
Research Article | DOI: https://doi.org/10.31579/2641-0419/031
1* Department of Pathology and Blood Bank, Rawalpindi Institute of Cardiology, Pakistan
2 Executive Director, Professor of Medicine/ Cardiology Rawalpindi Institute of Cardiology, Pakistan
3 Rawalpindi Institute of Cardiology, Pakistan
*Corresponding Author: Arif Maqsood Ali, Assistant Professor of Microbiology, Department of Pathology & Blood Bank Rawalpindi Institute of Cardiology Rawalpindi, Punjab, Pakistan.
Citation: Arif M. Ali., Agha B. Hussain., Azhar M. Kayani. (2020) Frequency and antibiotic susceptibility of acinetobacter Baumannii in surgical site infections at Rawalpindi Institute of cardiology. J Clinical Cardiology and Cardiovascular Interventions, 3(2); DOI:10.31579/2641-0419/031
Copyright: © 2020 Arif Maqsood Ali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 November 2019 | Accepted: 16 December 2019 | Published: 06 January 2020
Keywords: acinetobacter baumannii; surgical site infections; coronary artery bypass graft; multi drug resistant; extended drug resistant
Acinetobacter is an important nosocomial pathogen to cause infections such as pneumonia, bloodstream infections, meningitis, wound and surgical site infections including flesh eating bacterium necrotizing fasciitis and urinary tract Infections. A. baumannii can be spread through direct contact with surfaces, objects and the skin of contaminated persons. Acinetobactter has acquired resistance to most of the antibiotics and can play havoc in hospital environment due to its ability to survive desiccation and in moist environment in the presence of disinfectants. Currently, there are 32 genospecies of Acinetobacter known. Among these, A. baumannii is the most important in the clinical context, since it is the most frequently isolated in nosocomial infections and the one associated with the highest mortality rate.
Objective
To find out the frequency of A. baumannii causing surgical site infections after cardiac surgery and best antibiotic options for its treatment in patients admitted in Rawalpindi Institute of Cardiology.
Materials and Methods
A retrospective study was carried out to find out bacterial cultures in admitted patients at Rawalpindi Institute of Cardiology with surgical site infections from July 2017 to August 2018. A total of 405 pus specimens collected from patients with suspected surgical site infections were tested for bacterial culture and antimicrobial susceptibility test. Patient profile was noted from centralized hospital data.
Results
Out of total 405 specimens 13 were culture positive for A. baumannii (3.2%). Ten isolates were Pan Drug Resistant (PDR).
Conclusion
A. baumannii infection although infrequent in our set up is mostly pan resistant. Infection control practices & surveillance are important to avoid its spread in hospitalized patients.
Surgical site infections (SSI) can involve any part of the anatomy after incision and surgical procedure. It can occur in skin, organs or implanted materials.[1] It commonly occurs within 30 days after an operation or under a special circumstance or within one year if an implant was placed and the infection appears to be related to the surgery. SSIs occur in 15% of all nosocomial infections among surgical patients. Post-operative SSI is the most common healthcare-associated infection in surgical patients, occurring in up to 5 percent of surgical patients. In the United States, between 500,000 to 750,000 SSIs occur annually.[2]
Although Staphylococcus, Streptococcus, Pseudomonas spp. commonly cause SSIs yet nosocomial SSI due to A. baumannii following Coronary Artery Bypass Graft (CABG) is a serious and costly complication. [3]
It commonly spreads in environmental surfaces, ventilators, dialysis machine, water sources, suction equipment, as a colonizer on skin and mucosal surfaces due to its resistance to commonly used antibiotics and disinfectants which make it difficult to eradicate from hospital environment. [5]
Multi drug resistant (MDR) A. baumannii have highest resistance among countries of South East Asia although these have been reported worldwide.[6] Mortality and morbidity rates are high due to its infection. There has been no study reported in SSI caused by this organism in cardiac hospitals of Pakistan.
Materials and Methods
A retrospective study was conducted from 1st July 2017 to 31st June 2018 at Pathology Department of Rawalpindi Institute of Cardiology (RIC), Rawalpindi Pakistan. It is a 272-bedded cardiac hospital located in Rawalpindi and provides both indoor and outdoor cardiac facilities to the patients of Rawalpindi, Islamabad and adjacent areas including patients from AJK and Northern areas.
All indoor and outdoor patients having SSI which were reported at RIC consecutively included in this study.
Specimens collected from patients having no history of surgery were excluded moreover specimens cultured other than surgical sites are also excluded.
Specimens from surgical sites including pus, tissues, fluids and aspirates were observed for both culture and antibiotic susceptibility.
Methods of Specimen Collection
Specimens were collected by standardized universal method by collecting the specimen before any dressing or cleaning procedure of the wound so as to avoid killing of the organism by using antiseptics. Sterile swab was taken by gently rotating it on the surgical wound site to collect exudate from the wound and was place into transport medium. Pus aspirates were also collected by standardized method. [7]
After receiving specimen in Microbiology laboratory, it was processed by inoculating it on blood, chocolate and MacConkey agar and incubated plates at 370C for 24 hours. The colony morphology typically showed is 1 to 2mm, non-pigmented, domed and mucoid colonies with smooth to pitted surfaces.[8]
Identification of gram negative rod was observed on microscopic examination by gram staining. Oxidase test was negative and confirmatory biochemical testing was done by using API 20E and NE (Biomerieux France) after incubation at 370C for 24 hours. Acinetobacter does not reduce nitrate which is its distinguishing feature from Enterobacteriaceae. Indole is negative, glucose is not fermented. Antibiotic susceptibility was done by Kirby Bauer Disc Diffusion Technique and results were interpreted as per CLSI guidelines M100-S27. [8]
Out of 405 pus cultures 13 (3.2%) were culture positive results for A. baumannii whereas 180 (44.4%) were culture negative and 212 (51.4%) were positive for other isolated organisms [figure 1].

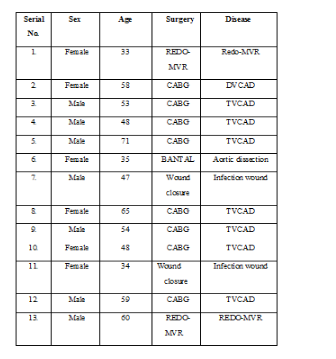
Out of total 13 positive samples 7 were male patients and 6 were female patients [Figure 4].

SSIs depend upon the type of surgery performed and the hospital environment. The prevalence of pathogen varies from place to place and hospital to hospital. The age distribution of all A. baumannii positive cases was above 30 and among them 8 were those having CABG while remaining 5 had different surgical procedures.
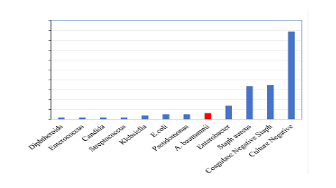
Out of 405 specimens 180 (44.4%) culture negative and other culture positive isolates were Coagulase Negative Staphylococcus70 (17.3%), Staphylococcus aureus 68(16.8%), Enterobacter spp. 28(6.9%), Escherichia coli 10(2.5%), Pseudomonas aeruginosa 10(2.5%), Klebsiella spp. 8(1.9%), Streptococcus spp.4(1.0%), Enterococcus spp.4(1.0%), Bacillus spp. and Diphtheroids 4(1.0%), Candida spp. 4(1.0%), Serratia spp. 2(0.5%)[Figure 5].
Out of 13 positive A. baumannii isolates 10 isolates were pan resistant and 3 isolates showed partial susceptibility to antibiotics. Among these, the first isolate was sensitive to Amikacin, Gentamycin, Ciprofloxacin, Chloramphenicol, Tazobactam/Piperacillin, the
Second isolate to Levofloxacin, Sulphamethoxazole, Meropenem, Imipenem,
Ciprofloxacin and the third isolate to Meropenem, Impanel, Amikacin,
Gentamycin.
A. baumannii has emerged as the causative agent of nosocomial infection due to increased use of invasive procedures, overuse of broad spectrum antimicrobials and prolonged duration of stay in the hospital. Development of resistance against antimicrobials is a major problem in the treatment of Acinetobacter infections. Although they are considered as pathogen of mild virulence, they can rapidly acquire resistance. [9]
A. baumannii is an opportunistic pathogen. It has a high incidence among
immunocompromised individuals, particularly those who have experienced a prolonged
Hospital stay. [10] It may colonize the skin as well as being isolated in high numbers from the respiratory, surgical and oropharynx secretions of infected individuals. [11] In recent years, it has been designated as a “red alert” human pathogen, generating alarm among the medical community, arising largely from its extensive antibiotic resistance spectrum. [12]
SSIs are one of the common post-operative complications. Apart from bacterial contamination of wound, various patient and environment related factors play role in development and outcome of SSIs. The present study is undertaken to study the frequency of of A. baumannii SSIs after cardiac surgery and its antimicrobial susceptibility. The prevalence of pathogen varies from place to place and hospital to hospital. [13]
Most of the isolates were considered as highly resistant to Imipenem, Amikacin, and Ampicillin/Sulbactam. MDR Acinetobacter spp. is defined as those isolates resistant to more than three classes of antibiotics (Penicillin’s and Cephalosporins, Fluoroquinolones and Aminoglycosides). An isolate was classified as extended drug resistant (XDR) when it was resistant to the three classes of antimicrobials described above (MDR) and shall also be resistant to Carbapenems. Pan drug resistant isolate define as that is resistant to Polymyxins and Tigecycline. [14]
CDC considers A. baumannii is a serious public health hazard due to its resistance to multiple antibiotics. [15]
SSI are still common in patients despite great advances in surgical techniques such as prophylactic antibiotics, disinfection and sterilization. Numerous studies have reported nosocomial infections after cardiac surgery to exceed 20%. The incidence of nosocomial infections was reported as 16% in the study by (Lomtadze et al) and 8.3% in the study by (Davoodi et al). [16]
Microbiological evidence suggests that 5% of open heart surgery patients develop nosocomial infections. The health authorities need to take measures at the ministerial and regional levels in order to reduce this under-reporting. [16]
A. baumannii has emerged as an important pathogen affecting any age group but inour study, it is most commonly found in patients between 30-70 years. In a previous study the most common age group effected by A. baumannii was between 42-68 years. [17]It is probably due to early onset of IHD in patients requiring Cardiac surgery.
A. baumannii was reported in surgical wound infection in Turkey and Saudi Arabiain 8.3% and 8.6% cases respectively. In another study reported in Saudi Arabia, the frequency of A. baumannii was 22.2% in wound infections. [18]
A. baumannii Infections were frequently isolated in males (53.8%) than females(46.10%) in our study. It is similar to a study in Saudi Arabia where out of 131 patients operated, 93 (71%) were males. The higher number of males may be due to the fact more males prone to have cardiovascular diseases than females that require surgery. [19]
A. baumannii infections are associated with major risk factors such as post-surgical, catheterization, extended hospital stays and prolonged antibiotic usage. A. baumannii isolated from normal skin and mucous membranes are reported to cause serious and sometimes fatal infections. [20]
Since, our study is based in a cardiac set up A. baumannii infections were found in cardiac patients having complications like Triple or Double Vessel Coronary Artery Disease (TVCAD) or (DVCAD), Redo-Mitral Valve Replacement Surgery (Redo- MVR), aortic dissection and infection wound so open-heart surgery was performed. Infection occurred in patients who were admitted to ICU for stabilization after a surgical procedure and required mechanical ventilation.
Infectious complications after cardiac surgery occur in 5% to 21% of cases.[21] Major infectious complications increase postoperative mortality by more than 5 times and prolong recovery. [22] Forty seven percent of these patients require more than 14 days in the hospital compared with 5.9% of patients without a major infection. [23]As a result, infectious complications often increase the cost of care. [24] However, infectious complications can be reduced with many simple interventions, by risk factor modification preoperatively to postoperative risk factor vigilance in the ICU.
In a review, the most common sites of infection reported were respiratory tract (45.7% - 57.8%), surgical site (27.7%), and catheters or devices (20.5%-25.2%) occurring perioperatively or within the first 12 months of surgery. [25]
In our study out of 405 specimens commonly isolated culture positive organisms are Coagulase Negative Staphylococcus 70(17.3%),Staphylococcus aureus68 (16.8%),Enterobacter spp. 28 (6.9%), Escherichia.coli 10 (2.5%), Pseudomonas aeruginosa 10(2.5%), Klebsiella spp. 8 (1.9%), Streptococcus spp. 4 (1.0%), Enterococcus spp. 4 (1.0%), Bacillus spp. and Diphtheroids 4 (1.0%), Candida spp. 4 (1.0%), Serratia spp. 2 (0.5%) alongwith A. baumannii (3.2%) (Fig. 3).
Similar to our study a bacteriological study of SSIs carried out in a tertiary care hospital at India concluded that overall frequency of SSI was 6.17%. Most common isolates were Staphylococcus aureus, Coagulase negative Staphylococci (CONS), E. coli and Pseudomonas aeruginosa. The frequency of Methicillin Resistant Staphylococcus aureus (MRSA) was 8.6%. The maximum frequency was among patients operated on emergency basis in surgical department. [26]
A. baumannii cause skin or soft tissue infections outside the military population leadingto 2.1% of ICU-acquired skin or soft tissue infections. A. baumannii was isolated from soldiers withopen tibia fractures in Iraq or Afghanistan war. [27]
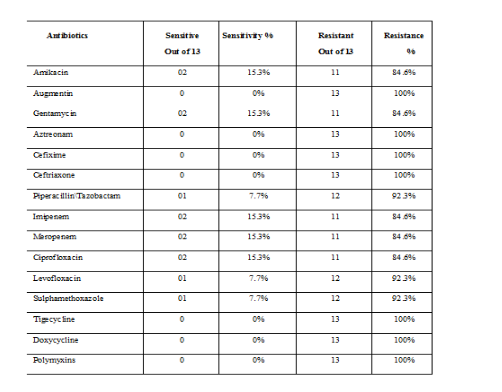
A. baumannii is a nosocomial pathogen and due to its resistance pattern, it is one ofthe leading cause of SSIs in our setup. Antibiotic susceptibility pattern of Acinetobacter spp. against various antibiotics in the present study showed (15.3%) susceptibility to Meropenem, Imipenem, Gentamicin, Ciprofloxacin & Amikacin whereas for Piperacillin/Tazobactam combination, Levofloxacin and Trimethoprim/ Sulphamethoxazole it was (7.7%). All isolated were resistant to Augmentin, Aztreonam, Cefixime, Ceftriaxone, Tigecycline, Doxycycline and Polymyxins (Table 2). A study from India reported antibiotic susceptibility of Acinetobacter species to Meropenem (86%), Piperacillin Tazobactam (76%), Amikacin (67%), Ampicillin/ Sulbactam (58%), Gentamicin (50%), Ciprofloxacin (49%), Ceftazidime (40%), Tetracycline (31%), Cotrimoxazole (29%), Ceftriaxone (21%) and Cefepime (18%).[28]
In another Study 52.5% cultures yielded significant growth and only 3% Acinetobacter spp. were isolated. Maximum (56.9%) isolates were obtained from pus/swab, followed by blood (13.1%) and urine (12.4%). Elderly age, being inpatients, longer duration of stay in the hospital, associated co-morbidity, and invasive procedure were found to be significant risk factors in the setup investigated. Out of 3% A. baumannii isolates, 54.7% were resistant to more than three classes of antibiotics MDR and 5.8% were resistant to all commonly used antibiotics PDR. Majority of the isolates were sensitive to Imipenem, Meropenem, and Piperacillin/Tazobactam, and showed resistance rates of 19%, 22%, and 23%, respectively.[29]
In a study from Brazil where in a six-month period, 1333 patients were admitted to the five ICUs included. The mean age of the participants was 53.2 years, and 59.4% were male. Most patients (98.4%) had previously taken antimicrobials and 68.2% had used two or more classes of antimicrobial drugs. The most commonly used drugs were 3rd-and 4th-generation Cephalosporins (71.4%) and Carbapenems (50.8%). [30]
Another study at Pakistan reveals that isolation rate of Acinetobacter was high from the respiratory specimens, followed by wound samples. Antibiotic susceptibility analyses of the isolates revealed that the resistance to Cefotaxime and Ceftazidime was the most common, in 710 (99.2%) specimens each, followed by the resistance to Gentamicin in 670 (93.6%) isolates, and to Imipenem in 651 (90.9%) isolates. However, almost all isolates were susceptible to Tigecycline, Colistin, and Polymyxins B. [31]
In an international study in ICUs, the Acinetobacter infection rate was 19.2% in Asia, 17.1% in Eastern Europe, 14.8% in Africa, 13.8% in Central and South America, 5.6% in Western Europe, 4.4% in Oceania and 3.7% in North America [32].
Global data reveals that multidrug-resistant A. baumannii is emerging as a common hospital-and community-acquired infection that is difficult to treat. It is a very resistant and aggressive organism that infects patients with weakened defences like ICU patients and those with invasive devices. [33]
It is important to notify multi drug resistant A. baumannii (MDR-Ab). For patients colonized or infected with MDR-Ab maximum isolation precautions require a private room and one to one nursing. Each patient with MDR-Ab needs dedicated equipment and universal precautions should be followed to attend patients with MDR-Ab.
The frequency of A. baumannii infections in our study is 3.20% in surgical site infections. SSI is more common in males (53.80%) than females (46.20%) and most often seen in CABG patients. Most of these isolates were pan resistant. In order to decrease the spread of A. baumannii infections and reduce its resistance, it is important to promote the rational use of antimicrobials, with implementation and monitoring of the Antibiotics Stewardship Program in hospitals. Hand hygiene and barrier nursing are important to keep the spread of infection in check.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
