
Case Report | DOI: https://doi.org/10.31579/2641-0419/196
1Associate Professor of Cardiology, Dayanand Medical College & Hospital – Unit Hero DMC Heart Institute, Ludhiana.
2Intern, Dayanand Medical College & Hospital, Ludhiana.
3Consultant physician, Dayanand Medical College & Hospital – Unit Hero DMC Heart Institute, Ludhiana.
4Professor, Department of medicine, Dayanand Medical College & Hospital – Unit Hero DMC Heart Institute, Ludhiana.
*Corresponding Author: Shibba Takkar Chhabra, Associate Professor of Cardiology, Dayanand Medical College & Hospital – Unit Hero DMC Heart Institute, Ludhiana.
Citation: Shibba Takkar Chhabra, Tripat Kaur, Gurleen Kaur, Rohit Tandon, Vandana Midha (2021) Fortuitious Diagnosis of Scimitar Syndrome in an Asymptomatic Adult. J. Clinical Cardiology and Cardiovascular Interventions, 4(14); Doi:10.31579/2641-0419/196
Copyright: © 2021 Shibba Takkar Chhabra, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 July 2021 | Accepted: 19 July 2021 | Published: 26 July 2021
Keywords: asymptomatic; adult; scimitar syndrome
Scimitar syndrome is a rare congenital anomaly seen as one of the components of congenital pulmonary venolobar syndrome. Simple and traditional investigation tools like CXR if interpreted with vigil can aid in prompt diagnosis and management of patients even in absence of clinical symptoms.
Scimitar syndrome is a rare congenital anomaly seen as one of the components of congenital pulmonary venolobar syndrome. It is a combination of pulmonary hypoplasia and partial anomalous pulmonary venous return (PAPVR) and occurs exclusively on the right side. The name ‘scimitar’ is derived from the curvilinear vascular pattern seen on chest x-ray due to the anomalous pulmonary vein coursing along the right side of the heart towards the diaphragm, resembling a ‘Scimitar’ or a Turkish sword. We report scimitar syndrome diagnosed after identifying this scimitar appearance on a routine chest x-ray done (CXR) in an asymptomatic embassy case.
A 27 year old healthy male presented to our outpatient department for health check-up as an embassy case. He was asymptomatic with no significant past or family history. General physical examination, cardiovascular and respiratory examinations were unremarkable. Routine CXR revealed a curvilinear pattern on right side of the heart (Figure 1).

EKG done revealed normal sinus rhythm with right axis deviation.
Transthoracic echocardiography (TTE) demonstrated dilated right atrium and right ventricle, mild tricuspid regurgitation and pulmonary artery systolic pressure of 30mm Hg. Transesophageal echocardiography (TEE) showed drainage of right upper and lower pulmonary veins into the inferior vena cava (IVC).
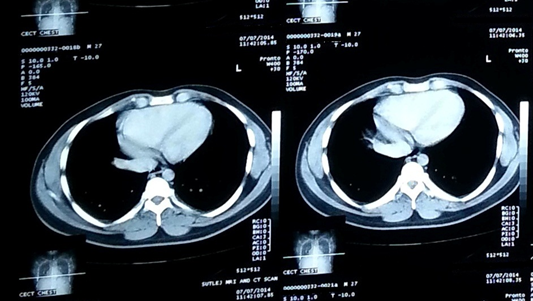
CT pulmonary angiogram was performed which revealed right upper and lower pulmonary veins draining into suprahepatic IVC, thus confirming scimitar syndrome (Figure 2).
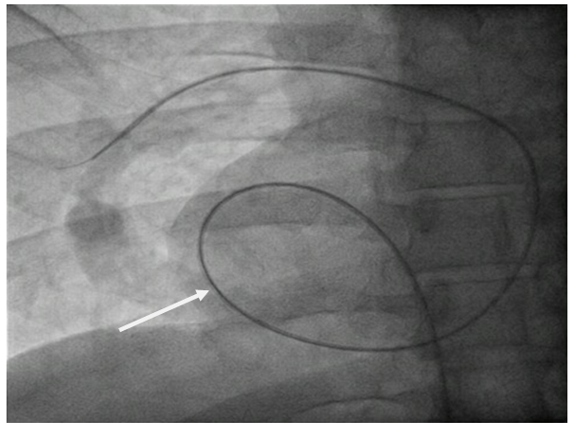
Cardiac catheterization was done which demonstrated scimitar vein and a significant step up in oxygen saturation in IVC above and below renal veins (Figure 3).
Mean pulmonary pressures were normal and Qp/Qs was 1.5. No associated anomalies were noticed. Since the patient was completely asymptomatic, he was managed conservatively.
Scimitar syndrome is a constellation of cardiopulmonary anomalies and accounts for about 0.5-1% of congenital heart diseases. It has an incidence of 1-3/1, 000, 00 live births [1, 2]. The exact cause is still not known. It is characterized by an anomalous pulmonary vein which usually drains into IVC (most common), right atrium or portal vein. Hemodynamically there is an acyanotic left to right shunt due to connection of pulmonary venous circulation and systemic venous circulation. The presenting features depend on the age of the patient with infantile form being worse than the adult form. In infancy it usually presents with cyanosis, poor growth, tachypnea, pulmonary hypertension and congestive heart failure. However adults have a more benign course [3] and may experience recurrent pulmonary infections, hemoptysis or exertional dyspnea. Common associations of this syndrome include atrial septal defect, ventricular septal defect, dextrocardia, bochdeleck hernia, horseshoe lung, hemivertebrae and pulmonary sequestration [4]. CXR is diagnostic and shows a small lung with ipsilateral mediastinal shift and an anomalous draining vein seen as a curvilinear shadow paralleling the right heart border in the shape of a Turkish sword or ‘scimitar’. It can be further confirmed by echocardiography and CT or MR angiography. Cardiac catheterization is done to identify the course of anomalous vein, measure the degree of left to right shunt, assess for pulmonary hypertension and to look for associated cardiac anomalies. Important differential diagnosis includes pulmonary sequestration, right middle lobe atelectasis and unilateral absence of pulmonary artery. Treatment primarily consists of surgical correction which includes direct anastomosis of the scimitar vein to the left atrium or reimplantation of the anomalous vein into the right atrium with baffle insertion to redirect the flow into left atrium. Indications for surgical correction include presence of left to right shunt exceeding 50% and lung sequestration with recurrent right sided chest infections [5]. We have reported the case of an asymptomatic adult with scimitar syndrome diagnosed incidentally on routine CXR. Simple and traditional investigation tools like CXR if interpreted with vigil can aid in prompt diagnosis and management of patients even in absence of clinical symptoms.
FUNDING: NONE
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
