from 10% to 90% [7,8,15]. While many studies have reported significant improvement in symptoms following surgery, long-term outcomes are inconsistent [6,7,16,17]. Some patients experience symptom recurrence, while others see little benefit from the procedure. Additionally, postoperative complications, including infections, cerebrospinal fluid leaks and re-tethering have been reported [6,18,19,20, 21].
There is a particular lack of outcome data for children with developmental comorbidities following TCS release [3]. These children often present with pre-existing bladder and bowel dysfunction, complicating the assessment of surgical impact. Some have undergone prior pull-through surgeries for anal atresia, while others manage their conditions with a stoma or self-catheterization. Given these complexities, the effect of TCS release on this subgroup remains uncertain.
This study examines functional outcomes and the disease spectrum in children with tethered cord caused by fatty or tight filum, based on a diverse retrospective cohort from a high-volume pediatric neurosurgery unit.
The study protocol was approved by the local ethics committee (protocol #17-504 and protocol #202/20). Written informed consent for the surgery was given by all parents/patients.
All patients undergoing surgical de-tethering for fatty/tight filum at our institution from 01/2018 from 02/2024 were included. Two patients got external de-tethering by the same staff surgeon and follow-up at our institution. Routine follow-up consisted in patient (and/or parent) interview, clinical exam, neurophysiological and urodynamic testing [8,18].
The data analyzed included gender, age at the time of surgery, and preoperative symptoms related to TCS. These symptoms encompassed motor function disturbances: degree of paresis, gait ataxia, ambulation ability, and results from neurophysiological tests such as somatosensory evoked potentials (SEPs) and, if performed, motor evoked potentials (MEPs), bladder function (urodynamic findings including bladder capacity, compliance, post-void residual volume, frequency of urination, catheterization frequency if applicable, incidence of urinary tract infections, and presence of urge or stress incontinence), bowel function, back pain, as well as the type and severity of foot or spinal deformities. Additionally, the presence of associated developmental disorders or genetic alterations. Each diagnosis was confirmed through lumbar magnetic resonance imaging (MRI) in conjunction with clinical and electrophysiological findings (exemplary illustration is provided in figure 1A and 1B).
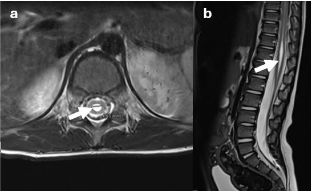
Figure 1A. Syringomyelia in a T2-weighted lumbar MRI
T2-weighted axial (a) and sagittal (b) MR image demonstrating a pointed conus medullaris with associated syringomyelia (arrows) with a maximum diameter of 5mm. The underlying reason is a tight fatty filum (arrows), which can be seen in the corresponding T1-weighted axial (c) as well as sagittal (d) MR images.
Figure 1B. Tight fatty filum in a T1-weighted lumbar MRI
The outcome measures included functional alterations of the symptoms and complications mentioned. The criteria for symptom improvement were defined as previously described [8].
The surgical management of the herein described cohort included the excision of any sinus tracts when present (n=3), as well as the removal of conus-lipomas (n=1) or dermoids (n=1). All patients underwent surgical de-tethering with continuous neurophysiological monitoring, including SEPs and MEPs, along with direct nerve root stimulation of the lower limb muscles and anal sphincters. The microsurgical procedure was performed through an ultrasound-guided, minimally invasive skin incision of approximately 1.5 cm and an interlaminar approach with undercutting of the ligamentum flavum. The dura was then opened in the midline over a length of 5 mm, secured with tag-up sutures on both sides, and CSF was allowed to drain. Subsequently, the filum terminale was identified among the nerve roots of the cauda equina using electrical stimulation, followed by coagulation and sectioning of the filum (figure 2 presents an illustrative example).

Intraoperative view of the tight fatty filum mobilized through a minimal dural opening before microsurgical transection.
Figure 2: Intraoperative view of a tight fatty filum
Quantitative analysis was conducted using GraphPad Prism 8, with data presented as proportions or mean with standard deviation (sd). Categorical data were analyzed using the chi-square test, and continuous data with paired or unpaired t-test. A p-value of ≤ 0.05 was considered statistically significant.
The cohort (shown in table 1) consisted of 58 patients with a mean age at surgery of 5.5 ± 6.2 years and a follow-up duration averaging 1.8 ± 2.0 years. The male-to-female ratio was 62.1% to 37.9%.

1 more than one may apply; Abbreviations: n, number; yrs, years; sd, standard deviation.
Table 1: Demographic characteristics
Of the entire cohort, 31 children (53.3%) presented with complex anorectal or urogenital malformations associated with tethered cord syndrome or additional syndromic disease. Among them, 13 exhibited caudal regression syndromes with 5 cases involving anal atresia, two children displaying a persistent urogenital sinus, and two identified with a VACTERL association. Additional four children were diagnosed with VACTERL (without caudal regression syndrome), including one case with anal atresia. One child showed a persistent urogenital sinus, and another presented with anal atresia (both without additional syndromic conditions). Other rare syndromic conditions included Trisomy 21 (n=2), Coffin-Siris syndrome (n=1), Kasabach-Merritt syndrome (n=1), and X-linked hydrocephalus (n=1) and 7 other various combined developmental disorders. Conus lipoma was present in 24.1% of patients, while syringomyelia was observed in 25.9%, and diastematomyelia in 3.4%. Chiari malformation and hydrocephalus were present in 3.4% and 5.2% of patients, respectively with 5.2% requiring a VP shunt. Children with developmental anomalies underwent surgery at 3.9 ± 3.2 years, compared to 7.4 ± 7.7 years for healthy children (p=0.025).
Of particular interest was a 15-year-old girl who had undergone postnatal MMC closure, decompression of a Chiari II malformation and a ventriculoperitoneal shunt in former history. On presentation, she showed deteriorating urodynamics, and imaging revealed a tight filum terminale with a lipoma at the filum terminale.
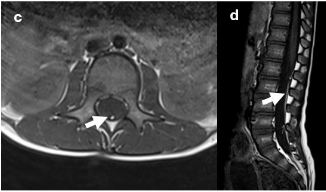
Symptomatic tethering was the indication for surgery in most children. Table 2 presents the preoperative symptoms in descending order of frequency in the overall cohort: the most prevalent symptom was neurogenic bladder, affecting 79.3% of patients, followed by bowel dysfunction (56.9%).

The proportions are shown relative to the number of children in the respective cohort. 1more than one may apply; Abbreviations: n, number. *p<0.05.
Table 2: Preoperative symptoms
One 7-year-old boy with genetically confirmed Saethre-Chotzen syndrome was operated due to symptomatic re-tethering 4 years post-surgery with worsening somatosensory evoked potentials and progressive bowel incontinence. His initial surgery involved transection of the fatty filum and Chiari I decompression.
Five patients were asymptomatic preoperatively diagnosed due to stigmata like dermal sinus (n=2), sacral dimple (n=1), lumbosacral hairy patch (n=1) and lumbar hemangioma (n=1). Besides fatty/tight filum MRI showed syringomyelia in one case and three conus lipomas. The dermal sinuses were additionally removed during surgery.
When comparing symptoms, patients with developmental anomalies showed a higher incidence of bowel dysfunction (80.6% vs. 29.6%, p<0.0001), whereas pain was more commonly reported among the healthy children (29.6% vs. 6.5%, p=0.02). Notably, all five asymptomatic patients were found exclusively within the healthy subgroup (p=0.01).
Figure 3 illustrates the functional improvements across all symptoms, highlighting the substantial postoperative recovery in pain and motor function. Of the children with developmental anomalies, 66.7% showed significant improvements in motor impairments, while 100% achieved complete pain relief. In contrast, 75% of healthy children also reported a reduction in pain symptoms.
Post-surgery, bladder dysfunction improved in 26.1% of patients (p=0.04), while 73.9% maintained stable symptoms. Two previously non-ambulatory patients gained the ability to walk. Foot deformities improved in 16.7% of cases, and bowel dysfunction in 18.2%, with most patients showing stable symptoms. Notably, no symptoms worsened during the follow-up period. Scoliosis was present in nine children (15.5%) preoperatively, though no follow-up data is available on its improvement. The five asymptomatic children remained symptom-free throughout the follow-up period.
1 more than one may apply; Abbreviations: n, number. *p<0.05
In summary, this descriptive analysis highlights the heterogeneity of the patient population and underscores the general efficacy and safety of de-tethering surgery in improving or stabilizing neurological function and associated symptoms in children with tethered cord syndrome due to fatty or tight filum. Children with TCS related pain had a 80% chance of clinical improvement. The fact that all preoperatively asymptomatic patients remained symptom-free throughout the follow-up period supports the potential value of the surgery as a prophylactic measure. As no patients experienced deterioration, it can be concluded that ultimately all patients benefited from surgery.
The demographic data from our cohort indicate that surgery was performed at a relatively early age, with an average age of 5.5 years. This reflects a clinical focus on intervening promptly after diagnosis to address symptoms and prevent progression. Young patients in our cohort demonstrated favorable outcomes, including improvement in bladder function and pain. These findings align with existing literature emphasizing the benefits of timely surgery in minimizing long-term neurological damage [7, 19, 22-26].
There are a few studies that have specifically examined neurological outcomes following de-tethering of an isolated fatty or tight filum [6, 7, 18, 19, 20, 21, 27-29]. While these studies generally suggest favorable functional outcomes, it is important to note that many exclude children with complex conditions, such as anorectal malformations and urogenital anomalies, limiting the applicability of these findings to a more vulnerable patient population. Additionally, healthy children, particularly those without complex conditions, tend to have better functional outcomes post-surgery [7, 30-33]. This underscores the challenges faced by managing children with more complex conditions, who are often excluded from studies but remain at higher risk for poorer outcomes.
Diagnosing TCS in young children, particularly those with developmental anomalies, remains a significant challenge. Symptoms such as pain and sensory deficits can be difficult to assess in this population, complicating the clinical decision-making process. Additionally, children with developmental anomalies may present with overlapping or atypical symptoms, further obscuring the diagnosis. The availability of objective diagnostic tools, such as neurophysiological monitoring and urodynamic studies, is often limited in young children with complex etiologies, underscoring the need for standardized assessment protocols. Addressing these diagnostic challenges is essential to ensuring timely and effective intervention [8, 18, 21, 22, 24, 25, 27].
Studies suggest that the outcomes of surgery vary depending on follow-up duration and patient comorbidities. Improvement or stabilization in bladder function is commonly reported [6, 19, 34-37], while motor dysfunction shows more variable rates of improvement [6-8]. However, bowel function appears to benefit less consistently, indicating that preexisting bowel dysfunction may limit the impact of the procedure [6-8, 34].
Apart from neurological outcome the re-tethering risk remains a notable concern, especially in children with more complex etiologies. A re-tethering rate of 33.6% was reported in children with complex conditions, such as those with previous anorectal or urogenital surgeries [20], compared to markable lower rates in children without these complications [18, 19, 27-29]. In our cohort, no cases of re-tethering were observed during the 1.8-year follow-up period. This aligns with findings from previous research, where re-tethering rates were low in younger cohorts [18, 19, 27, 28]. Besides etiology, early surgical intervention may reduce the likelihood of symptomatic recurrence, particularly when combined with meticulous surgical techniques and intraoperative monitoring [26, 30, 31, 37, 38]. However, long-term follow-up is essential to fully evaluate recurrence risks [16, 25, 26, 39, 40-44]. The largest published cohort of 99 patients following fatty filum surgery reported a re-tethering rate of 5.1
This study demonstrates that surgery for TCS in a pediatric population is safe, with minimal complications, and leads to marked improvements in motor function, pain relief, and bowel as well as bladder function, even among symptomatic patients from vulnerable groups with preexisting developmental anomalies. We recommend a proactive approach to surgery in children with TCS, regardless of the severity of their preexisting symptoms.
Conflict of interests
The authors declare no competing interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
