
Research | DOI: https://doi.org/10.31579/2640-1053/108
1 Neurosurgery Department, Mustapha Pacha University Hospital, Algiers, Algeria.
2 Neurosurgery department of Ali Ait Idir Health Hospital Establishment, Algiers, Algeria.
*Corresponding Author: K. Badache, Neurosurgery Department, Mustapha Pacha University Hospital, Algiers, Algeria.
Citation: K. Badache, N.habchi, F.Z Bendib, Kh Khalfi, N. Ioualalen, ET M. Djaafer. (2022). Follow up of Medulloblastoma’s Treatment Retrospective Study of 144 Cases. Cancer Research and Cellular Therapeutics. 6(2); Doi:10.31579/2640-1053/108
Copyright: © 2022 K. Badache, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 December 2021 | Accepted: 07 February 2022 | Published: 10 February 2022
Keywords: medulloblastoma,; metastasis; surgery; adjuvant treatment
Introduction: Medulloblastoma is the most common childhood primary CNS tumor, and treatment approaches have evolved over the past three decades. Despite recent improvements in cure rates, prediction of disease outcome remains a major challenge and survivors suffer from serious therapy-related side-effects.
Patients and Methods:
A retrospective study including 144 patients with medulloblastoma were performed at the Neurosurgery Department in Ait IDDIR Health Hospital Establishment between the period of January 2004 and December 2014. In each case, diagnosis was made clinically and confirmed radiologically and histo-pathologically. All patients were operated and received the adjuvant treatment
Results and discussion
Out of 144 patients, 63 (44%) patients were females and 81 (56%) were males. We have 59 cases who had age ranged from 05 months to 5 years, however, we had 85 cases who had more than 5 years ; we identified 29 (58%) children and 21 (42%) adults. Clinical manifestations of meduloblastoma vary widely according to the location. The vermis is the main location of the child with 95%. The most frequent clinical manifestations found were Intracranial hypertension syndrome and static and kinetic cerebellar syndrome, 98% patients had intracranial hypertension at diagnosis: 1,4% with engagement (2 cases) and 0,7% with coma(01 case).A ventriculo-peritoneal shunt was performed in all patients, 01 case after surgical removal. The most common complications were as follows: Meningitis ( 0,2%),ventriculitis (0,2%), CSF leakage (0,4%), post-surgical hematoma (0,2%), Shunt dysfunction ( 0,6%), aggravation of the cerebellar syndrom (0,4%), affection of mixed nerves ( 0,2%) and cerebellar mutism (0,4%). Tumor architecture was classified as classic (Grade II) and desmoplasic. We had T2M0 in 41(28,47%) cases, T2M2 in 2 (1,38%)cases ,T3aM0 in 98(68%)cases,T3bM3 in 2(1,38%) cases and T3bM4 in 1 (0,7%)case. During follow-up period, recurrence occurred in 15 (10%) cases, sustentorial metastasis in 04 (2,7%) cases, leptomeningeal dissemination in 03 (2%) cases and medullary metastasis in 03 (2%) cases. The five years survival rate was 84%.
Conclusion: the surgical treatment of medulloblastoma remains a difficult therapeutic challenge because they have the most virulent form of the disease and are at highest risk for treatment-related sequelae.
Brain tumors are the leading cause of cancer-related death among children in the developing world [1] and medulloblastoma is one of the most frequent high-grade pediatric brain tumors [2]. Survivors of childhood medulloblastoma frequently suffer from significant long-term sequelae, such as physical impairment, reduced neurocognitive functioning, psychological disability, and poor social outcomes [3, 4].
Study design
A retrospective clinical cohort study of 144 patients with meduloblastoma was performed, and they underwent open surgical excision with ventriculo-peritoneal (V-P) shunt. All patients were admitted to the Neurosurgery department in Ait IDDIR Health Hospital Establishment in Algiers between a period of January 2004 and December 2014.
For all the patients, the diagnosis was made after surgery. All patients received the adjuvant treatment.
Preoperative work-up
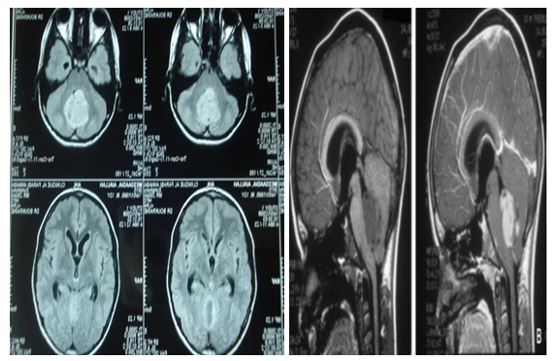
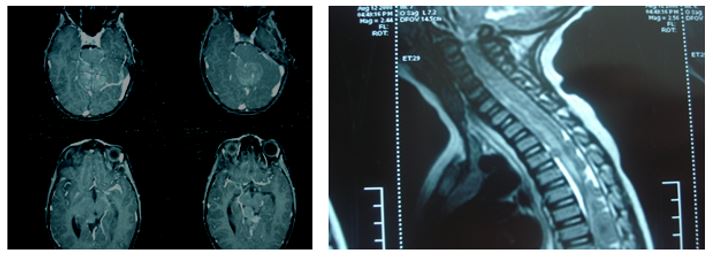
All patients underwent routine physical examination; they also received a thorough neurological evaluation. A special neuro-surgical sheet was applied in all cases included in the study to cover all suspects needed. CT as well as MRI, with and without contrast enhancement, was done for all cases before surgery as shown in Fig. 1.

A ventriculo-peritoneal shunt was performed in all cases (figures 3 and 4).
The treatment is based on the surgery, radiotherapy of all central nervous system and chemotherapy with different modalities.
Operative note
Surgery was performed with general anaesthesia, in prone position, using an operating microscope and microsurgical instruments in all studied cases.
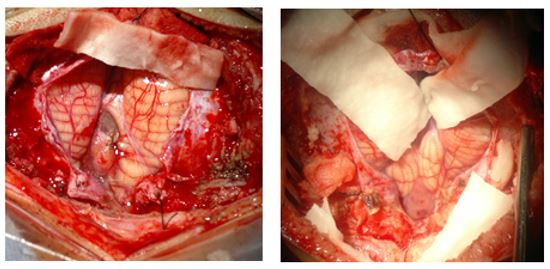
In our study, all patients were operated via a midline suboccipital approach. The objective of this surgery was to complete microsurgical excision of the tumour unless that tumour was invading the brain stem or attaching important vessels or nervous tissue (figures 5 and 6).
Postoperative follow-up
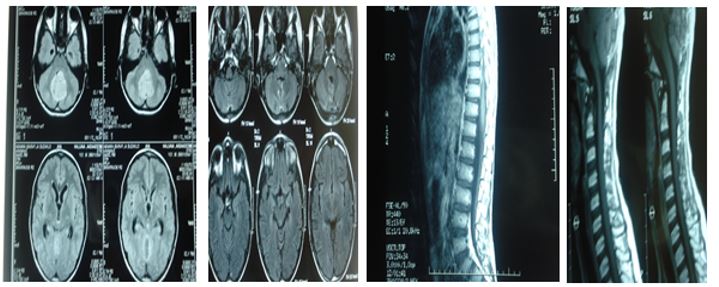
Early CT scan was performed to rule out early complications. Patients were followed clinically in our hospital then in outpatient neurosurgery clinic and also radiological through a period of 10 to 36 months. CT ± MRI with contrast was done at 3rd to 6th month of postoperative period then 1–2 years later. All intraoperative and postoperative complications were collected and reviewed, to detect any recurrence of the excised tumour (figures 7 and 8).


For the Surgical outcome of this study: the Ventriculo-peritoneal shunts were placed in all our patients, the total tumor excision was done to 35% and the partial tumor excision was done to 65% patients.
Between January 2004 and December 2014, 144 patients with medulloblastoma were operated, 63 (44%) patients were females and 81 (56%) were males. We have 59 cases who had age ranged from 05 months to 5 years, however, we had 85 cases who had more than 5 years ; we identified 29 (58%) children and 21 (42%) adults. A male and pediatric predominance were observed in our series.
Clinical manifestations of medulloblastoma vary widely according to the location. The most frequent clinical manifestations found were Intracranial hypertension syndrome (98%) and static and kinetic cerebellar syndrome (18%).Between patients who had intracranial hypertension at diagnosis: we had 1,4% with engagement (2 cases) and 0,7% with coma(01 case).
The imagery had shown that 95% of these tumors originated from vermis. The vermis is the main location of the child Fig. 1.
For the Surgical outcome of this study: the Ventriculo-peritoneal shunts were placed in all our patients, 01 case after surgical removal, the total tumor excision was done to??% and the partial tumor excision was done to??% patients.
In our study, the most common complications were as follows: meningitis( 0,2%),ventriculitis (0,2%), CSF leakage (0,4%), post-surgical hematoma (0,2%), Shunt dysfunction ( 0,6%), aggravation of the cerebellar syndrom (0,4%), affection of mixed nerves ( 0,2%) and cerebellar mutism (0,4%).
According to tumour pathology -based on the classsification of CHANG and coll [10] - we had T2M0 in 41(28, 47%) cases, T2M2 in 2 (1, 38%)cases ,T3aM0 in 98(68%)cases,T3bM3 in 2(1,38%) cases and T3bM4 in 1 (0,7%) case.
MRI medullary was positive in 3 (2%) cases and MRI medullary was negative in 26 (18%) cases (Figures 9 and 10). Medulloblastomas are currently classified into two groups (Packer RJ 2003):
Group of« Standard risk» Medulloblastoma,with Total removal (or residual volume < 1>28(19%) cases (Figure 9).
Group of« High risk» Medulloblastoma, with tumoral remainning (postoperative imaging > 1,5 cm2 ),we had presence of tumor cell in the CSF in 4 (2,7%) cases and medullar metastasis in 8 (5,4%) cases (Figure 10).
Adjuvant treatment regimens following resection included radiation therapy only (72%) for 36 patients including children above and adults and chemotherapy only (39%).
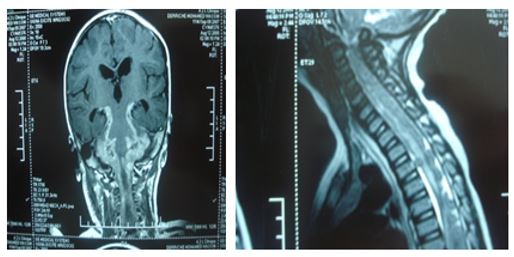
During follow-up period, recurrence occurred in?? % ?? Patients (Figure 11), sustentorial metastasis in 04 (2, 7%) cases, leptomeningeal dissemination in 03 (2%) cases and medullary metastasis in 03 (2%) cases (Figure 12). The five years survival rate was 84%.


Medulloblastoma is the most common childhood primary CNS tumor, and treatment approaches have evolved over the past three decades. Stratification of patients with medulloblastoma into risk groups is the backbone of most ongoing therapeutic studies. Patients are usually characterized as being either average risk or poor risk, although an intermediate risk group may exist. Standard treatment for older children with medulloblastoma consists of radiation and, for most, chemotherapy. Children with non-disseminated disease at the time of diagnosis have been reported to have as high as an 80% five-year disease-free survival rate after treatment with reduced dose (2340 cGy) craniospinal irradiation, local boost radiation therapy (5500 cGy), and chemotherapy, given during and after radiation therapy [5].
In the serie of M.Gajjar [6],106 cases were operated with 34 cases of Leptomeningeal dissemination: 9 cases (8.5%) MRI + and CSF- with 11cases (11.56%) MRI- and CSF+.
In the North American study, the authors has initially concluded to the increase of the early spinal relapses; However, event-free survival in the longer term, seemed identical [7].
Medulloblastoma is a malignant tumor of the cerebellum with high metastatic power, particularly leptomeningeal. The management of this disease must necessarily be multidisciplinary in concerted action teams neurosurgery, neuroradiology, pediatric oncology, neuro-oncology and radiotherapy. Recent work suggests that in the future, data from molecular biology to play a major role in predicting prognosis and therapeutic adaptation strategies [8].
Despite recent advances in chemotherapy, 5-year survival has long been reported at rates around 30 to 50% in this situation.
The alternatives proposed today to try to improve the prognosis of metastatic forms call for the intensification of chemotherapy (high-dose chemotherapy with support of hematopoietic stem cells) rather than increases in radiation doses, source of major sequelae [6].
In young children, it appeared essential to identify more suitable treatments in order to reduce certain unacceptable side effects.“The North American and French studies have shown that prolonged conventional chemotherapy prevented craniospinal irradiation for the vast majority of children with a 5-year survival of 70 to 80%.The German study based on a more aggressive treatment from the outset with administration of intravenous and intraventricular methotrexate, the neurological toxicity of which is not negligible, however gave very encouraging results with an event-free survival at 5 years of 83 % [9].With regard to metastatic medulloblastomas in young children, the prognosis remains bleak, no treatment having yet proven its effectiveness and the long-term sequelae still remaining very serious. However, current studies seem to show that intensive sequential chemotherapy could improve the prognosis. The development of genetic knowledge has contributed to the emergence of new risk criteria, which will surely make it possible to better guide therapeutic strategies [8, 11].
Medulloblastoma is a malignant tumor of the cerebellum with a high metastatic power, in particular leptomeningeal. The management of this pathology must necessarily be multidisciplinary by the concerted action of the neurosurgery, neuroradiology, pediatric oncology, neuro oncology and radiotherapy teams. Recent work suggests that in the future, molecular biology data may play a major role in predicting prognosis and adapting therapeutic strategies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
