
Case Report | DOI: https://doi.org/10.31579/2768-2757/138
1 Cirujano General. Residente de Cirugía Plástica y Reconstructiva, Servicio Oncológico Hospitalario Padre Machado Caracas. Venezuela.
2 Cirujano Plástico y Reconstructivo, Jefe de Servicio de Cirugía Plástica y Reconstructiva del Servicio Oncológico Hospitalario Padre Machado Caracas. Venezuela.
3,4,5,6 Cirujano Plástico y Reconstructivo, Cirujano Oncoplástico, Servicio Oncológico Hospitalario Padre Machado Caracas. Venezuela.
7 Cirujano Plástico y Reconstructivo, Fellow Cirugía Oncoplástica, Servicio Oncológico Hospitalario Padre MachadoCaracas. Venezuela.
*Corresponding Author: Juan Ricciardi V., Cirujano General. Residente de Cirugía Plástica y Reconstructiva, Servicio Oncológico Hospitalario Padre Machado Caracas. Venezuela.
Citation: : Juan Ricciardi V, Nilyan Rincón, Otto González, Carianda Ramírez, Natalia Solórzano, et al, (2024 Forrest Mastectomy and immediate Reconstruction Through Latissimus Dorsi Flap with Breast Implants and Contralateral Simetrization, Journal of Clinical Surgery and Research, 5(7); DOI:10.31579/2768-2757/138
Copyright: © 2024, Juan Ricciardi V. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 September 2024 | Accepted: 19 September 2024 | Published: 01 October 2024
Keywords: latissimus dorsi; reconstructive breast surgery; hybrid reconstruction
The demand for breast reconstruction is increasing constantly, which leads plastic surgeons to look for new methods to obtain a more natural and aesthetically pleasing appearance of the reconstructed breasts. The latissimus dorsi (LD) muscle has been adopted as one of the workhorse flaps for breast reconstruction.
Objective: Report a breast immediate reconstruction through a latissimus dorsi muscle flap with breast implants and contralateral simetrization.
Clinical Case: 47 years old female with a right ductal invasive breast carcinoma with a partial oncological response after neoadjuvant treatment and Forrest total right mastectomy and immediate reconstruction by the Plastic and Reconstructive service using a hybrid technique.
Discusion And Conclusion:Among all the surgical methods, modified mastectomy is adopted most commonly in China; however, it has been found to have negative psychological effects on women’s emotion and affects their quality of life. The latissimus dorsi (LD) flap is a commonly used technique in reconstructive surgery. It is an autologous tissue that can cover a large area, for defects due to trauma, wide excision, or tumors. It is one of the most commonly used flaps in reconstruction of small to moderate breast volumes. The latissimus dorsi muscle flap with breast implants and contralateral simetrization are both an excellent reconstructive alternative to the breast reconstruction after Forrest mastectomy defects in the same surgical time.
Breast cancer is the most common malignancy in women, with a global incidence of 2,088,849 new cases and 626,679 related deaths reported in 2018 [1] and according to the American Cancer Society, about 2,710 new cases of invasive breast cancer will be diagnosed in the United States in 2022. [2] The percentage of U.S. women who opted to undergo breast reconstruction after breast cancer was estimated at 43.3
Female 47 years old, without oncological antecedents, who reports the beginning of current illness 14 months earlier characterized by self-detected nodular mammary lesion between the upper mammary quadrants (12 o´clock) of the right breast with irregular edges, 5 x 4 cm non-mobile and attached to deep planes, so she went to a medical consultation where they request a mammography and bilateral breast ultrasound with a core needle biopsy who reports a ductal invasive breast carcinoma, immunohistochemistry reports Her2/neu (+++) so after the adequate stadification process she went first to a neoadyuvant treatment with a partial oncological response (50% lower lesion) and after that appropriate elective surgery was planned at the “Padre Machado” Oncological Hospitalary Service. Therefore, under general anesthesia, on the first surgical time the Breast surgery service it performs a right Forrest total mastectomy, on a second time immediate reconstruction by the Plastic and Reconstructive service through a latissimus dorsi flap with breast implants and contralateral simetrization using a superior pedicle mastopexy. Adequate postoperative functional and aesthetic results and continue follow up with an Oncology and Breast Surgery service.
Breast cancer is the most common malignancy for women. The treatment of choice for early-stage breast cancer is surgery. (5) Among all the surgical methods, modified mastectomy is adopted most commonly in China; however, it has been found to have negative psychological effects on women’s emotion and affects their quality of life. Therefore, it is vital to consider other surgical approaches such as breast reconstruction and oncoplastic conservation surgery. [6]
The latissimus dorsi (LD) flap is a commonly used technique in reconstructive surgery. It is an autologous tissue that can cover a large area, for defects due to trauma, wide excision, or tumors. [7] It is one of the most commonly used flaps in reconstruction of small to moderate breast volumes [8]
According to Sood R, Easow J, et al; [9] there are several specific indications for the latissimus dorsi flap (LDF). For autogenous breast cancer reconstruction, the LDF is first line for patients who are not candidates for the TRAM flap, due to previous abdominoplasty, prior TRAM, insufficient abdominal skin or fat, and high-risk comorbidities such as diabetes, obesity, or tobacco use. [9] Having relation with our case, because the patient had an abdominal hysterectomy antecedent by huge uterine myomas treatment.
In the other hand, according the skin pattern design of the island flap, the work of Ho Lee J, Yeop Ryu J, et al [7] describe that the vertical latissimus dorsi flap is applicable in all partial breast reconstructions, regardless of the region of defect. It also showed a statistically significant decrease in admission and operation times with higher patient satisfaction than the mini-LD flap technique, however have not relation with the latissimus dorsi technique of our case because was made with a classic pattern after a total mastectomy instead a partial one.
According Lu Li, Yue Yang, Wang Li et al [10] neoadjuvant chemotherapy is an accepted treatment option for patients with locally advanced breast cancer, and the use of a latissimus dorsi musculocutaneous flap for post-mastectomy reconstruction may improve the patients’ physical condition, having a strong relation with our case because the patient went to neoadjuvant treatment before the total mastectomy and the immediate reconstruction through the latissimus dorsi flap.
The demand for breast reconstruction is increasing constantly, which leads plastic surgeons to look for new methods to obtain a more natural and aesthetically pleasing appearance of the reconstructed breasts. For example, the work of Xun Ma J, Bi Li [11] describe a Latissimus dorsi muscle flap transfer through endoscopic approach combined with the implant after tissue expansion for breast reconstruction of mastectomy patients could effectively reduce visible scars, avoid the patch effect, while require short time for latissimus dorsi flap muscle harvest and present low incidence of complications. However, requires a huge aparatology, well trained center and training on minimal invasive reconstructive experience, a fact that have not relation yet in our country where we need to extend the plastic and reconstructive surgery programs in order to can learn and develop these complex techniques.
The latissimus dorsi muscle flap with breast implants and contralateral simetrization are both an excellent reconstructive alternative to the breast reconstruction after Forrest mastectomy defects in the same surgical time.
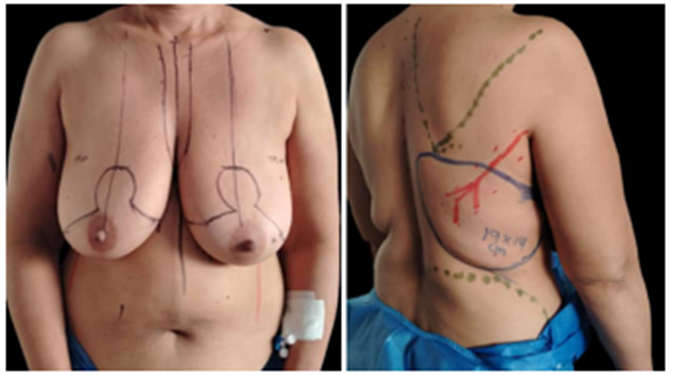
Figure 1.2: 1. Mastopexy bilateral pattern with a superior pedicle at the contralateral breast.
2. Latissimus dorsi muscle flap preoperative design.

Figure 3. New LDMF design with the patient in left lateral position at the operation room.

Figure 5. Result of the immediate right breast reconstruction through the latissimus dorsi muscle flap with breast implants and superior pedicle Mastopexy contralateral simetrization.

Figure 6: Result of the immediate right breast reconstruction through the latissimus dorsi muscle flap with breast implants and superior pedicle Mastopexy contralateral simetrization.
Plastic, Reconstructive and Oncoplastic Surgeons of the SOH Padre Machado, Caracas, Venezuela.
The author declare no conflicts of interest.
This research complies with the World Medical Association Declaration of Helsinki on medical protocols and ethics.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
