
Case Report | DOI: https://doi.org/10.31579/2690-4861/226
1 Loma Linda University Health. Family Medicine Department, USA
2 Hospital Nossa Senhora das Gracas. Infectious Diseases Department, Brazil
3 Loma Linda University Health. Family Medicine Department, USA
4 Loma Linda University Health. Family Medicine Department, USA
*Corresponding Author: Ecler Jaqua, Loma Linda University Health. Family Medicine Department, USA
Citation: Graber S, Shierling N, Jaqua E, Nguyen V., (2022) Fever of Unknown Origin: A Hot Diagnosis in the Outpatient Setting. International Journal of Clinical Case Reports and Reviews. 11(3); DOI: 10.31579/2690-4861/226
Copyright: © 2022 Stephen Graber, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 May 2022 | Accepted: 24 May 2022 | Published: 03 June 2022
Keywords: hot diagnosis; cough; myalgias; fatigue
A 63-year-old man presents to the primary care office with a productive cough, myalgias, fatigue, and a temperature ranging from 100.1 to 101 F for a one-week duration. He has atrial fibrillation, hypertension, benign prostatic hypertrophy, and a history of pancreatic cancer status post partial pancreatectomy and splenectomy three months prior, resulting in uncontrolled, post-surgical diabetes. He is taking amiodarone, carvedilol, hydrochlorothiazide, and metformin. He denies any other recent procedures, hospital admissions, or sick contacts.
A 63-year-old man presents to the primary care office with a productive cough, myalgias, fatigue, and a temperature ranging from 100.1 to 101 F for a one-week duration. He has atrial fibrillation, hypertension, benign prostatic hypertrophy, and a history of pancreatic cancer status post partial pancreatectomy and splenectomy three months prior, resulting in uncontrolled, post-surgical diabetes. He is taking amiodarone, carvedilol, hydrochlorothiazide, and metformin. He denies any other recent procedures, hospital admissions, or sick contacts.
Physical examination, including vital signs, is unremarkable. Rapid COVID-19 NAAT testing was negative. However, due to the patient’s fever and productive cough, the patient was diagnosed with clinical pneumonia and prescribed levofloxacin and guaifenesin for seven days.
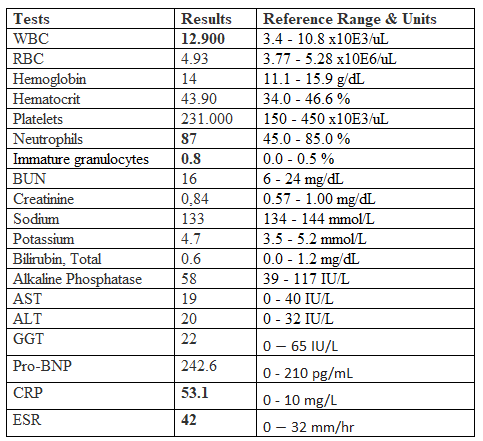
The patient’s symptoms improved initially, but within two days of completing his antibiotic course, the patient presented to the Emergency Department (ED) for low-grade fevers and a dry cough. Physical examination was unremarkable again except for a fever of 101 F. Laboratory evaluations were significant for a mild leukocytosis with left shift and elevated c-reactive protein (CRP). See Table 1. Chest radiograph, urine testing, and COVID-19 PCR testing were negative. The patient was diagnosed with tracheitis and discharged with acetaminophen, guaifenesin with codeine, and prednisone.
Two weeks after ED evaluation, the patient presented to his primary care physician with unresolved low-grade fevers and generalized malaise. Although vital signs were unremarkable, a new III/VI systolic heart murmur was noted at the bilateral upper sternal borders. In addition, the following physical exam findings were not present: rashes, dental caries, ophthalmic changes, extrapulmonary sounds, or lower extremity swelling. The patient then mentions that he has known heart valve problems but that “his heart is fine.” At this point, the patient was urged to present to the hospital for further evaluation of his fevers and new heart murmur. Unfortunately, the patient disagreed with the recommendation due to his fear of prolonged hospitalization, similar to his recent pancreatectomy.
Since the patient refused hospitalization and was clinically stable, an Infectious Diseases physician was consulted in the outpatient setting. Under specialty recommendation, the patient completed the following outpatient evaluation: serial blood cultures, tuberculosis screening, complete blood and metabolic panels, CRP, echocardiogram, and computed tomography (CT) of the chest and abdomen and pelvis.
Findings were significant for mild leukocytosis with left shift and slightly down-trending CRP. Tuberculosis screening was negative despite a CT chest that showed calcifications in the upper lobe of bilateral lungs (Figure 1). CT abdomen and pelvis were negative for any acute changes or complications from previous abdominal surgeries. While waiting for the outpatient echocardiogram, three blood cultures were positive for gram-positive cocci in clusters.

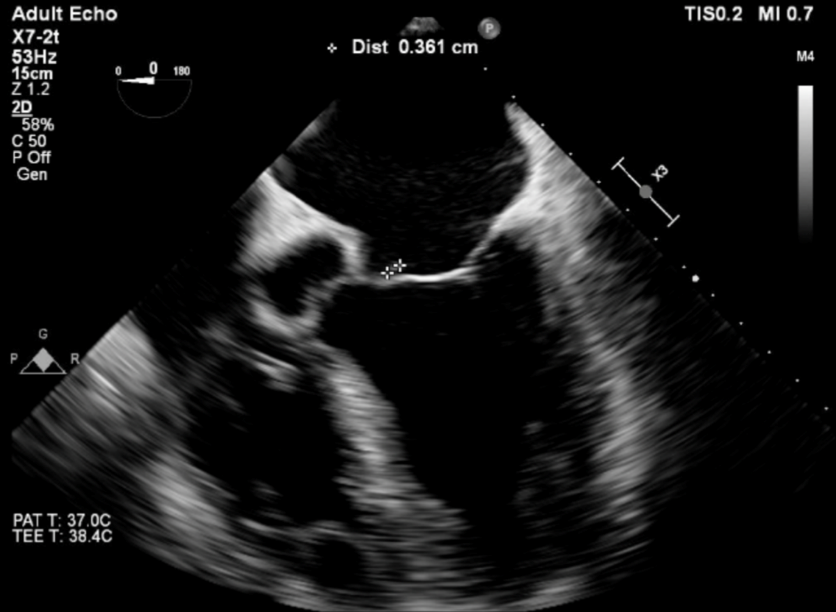
The patient was persuaded to hospitalization with positive cultures and systemic signs of bacteremia. Blood cultures speciated to Streptococcus sanguinis and thus led to a transthoracic and transesophageal echocardiogram that revealed mitral valve prolapse with severe regurgitation and evidence of 4 mm vegetation (Figures 2 and 3). The patient was diagnosed with Streptococcus sanguinis endocarditis and subsequently treated with intravenous Ceftriaxone for four weeks. The patient is doing well and awaiting mitral valve replacement.

The initial diagnosis and treatment for clinical pneumonia were determined based on his clinical presentation – fever and productive cough. However, a more extensive evaluation was warranted after treatment failure and meeting the criteria for fever of unknown origin (FUO). Fever of unknown origin has classically been defined by [1] multiple temperature measurements > 100.9 F, [2] fever duration > three weeks, and [3] uncertain diagnosis after one week of evaluation[1]. However, the definition of FUO has varied over time, and any proposed definition is subjective. Haider and Singh proposed a broader definition in 2022 that includes the core features of fever without an identifiable cause despite reasonable investigations and a duration that is sufficient to rule out self-limiting febrile conditions2. The differential diagnosis for FUO is broad, including infection, rheumatic disease, and malignancy. The most common infections are tuberculosis and abdominopelvic abscess [3]
In this case, the patient was being evaluated in the outpatient setting, and ED and blood cultures may have expedited the patient’s treatment. His blood cultures were eventually ordered by the Infectious Disease specialist. Blood cultures are still indicated in the ED to evaluate suspected sepsis, meningitis, complicated pyelonephritis, and endocarditis4. But, in the outpatient setting, blood cultures have a low yield, with clinical significance in less than 3% of tests [5]. However, in this specific case, since the patient was immunocompromised, met the definition of FUO, and was refusing evaluation in the ED, blood cultures should be considered sooner due to their higher pre-test probability.
Moreover, the patient was not forthcoming about his history of valvular disease, not understanding its importance as he was previously asymptomatic. This patient, with his asplenia, is immunocompromised and at high risk for severe infections [6,7] The clinician should have a high suspicion of atypical infections, and a more thorough dive into the patient’s medical history is necessary. Specifically, this patient’s asplenia and valvular disease place the patient at high risk for endocarditis.
FUO is challenging to evaluate in the outpatient setting but more so in high-risk, immunocompromised patients. This case illustrates the critical need for a high index of suspicion for severe and atypical infections and consideration for hospitalization for expedited evaluation and treatment while always obtaining a thorough medical history.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
