
Case Report | DOI: https://doi.org/10.31579/2690-8808/173
1 Neurology division, Department of Medicine, University College Hospital, Ibadan, Nigeria.
2 Rheumatology division, Department of Medicine, University College Hospital, Ibadan, Nigeria.
*Corresponding Author: Chukwuocha Ikechukwu, Grodno State Medical University, 80, Gorkogo St., 230009, Grodno, Republic of Belarus.
Citation: Chukwuocha Ikechukwu, Oladotun V. Olalusi, Joseph Yaria, A. I. Dedeke. (2023), Focal onset Seizures as the First Manifestation of Anti-Ds-DNA Negative Systemic Lupus Erythematosus: A Case Report and Review of Literature, J, Clinical Case Reports and Studies, 4(6); DOI:10.31579/2690-8808/173
Copyright: ©, 2023, Chukwuocha Ikechukwu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 December 2023 | Accepted: 15 December 2023 | Published: 25 December 2023
Keywords: seizures; neuropsychiatric SLE; NPSLE; connective tissue disease; auto-immune disease
Systemic lupus erythematosus (SLE) is a quintessential autoimmune disease once thought to be rare in Africans. It may affect any organ or tissue, synchronously or asynchronously. Neuropsychiatric manifestations of SLE (NPSLE) range from headaches, mood/behavioral disorders to seizures. There are documented reports of seizures accompanying the diagnosis of SLE, with varying prevalence according to specific regions. However, seizures rarely precede the diagnosis of SLE. We present a case report of a 19-year-old female with new-onset focal seizures preceding overt clinico-laboratory diagnosis of anti-dsDNA negative SLE. It may be important to recognize SLE as a potential cause of adult-onset seizures in female subjects to allow early recognition and improved care. Baseline ANA may be a viable screening tool as part of the work up for Adult onset seizure disorders especially in females, in the absence of offending drugs, known metabolic or structural disease.
Systemic lupus erythematosus (SLE) is a quintessential autoimmune disease [1] once thought to be rare in Africans [2]. It may affect every organ and tissue, synchronously or asynchronously. Genetic predisposition, environmental triggers, and hormonal factors, interplay in the pathophysiology of the disease development as well as in disease activity. Clinical manifestations and the pattern of organ involvement are protean, thus reflecting the complex mosaic of pathophysiologic pathways converging into the SLE clinical phenotype [1].
Among the systemic autoimmune disorders, neurological manifestations have been most recognized and well-studied in SLE and less prevalent in other systemic inflammatory and autoimmune disorders [3]. The American College of Rheumatology (ACR) Nomenclature for Neuropsychiatric SLE (NPSLE) provides case definitions for 19 neuropsychiatric syndromes seen in SLE, with reporting standards and recommendations for laboratory and imaging tests [4].
Literature is replete with reports of seizures accompanying the diagnosis of SLE, with prevalence ranging from 9.5% in Iran to 42.4% in Nigeria10, 11,12,15. It is important to note that in most of these reviews and case reports, the diagnosis of NPSLE rarely preceded that of SLE. We present a case report of a 19-year-old female with new-onset focal seizures preceding overt clinico-laboratory diagnosis of anti-dsDNA negative SLE.
A 19-year-old lady seen at the neurology out-patient on account of new-onset seizures, described as focal onset with bilateral tonic-clonic involvement of the limbs. Each episode was associated with facial twitching, upward eye rolling and teeth clenching; lasting 2 minutes with associated postictal sleep. She had a total of four episodes prior to the initial review and had no headaches or premonitory aura. Seizures had started during a febrile illness that was treated with parenteral antimalarials. There were no reports of seizures in the past, head trauma, vascular risks. There was no photosensitivity, joint pain, weight loss or drenching night sweat. She had no history to suggest renal or hepatic decompensation. She neither took alcohol nor use tobacco in any form. She had no previously diagnosed medical comorbidities. She had no known family history of epilepsy. Pregnancy, birth, and attainment of developmental milestones were unremarkable. Clinical examination as well the neurological, cardiovascular, chest and abdominal findings were otherwise unremarkable.
Serum calcium, uric acid, electrolytes, creatinine, and liver enzymes were normal, but serum albumin level was 2.8 g/dl. Urinalysis showed sediments, leucocytes+++, squamous epithelial cells++, bacteria ++ and sterile urine culture study.
An assessment of acute symptomatic seizures was considered and she was commenced on tab carbamazepine 400mg BD.
She presented at the clinic two weeks later (second visit) after having had another two episodes of seizures since the last review despite being regular on prescribed medications. Further neurological exam revealed a conscious and oriented lady with subtle dysdiadochokinesia and past pointing - attributable to the carbamazepine, otherwise essentially normal findings. The erythrocyte sedimentation rate (ESR) as assessed by the Westergreen method was 50mm in the first hour. Her chest radiograph was normal and Brain MRI showed multiple T2/FLAIR sub-centimeter white matter hyperintensities. The Electroencephalogram was otherwise normal.
Approximately three months after the first review (the third clinic visit), she reported exertional fatigue, breathlessness, worsening malaise, anorexia, and abdominal swelling. She was reported to have had episodic irrational behavior and aimless wandering few weeks prior. Clinical examination showed periorbital swelling, generalized maculopapular non-itchy skin rash on the trunk and proximal extremities, a suggestion of a facial rash sparing the nasolabial fold as well as patchy alopecia (figure 1). There was marked epigastric tenderness, abdominal swelling, and ascites.
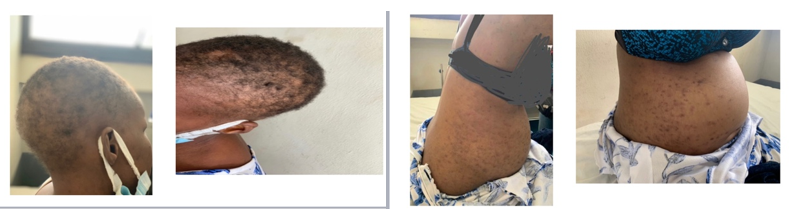
Figure 1: (three months after initial review)
A repeat ESR was 150mm in the first hour, serum anti-nuclear antibodies was 1:640 with low complement (C3, C4) levels. The anti-dsDNA assay returned negative. The ultrasonography of the abdomen and pelvic showed right kidney size at 109x54mm, left kidney size at 127mmx65mm with loss of corticomedullary differentiation, ascites, bilateral pleural effusion suggestive of pan-serositis (figure 3). Repeat urinalysis showed blood 3+, protein 3+. She was admitted and received pulse doses of steroids and was transitioned to oral prednisolone, mycophenolate mofetil (MMF) as well as hydroxychloroquine. She developed angioedema to MMF and this was switched to azathioprine. Due to the persistently low albumin levels and worsening ascites, she was planned for intravenous albumin infusion; paracentesis was attempted but unsuccessful. She is currently receiving multidisciplinary care from the rheumatologist, nephrologist, and neurologist as well as the gastroenterologist
The 2019 EULAR-ACR new classification criteria, used in this case, was developed using rigorous methodology with multidisciplinary and international input and has excellent sensitivity and specificity for the diagnosis of SLE. Use of ANA entry criterion, hierarchically clustered and weighted criteria accurately reflect current thinking about SLE and provide an improved foundation for SLE research and diagnosis [9]. According to this criterion [9], our patient had the entry criteria of ANA: >1:80 (1:640) while meeting criteria across the clinical and immunologic domains. The constitutional symptoms of fever/malaise, neuropsychiatric features, mucocutaneous manifestation (scarring alopecia = 2), serositis (ascites and pleural effusion; score of 5), renal manifestations with 3+ proteinuria, and immunologic domains with low C3 and C4 gives a total score of 10.
The learning point of this case is the initial presentation of SLE with focal onset seizures which had hitherto been unreported in sub-Saharan Africa and may pose a diagnostic challenge in resource limited settings. This may be due to under-recognition or under-diagnosis. The patient presented with neurological symptoms and only began to manifest features of an autoimmune illness three months later, prompting an autoimmune screen using ANA. A retrospective review from a foremost rheumatology clinic in Nigeria noted that a high index of suspicion is needed to diagnose SLE [2] while highlighting that concomitant presentation of neuropsychiatric manifestations and SLE may be rare. Baseline ANA may be part of the work up for Adult-onset seizure disorders especially in female subjects. The negative anti-dsDNA is a major highlight of this case and the early urinalysis findings raised concerns for lupus cystitis.
In a retrospective review by Adelowo et al, out of a total of 1,250 rheumatology cases seen over a period of 6 years, 5.25
The hallmark of this case is the initial presentation of SLE with focal onset seizures which had hitherto been unreported in sub-Saharan Africa and may pose a diagnostic challenge. It may be important to recognize SLE as a potential cause of new adult-onset seizures in female subjects to allow early recognition and improved care. Baseline ANA may be a viable screening tool as part of the work up for Adult-onset seizure disorders especially in females, in the absence of offending drugs, known metabolic or structural disease.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
The authors have no multiplicity of interests to disclose.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
