
Research Article | DOI: https://doi.org/10.31579/2639-4162/093
1 Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
2 Department of Opthalmology, Enugu State University Teaching Hospital, Enugu, Nigeria.
*Corresponding Author: 10.31579/2639-4162/093
Citation: Chukwubuike K. Emeka, Okoloagu Nkiruka, Anijunsi L. Patrick, (2023), Frequency of Intestinal Repair Leak Following Repair of Enteric Perforation in Children: A Single Surgeon’s Experience, J, General Medicine and Clinical Practice. 6(2); DOI:10.31579/2639-4162/093
Copyright: © 2023 Chukwubuike Kevin Emeka. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 February 2023 | Accepted: 06 March 2023 | Published: 07 March 2023
Keywords: children; frequency; intestinal; leakage; repair; typhoid perforation
Background: Enteric(intestinal) perforation causing peritonitis is a common surgical emergency in children and surgical repair is necessary. However, there may be complications accompanying the repair which may include leak from the repair site. The aim of this study was to evaluate the frequency of leak of intestinal contents after repair of enteric perforation.
Materials and Methods:
This was a retrospective study of children who were operated upon for intestinal perforation at the pediatric surgery unit of a teaching hospital in Enugu, Nigeria. The study covered a 5-year period. The information extracted included the age of the patient at presentation, gender, duration of symptoms before presentation, time interval between presentation and surgery, etiology of the perforation (intra-operative finding), operative procedure performed, post-operative complications (including evidence of repair leak), duration of hospital stay and outcome of treatment.
Results:
A total of 112 cases of enteric perforations were repaired during the study period. There were 70 (62.5%) males and 42 (37.5%) females. Typhoid intestinal perforation and primary closure/repair were the most common cause and operative treatment rendered to the patients respectively. Leakage of intestinal contents from the repair site occurred in about one-third of the patients. The overall outcome was fair; however, mortality happened in about 5 percent of the patients due to overwhelming sepsis.
Conclusion:
Surgical repair of intestinal perforation in children may be achieved by primary closure or a resection and anastomosis. Howbeit, this intestinal repair may be complicated by leakage of intestinal contents. Typhoid intestinal perforation was the most frequent cause of enteric perforation in the index study.
Enteric (intestinal) perforation causing peritonitis is a common surgical emergency in developing countries since time immortal [1]. Statistically, enteric perforation has been postulated to account for the fifth most common cause of abdominal emergencies due to the high incidence of typhoid fever [1]. Historically, enteric perforations have been found in Egyptian mummies [1]. The pathogenesis of intestinal perforation is explained by the fact that the disease extends through the full thickness of the intestinal wall. The etiologies of intestinal perforations could be from bacterial infections (eg., salmonella, tuberculosis); viral infection (eg., human immunodeficiency virus); fungal infection (eg., Entaamoeba histolytica). Other causes include drugs include NSAIDS such as ibuprofen. In low income countries, enteric perforation (mostly ileal) results as a complication of typhoid fever which is a public health problem in developing countries [2]. It is noteworthy to state that in some cases the cause of the intestinal perforation is not known and such situations are called non-specific intestinal perforation [3]. The consequence of intestinal perforation is the flooding of the peritoneal cavity by aerobic and anaerobic organisms causing peritonitis. The options of operative treatment of intestinal perforation may include primary repair/closure of perforation, primary ileostomy or resection and anastomosis [1]. Despite the various modalities of treatment, intestinal perforation is still associated with high morbidity and mortality. The aim of this study was to evaluate the frequency of leakage of intestinal contents after repair of enteric perforation. For the purposes of this study, only clinically obvious leaks were considered. What is the clinical benefit of this study? This study will help establish the guidelines for the optimal management of the children with enteric perforations.
This was a retrospective study of children who were operated upon for enteric perforation at the pediatric surgery unit of Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. The study covered a 5-year period, from January 2017 to December 2021. The diagnosis of typhoid intestinal perforation was made based on clinical features, investigations and intra-operative findings. On presentation at the children emergency room, the patients were resuscitated and stabilized using intravenous fluids and antibiotics. A nasogastric tube and urethral catheter were passed to decompress the upper gastrointestinal tract and monitor urine output respectively. Electrolyte imbalances, if any, were corrected. Following adequate resuscitation and under general anesthesia with endotracheal intubation, laparotomy was performed with the access through a transverse abdominal incision. The bowel perforation was identified and the surgeon closes the perforation primarily, performs an ileostomy or resection and anastomosis. The peritoneal cavity was cleaned out and the abdomen closed in layers. Patients who have had laparotomy for the same pathology at a peripheral hospital before referral to ESUTH for reoperation and patients with incomplete case records were excluded from this study. ESUTH is a tertiary hospital located in Enugu, South East Nigeria. The hospital serves the whole of Enugu State, which according to the 2016 estimates of the National Population Commission and Nigerian National Bureau of Statistics, has a population of about 4 million people and a population density of 616.0/km2. The hospital also receives referrals from its neighboring states. Information was extracted from the case notes, operation notes, operation register, and admission-discharge records. The information extracted included the age at presentation, gender, duration of symptoms before presentation, time interval between presentation and surgery, etiology of the perforation (intra-operative finding), operative procedure performed, post-operative complications (including evidence of repair leak), duration of hospital stay and outcome of treatment. The period of follow up was for 12 months. Ethical approval was obtained from the ethics and research committee of ESUTH. Statistical Package for Social Science (SPSS) version 21, manufactured by IBM Cooperation Chicago, Illonois, was used for data entry and analysis. Data were expressed as percentages, median, mean, and range
3.1. Patient’s demographics
A total of 112 cases of enteric perforations were surgically repaired during the study period. There were 70 (62.5%) males and 42 (37.5%) females which correspond to a male female ratio of approximately 1.7:1. The ages of the patients ranged from 3 to 14 years with a median of 10 years. The median duration of symptoms prior to presentation to the hospital was 7 days (5 – 8). The median duration from presentation to surgery was 2 days (range: 1 - 4). The mean duration of hospital stay was 14 days (range 10-27).
3.2. Etiology of the perforation (intra-operative finding)
The causes of the enteric perforation as found intra-operatively are shown in Table 1.

Table 1: Etiology of enteric perforation
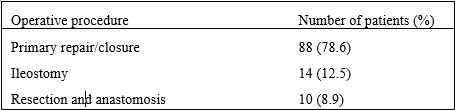
Table 2: Operative procedures carried out
3.4. Post-operative complications (including evidence of repair leak)
Among the 98 patients that had repair/anastomosis, 32 (32.7%) patients had leakage of intestinal contents from the repair site. This number excludes patients that had primary ileostomy. Other post-operative complications include surgical site infection in 15 (13.4%) patients, suture related complication in 6 (5.4%) patients and abnormal scars in 3 (2.7%) patients.
3.5. Outcome of treatment
Overall, all the patients achieved good recovery except for 6 (5.4%) patients that expired. The mortalities were due to severe sepsis and respiratory failure. Patients that had intestinal leaks were taken to theatre and secondary ileostomy performed.
Primary closure/repair of intestinal perforation is one of most performed surgical procedures in children [4]. The high incidence of intestinal perforations in low income ecountries could be related to lack of clean drinking water and poor sanitary conditions. Bowel perforation from any etiology is a serious abdominal emergency. Historically, since the late 1880s, appropriate treatment for intestinal perforation especially in typhoid intestinal perforation has remained controversial [5]. Surgery is the established modality of treatment of enteric perforation around the turn of the century [5]. However, it is worthy to note that there are reports of recovery of a few patients with enteric perforation who were treated only with antimicrobial agents. Currently, the recommended therapy for enteric perforation is always surgical which consists of simple closure and peritoneal irrigation [5].
In the present study, over a hundred enteric perforations were repaired. This number of enteric perforations is consistent with the report of Chalya et al [6]. This high number of intestinal perforations could be explained by the large number of typhoid intestinal perforations seen in developing countries like Nigeria and Tanzania. More male were affected by the enteric perforations. This male predominance is in line with the reports of other series on intestinal perforation [6, 7]. However, there is no established genetic basis for the male predilection and intestinal perforation is not gender related. The median age of the patients with enteric perforation is 10 years. The setting of the study and common predominant causes of enteric perforations in children may explain this median age. For instance, penetrating abdominal injuries from trauma may be more common in conflict areas while typhoid perforation from salmonella may be more in unhygienic food/water consumption and in untidy environments. Delay in presentation to the hospital is a frequent occurrence in low income countries. Poverty, ignorance and lack of awareness have been implicated in these delayed presentations. The clinical significance of this late presentation is that it impacts negatively on overall outcome of treatment. The two days lag period before surgical intervention is the interval required for resuscitation, stabilization and optimization of the patients. The entire duration of hospitalization refers to the overall time required for care, healing and recovery of the patients. This duration of hospital stay may be related to the etiology of the enteric perforation, premorbid condition of the patient and extent of operative procedure performed.
In the index study, typhoid intestinal perforation was the most common cause of intestinal perforation. Typhoid intestinal perforation is one of the surgical complications of typhoid fever. Typhoid fever is multisystem infection caused by the bacteria, Salmonella enterica serovar typhi and Salmonella enterica serovar paratyphi A and B which are transmitted through feco-oral route by ingestion of contaminated food and/or water [8]. The pathogenesis of typhoid intestinal perforation is the ulceration of the Peyer’s patches at the terminal ileum resulting in bowel perforation. This perforation leads to leakage of intestinal contents into the peritoneal cavity [9]. Chukwubuike et al reported intestinal perforation by salmonellosis as one of the most common causes of intestinal perforation in children in Enugu, Nigeria [10]. Prevention of typhoid infection can be achieved by provision of potable drinking water and proper waste disposal.
Tuberculous intestinal perforation was the second most common cause of enteric perforation in the current study. Tuberculous intestinal perforation results from intestinal involvement by mycobacterium tuberculosis. It is a public health problem in developing countries and its incidence is rising in western countries due to immigration and human immunodeficiency virus infection [11]. Abdominal tuberculosis can affect the peritoneum, intestine or lymph nodes and it occurs through reactivation of latent tuberculous infection or by ingestion of tuberculous mycobacteria (as with ingestion of unpasteurized milk or undercooked meat) [12]. Treatment of tuberculous intestinal perforation could be by primary closure or by resection and anastomosis. However, it is been postulated that primary resection of the affected intestine and anastomosis is the treatment of choice for tuberculous intestinal perforation [12].
Abdominal trauma is an infrequent occurrence in children except during times of civilian or military conflict. Blunt or penetrating abdominal trauma may cause intestinal perforation and/or can sever the vessels in the intestinal mesentery. It is worthy to note that occasionally intestinal perforation of unknown etiology can occur. Primary repair/closure of enteric perforation was the most frequently surgical procedure in our patients. The large number of typhoid intestinal perforations and the simplicity of primary closure may explain the numbers. However, in a background of gross peritoneal contamination where primary closure of enteric perforation is not advised, an enterostomy (eg., ileostomy) may suffice.
About one-third of the patients experienced a leak following repair of the enteric perforation. One study from Peshawar, Pakistan reported anastomotic leak in about one-fifth of their patients [4]. The cohort of patients recruited into a particular study may determine the frequency of the intestinal leak. For instance, there may be differences in anastomotic leaks in adults when compared to children. Again, the disease causing the problem may also affect the frequency of the perforation. The rate of anastomotic leak may also be related to the part of the bowel where the repair was performed. For instance, there may be more perforations in the small intestine when compared to the large intestine. The vascularity and consistency of the intestinal contents may also account for the disparities in the rates of leakage.
Surgical repair of intestinal perforation in children may require primary closure or a resection and anastomosis. Howbeit, this intestinal repair may be complicated by leakage of intestinal contents. Typhoid intestinal perforation was the most frequent cause of enteric perforation in the index study
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
