
Case Report | DOI: https://doi.org/10.31579/2641-0419/425
1Department of Anaesthesiology and Critical Care, & PSM.
2SGT medical College, Gurugram, Haryana, and Department of CTVS.
3Tender Palm super specialty Hospital, Lucknow, India.
*Corresponding Author: Vishnu Datt, Professor & HOD Anesthesiology, SGT Hospital, Gurugram, Haryana Former Director Professor and HOD, Cardiac Anesthesia, G B Pant hospital, New Delhi-2.
Citation: Vishnu Datt, Diksha Datt, Shivani Rathee, Vijay Aggarwal, Sunil Gundumala, et al, (2024), Fetal Complete Heart Block. A Successful Surgical Permanent Pacemaker Implantation in a Small for Gestational Age Baby (2.4 Kg): A Case report and Mini Review, J Clinical Cardiology and Cardiovascular Interventions, 7(13); DOI: 10.31579/2641-0419/425
Copyright: © 2024, Vishnu Datt. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 October 2024 | Accepted: 13 November 2024 | Published: 22 November 2024
Keywords: anaesthesia; congenital complete heart block; fetal echocardiography;lv pacing; newborn; ppi; small for gestation age
Congenital complete heart block (CCHB) without structural cardiac anomalies is a rare disease with an incidence of 1 in 15 000 – 20000 live births. CCHB is associated with high intrauterine and post-natal mortality. Maternal autoimmune diseases are often the predisposing factors for the isolated CCHB. Antibodies cross the placenta and cross-react with the developing conduction system, leading to injury and CCHB. Prenatal detection using intrauterine foetal echocardiography at the time of the obstetrics scan, and management with steroids, as well as appropriate delivery planning, and urgent permanent pacemaker implantation (PPI) in the newborn may improve the outcomes in CCHB. However, PPI in neonates can be challenging due to their small size, small vascular and ventricular sizes, and even leadless pacemakers and transvenous implantation in the neonates remain unsuitable. We describe a rare case of CCHB diagnosed at 19th week of pregnancy onwards in 25 yrs old mother, who was a known case of SLE for the last 5 yrs. The CCHB in the small -for -gestational -age (2.4 kg) male, newborn was refractory to the infusion of dobutamine, isoprenaline and dexamethasone. A detailed informed consent was obtained from the parents, and the CCHB was successfully managed with surgical LV epicardial PPI and using a VVI pacing mode at 120 bpm on the first day of life. Only few cases have been reported on the surgical LV epicardial PPI where both leads are attached to the LV and device has been fixed in the left thoracic cavity
The CCHB is a rare conduction disorder that affects about 1 in 20,000 to 25, 000 live births.[1,2] CCHB commonly develops between 18 to 30 weeks of the foetal life. It is associated with significant morbidity and mortality (20-30%)and association of structural cardiac defects further increase the mortality. The established risk factors for mortality in isolated CHB are low birth weight, premature delivery, hydrops fetalis, endocardial fibroelastosis and poor ventricular function. Many cases of CHB are diagnosed during fetal heart echocardiography evaluation, at birth or within the first month of life.[3] However, an early PPI in a newborn may improve the survival. Currently epicardial pacing remains the conventional technique for management of CCHB in neonates, though its challenging due to small size.[4,5,6] The common indications for urgent PPI in newborn are symptomatic bradycardia or sinus node dysfunction, or low cardiac output syndrome(LCOS) either from a CCHB or acquired CHB after open heart surgery.[1,2,3,4] The presented case demonstrates a CCHB diagnosed by fetal echocardiography during obstetrics anomaly scanning at 19th week of the pregnancy. The CCHB was confirmed by subsequent repeated echocardiography evaluation of fetal heart, and ECG of the small for gestational age (2.4 kg) newborn. The baby was delivered under planned elective caesarean section with an Apgar score of 8-9/10 at 1 & 5 minutes respectively, but HR of 52bpm only. The CCHB was refractory to the infusion of dobutamine and isoprenaline. However, the CCHB was successfully managed on the first day of life with an urgent surgical PPI via left 4th intercostal Mini thoracotomy, and LV epicardial leads fixation, and applying a VVI pacing mode at 120 bpm. This case demonstrates that surgical PPI can be performed and device can be fixed in the left thorax safely even in the small for gestational age newborn baby, and the leads can be fixed to the LV to prevent the mitral regurgitation and heart failure due to LV dyssynchrony observed with RA and RV pacing.
A search included PubMed, googles and books of cardiology and cardiac anaesthesia. Various words during search included; the congenital complete heart block, etiology, incidence of CCHB, onset during pregnancy, presentation, initial management, pacemaker support, sites/ access / mode of PPI and positioning of the pacemaker device in a new born and neonates. In addition, smallest size of pacemaker, smallest age and weight of newborn undergoing successful epicardial pacing for CCHB, mortality and complications were also searched using case reports, case series, meta-analysis, RCTs and reviews.
A zero- day old, full- term, male, weighing 2.4 kg, first baby of a 25-year-old mother was shifted to the cardio-thoracic and vascular surgery department immediately after the planned caesarean delivery for evaluation and management of CCHB. There was no history of maternal infection, diabetes mellites, alcohol consumption during pregnancy, however, her medical history was only remarkable for autoimmune disease (SLE), diagnosed approximately 5 years back, but asymptomatic. Obstetric ultrasound scanning during pregnancy at 19 weeks revealed an inappropriately low fetal HR, and so, she was referred for fetal echocardiography for further evaluation, that confirmed the CCHB (HR of 46bpm). Therefore, it was decided to assess the fetus progress with serial echocardiography and planned elective caesarean section at term, and followed by PPI, if baby remains stable after the delivery. On examination, the cry was good, respiratory rate was 32 / min with an oxygen saturation of 99% with 2 L of oxygen support, HR was 52 bpm, and urine output was adequate. Twelve lead ECG confirmed the A-V dissociation, narrow QRS complexes, and a complete heart block with a rhythm of 52 bpm, and CCHB was refractory to the infusion of isoprenaline and dobutamine. [Figure-1]
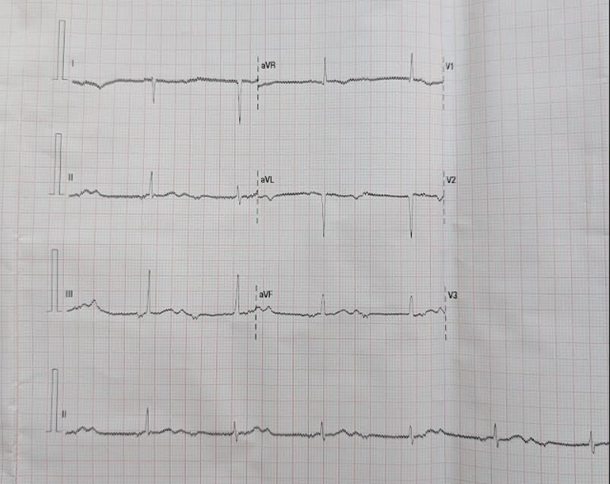
Figure 1: Twelve lead ECG of the newborn shows(arrow) complete A-V dissociation with narrow QRS complexes, a rhythm of 52 bpm suggestive of a complete heart block. The CCHB was refractory to the infusion of isoprenaline and dobutamine.
Transthoracic echocardiography revealed situs solitus, levocardia, atrio- ventricular and ventriculo- arterial concordance, ventricular D-loop, left sided aortic arch with a 3mm anterior shelf with a lumen of 5mm, but no coarctation, an ostium secundum ASD of 0.6 cm with left to right shunt, 2mm PDA with left to right shunt, mild TR and complete heart block (HR during study was 55bpm). Chest -X-ray did not revealed any cardiac or pulmonary abnormality. [Figure-2a] Intravenous access was achieved with 26 G cannula and 10
Transthoracic echocardiography revealed situs solitus, levocardia, atrio- ventricular and ventriculo- arterial concordance, ventricular D-loop, left sided aortic arch with a 3mm anterior shelf with a lumen of 5mm, but no coarctation, an ostium secundum ASD of 0.6 cm with left to right shunt, 2mm PDA with left to right shunt, mild TR and complete heart block (HR during study was 55bpm). Chest -X-ray did not revealed any cardiac or pulmonary abnormality. [Figure-2a] Intravenous access was achieved with 26 G cannula and 10 percentage). dextrose maintenance infusion was started. Although, the baby was hemodynamically stable, but CHB was not improving with the medical therapy. Therefore, it was decided for urgent PPI to avoid the complications like dilated cardiomyopathy, endocardial fibroelastosis, mitral regurgitation, LCOS and mortality. A detailed informed consent was obtained from the parents. In the operating room (OR), ECG and SPO2 monitoring was started. General anaesthesia was induced with intravenous fentanyl (5mcg) and ketamine (5mg), and atracurium(2mg) was used as a muscle relaxant to facilitate the endotracheal intubation with 2.5 mm. ID, cuff tube, fixed at 9cm. Intermittent positive pressure ventilation (IPPV) was initiated with 50 percentage oxygen in air along with sevoflurane (1-2 percentage). A tidal volume of 25 ml and rate of 32/min was used to maintain an ETCO2 of 30-35 mmHg. Left femoral artery cannulation was performed with 22 G leader Cath for continuous blood pressure monitoring and serial arterial blood gas(ABG) analysis. 3 FG double lumen catheter was inserted via the right internal jugular vein for CVP monitoring and administration of various medications and inodilators. In addition, temperature, urine output and airway pressure were also monitored. Anaesthesia was maintained with intermittent fentanyl, midazolam, atracurium and sevoflurane. Left lateral thoracotomy at 4th intercostal space was used for PPI. Pacing leads (Model. Medtronic 4968-35cm, Sereal No. LEN471040v) were fixed at the LV anterior wall, at 1cm distance, and the pacemaker device (Medtronic, model no. AttestaTM SR MRI Sure ScaneTM ATSR01) was secured in a Gor-Tex pouch, and fixed in the extra-pleural, subcostal region in left thorax.[Figure 2b][Video 1] The generator mode VVI was set at a rate of 120 bpm.[Figure-3] The pacemaker was placed in the Gor-Tex pouch to avoid the fibrosis, dense scarring, adhesions and inflammation around the pacemaker. The hemodynamic were maintained with dobutamine infusion(5mcg/kg/min). Following chest closure, atracurium neuro-muscular block was reversed with neostigmine (0.05 mg /kg) and glycopyrrolate (0.015mg/kg) mixture. The baby was extubated on the OT table. He was fully awake and maintained arterial oxygen saturation of 95-99 percentage with 2 L, oxygen flow via nasal canula, and BP of 55-75/ 40-55 mmHg. Total duration of the surgical procedure was 75 min. Patient maintained hemodynamic in ICU and dobutamine was tapered in the next 24 hours. the rest of the course was unremarkable, and patient was transferred back to the referral hospital on 3rd day of PPI.

Figure 2a: Chest -X-ray (A-P view) shows clear lungs, a normal cardiac silhouette without any chamber enlargement and a clearly outlined chest cavity
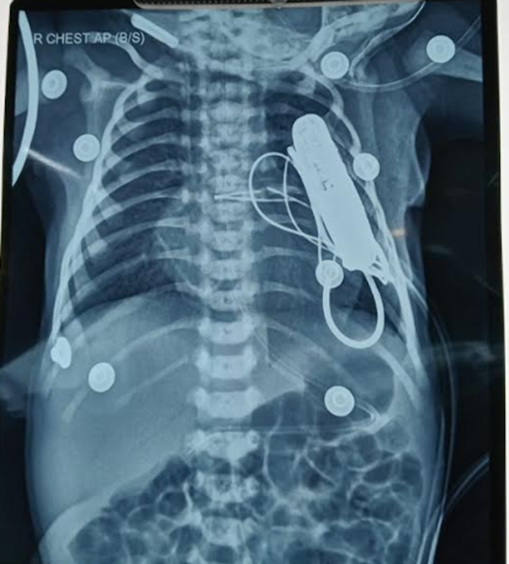
Figure 2a: Chest -X-ray (A-P view) shows clear lungs, a normal cardiac silhouette without any chamber enlargement and a clearly outlined chest cavity
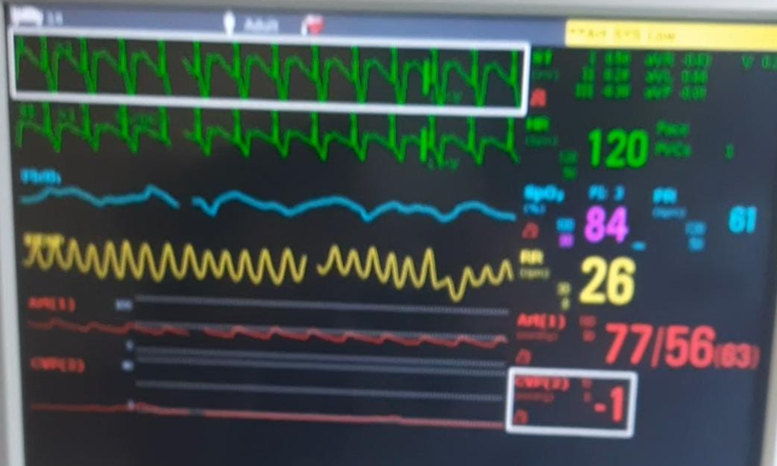
Figure 3: The picture of the multichannel monitor after successful permanent pacemaker implantation shows the paced HR of 120bpn and a BP of 77/56 mmHg and a CVP of -1 mean. The findings suggestive of hemodynamically stable baby following successful PPI in a one day- small- for gestational -age, newborn.
Central Message: Congenital complete Heart block in the fetus can be diagnosed during obstetrics anomaly scanning at 19th week of gestation by fetal heart echocardiography. Its progress in the newborn can be evaluated by ECG and echocardiography. It is also essential to rule out other associated complex congenital cardiac anomalies. The refractory CCHB even in a small -for -gestational -age newborn can be managed successfully with a surgical PPI on the first day of life after planned caesarean delivery. The pacing device can be safely fixed in the extra pleural subcostal region of the left hemithorax, and both pacing leads can be fixed to the LV to avoid ventricular dyssynchrony and MR and cardiac failure.
CCHB is considered if it is diagnosed in utero, at birth or with in first month of the life. The incidence of the CCHB is about 1 in 20,000 to 25,000 live births.[1,2] Fetal heart block usually develops between 16 and 24 weeks of gestation, although later onset can occur. CCHB may be associated with either autoimmune diseases(SLE, Sjogren’s syndrome) in the mother or structural congenital heart defects(CHD) like left atrial isomerism, L-transposition of the great arteries, or atrioventricular septal defect in the fetus.[7] CCHB induced by the CHD has been reported to be non-reactive or under responsive to treatment with terbutaline, and has a poor prognosis, with 7 percentage fetal demise, and additional 10 –15 percentage mortality during infancy alone.8,9 Maternal autoimmune diseases mediated heart block often presents with isolated CCHB as a result from the transplacental transfer of the ssA (Ro) or ssB (La) antibodies, which cause inflammation, fibrosis, scarring and injury of the fetal cardiac conduction system.[10] Approximately, 20–30 percentage of infants with CCHB have mothers with a previous diagnosis of autoimmune disease, and a majority are asymptomatic.[11] The presented baby’s mother was also asymptomatic case of SLE for the last 5 years. It has been reported that approximately 20–30 percentage of these infants suffer fetal or neonatal deaths. Almost 10 percentage of neonates with antibody-positive CCHB tend to born with hydrops or congestive heart failure (CHF) secondary to intra-uterine myocarditis and/or severe bradycardia.[12] Furthermore, it has been reported that extremely low fetal ventricular rates increase the likelihood of poorer outcomes.[2] Though, the CCHB in this newborn was refractory to the infusions of isoprenaline and dobutamine, even then he remained clinically stable. Some authors have reported that once 3rd degree heart block is identified, reversal has never been achieved, despite dexamethasone therapy.[13] CCHB is generally confirmed by fetus echocardiography evaluation during 18 –22 weeks of gestation using 2-D echocardiography and M-mode interrogation of the atrial and ventricular wall motions. Pulsed wave Doppler evaluates simultaneous flow across the mitral and aortic valves or the superior vena cava and aorta to demonstrate the lack of association between the atrial and ventricular flows.3
The pharmacological therapy for CCHB is aimed at limiting further immune mediated damage using corticosteroids, and to augment cardiac output via beta stimulation of heart rate.14 Therefore, early antenatal diagnosis by fetal echocardiography and regular assessment on the progress of CCHB and fetus till term pregnancy, along with proper planning for caesarean delivery, and assessment of new born clinical status, and cardiac rhythm and CCHB on ECG, and any structural cardiac anomalies on echocardiography, as well as urgent PPI are critical in order to prevent CHF and sudden death. This case, demonstrates the possibility that the fetus can survive for some period despite very low ventricular rates, and this may provide few hours for PPI to maximize neonatal survival. Eventually, the presented baby remained hemodynamically stable with dobutamine infusion, though the CCHB continued to be refractory. Therefore, it was decided for the PPI to avoid the imminent hemodynamic deterioration. It was successfully performed with in 24 hrs of the birth, and the HR raised from 52 bpm to 120 bpm. Therefore, this case narrates that PPI is the main therapy for the newborn with CCHB. Central indications for PPI in neonates include CCHB with wide QRS escape, ventricular dysfunction, ventricular ectopy or significant bradycardia, CCHB with heart rate below 50bpm or persistent postoperative CHB persisting for more than 7 days.[15,16] However, the implantation of pacemakers (PM) in neonates and infants requires consideration of small body size, marked body growth potential, and the long duration of future pacing therapy to be expected.
Although dual-chamber pacing is the most common mode of pacing in the adult population, contributing to physiological HR and atrioventricular synchrony, but single-chamber ventricular pacing is a widely used and accepted pacing mode in children.[17] However, due to one day of age, low weight, grossly small cardiac structure and vascular access, it is difficult to implant endocardial pacing leads, and hence, the implantation of epicardial pacing leads becomes an ideal method to treat CCHB. Epicardial pacing is also a preferred technique because transvenous leads increase risk of vascular occlusion, thrombosis, and atrioventricular valve regurgitation in this age group.[5] We chose the LV because previous reports have suggested that epicardial LV pacing shows better outcome than RV pacing as ventricular synchrony and LV function.[18,19] Others also approve clinically proven Managed Ventricular Pacing (MVP) algorithm promoting intrinsic conduction and reducing unnecessary RV pacing by 99 percentage leading to reduced risk of AF and HF hospitalization.[20] Matsuhisa H, et al and others have also implanted most ventricular leads (30/31, 96.8 percentage) in the anterior wall of the LV to avoid the RV pacing-induced dyssynchronous LV contraction, and development of significant MR and heart failure.[21,22,23] A left lateral thoracotomy can directly reach the surgical site (LV), obtain excellent exposure, shorten operation time, and get small trauma and causes less fibrosis, scarring, adhesions, and inflammation.[24]
Berul et al have used a tiny pacemakers for tiny babies as a novel implantable pulse generator (Medtronic Micra TM 29.4x 16.6x 9.6, 5gm, battery life 16-17 yrs) to treat 5 premature neonates weighing range of 0.99- 2.68 kg with CHB at birth in 4 centres, with 100 percentage success rate.[25] Recently, the Micra™ transcatheter leadless pacing (TLP) system (Medtronic, Minneapolis, MN, USA), the world’s smallest commercially available pacemaker, weighing 1.75 g with a volume of 0.8 mL with accepted electrode space of 18mm providing various pacing modes like VVI, VVIR, VOO, OVO, VDD, VDI, ODO, OFF have been designed for transvenous implantation in adults. Recently, Medtronic has modified the Micra™ pacemaker generator to provide a header block for epicardial pacing using a standard bipolar epicardial lead to make it suitable and effectively manage CCHB even for the smallest neonate of 2.68kg. However, due to anatomic considerations, such as small vessels and ventricle sizes, leadless pacemakers and transvenous implantation in the youngest neonatal population remain unsuitable. And therefore, this pacemaker has been approved under “Emergency Use” yet seeking approval for regular use in small babies with CCHB by the U.S. Food and Drug Administration (FDA).[26]
Based upon the recent literature, the focus is drawn to the fact that epicardial pacing leads fixed to the LV should probably be considered for pediatric patients in whom atrio-ventricular or inter-ventricular pacing might not be possible to achieve, or else as a regular approach for small patients requiring VVI epicardial pacing to prevent the LV dyssinchrony.[21,22,27] First and foremost, Bhattacharya et al have also published a largest series on the newborn with CCHB managed with epicardial PPI with Steroid eluting bipolar suture leads (Medtronic Capsure 10366 or 4968, Minneapolis, MN) and ventricular lead was placed on the anterior RV free wall, using a partial sternotomy, and the pacing device was placed in the rectus sheath. They have reported an overall mortality rate following PPI as 13.6percentagee, and predominantly related to myocardial dysfunction.[16]
The beneficial effect of left ventricular pacing on short- and midterm electromechanical function and synchrony has recently been verified in a cohort of neonates and infants and the left ventricular apex seems to be the best location.[28] In the long term, the beneficial impact of epicardial pacing on ventricular synchrony resulting from LV rather than RV pacing may outweigh the advantages of transvenous pacing.[17] Dyssynchronous LV contraction results in papillary muscles dysfunction, delays end-diastolic mitral valve (MV) closure, and early systolic MR, particularly in the pre-existence of unusual MV.[29] Implantation of a dual chamber epicardial pacemaker in neonates with CCHB is technically feasible and results in excellent outcomes in patients with structurally normal hearts, and even system longevity at 6 years is excellent. Although, Patients with CCHB and heterotaxy syndrome have a poor prognosis despite dual-chamber pacing. [30]
Aellig NC, et al have implanted Bipolar steroid-eluting epicardial leads (Medtronic CapSure Epi 10366 and 4968) through median sternotomy, the sybxyphoid approach, or thoracotomy. The authors have reported that Sternotomy is the preferred approach in case the pacemaker implantation is required at the time of cardiac surgery, or for postoperative heart block, or for very small babies in whom exposure through a subxyphoid access has been suboptimal. The atrial leads were fixed at RA and LA and ventricular leads at RV and LV in the newborn and neonates for the dual chamber pacing. Even for neonates and infants, modern pacemaker therapy is feasible, safe, and effective.[4] But these authors have used Pacing system implantation immediately after birth under external pacing for Two infants with severe hydrops fetalis for whom transvenous pacing was not suitable owing to the small patient size of 1 kg and difficult venous access.in addition, the Small patient size necessitated positioning of the pulse generator within the abdominal cavity.[4]whereas, in the presented patient the leads were attached to the LV and a single chamber(LV) VVI pacing was used, and the device was fixed in the left thorax rather behind the rectus sheath. Kelle AM et al have also reported that Implantation of a dual chamber epicardial pacemaker in neonates technically feasible and results in excellent outcomes in patients with CCHB with normal heart and the device longevity at 6 years is excellent. However, like Aellig et al a poor prognosis despite a dual chamber pacing in neonates with CCHB and heterotaxy syndrome has been reported. [30] In their 2.2-kg, newborn baby, the dual-chamber pacing leads were placed through a full sternotomy. The steroid-eluting leads were directly affixed to the high on the RVOT epicardium and the RA and the pacemaker was in a pocket created beneath both rectus muscles. They have suggested that dual-chamber pacing maintains a sinus node responsiveness and physiologic A-V synchrony. This baby with Heterotaxy (polysplenia), unbalanced AVC, coarctation of the aorta suffered a mortality. Aellig MC et al, Kelle AM et al and Vos LM et al have suggested that epicardial pacing is the method of choice because transvenous leads are accompanied by an increased risk of vascular occlusion, thrombosis, and atrioventricular valve regurgitation in this age group.[4,5,31] Epicardial pacemaker implantation in neonates and infants is an invasive but safe and effective procedure with a relatively low risk of complications. The use of intracardiac electrodes is contraindicated in patients with congenital heart disease and intracardiac shunt because of the risk of thromboembolic complications.[5]
The central picture of the procedure depicts the shielding of the permanent pacemaker device in the handmade Gor-Tex pouch and fixed in the extra pleural subcostal region of the left hemithorax. In addition, both the pacemaker leads are attached to the LV anterior wall at 1Cm distance [Figure4a&b]. This single case report also demonstrates that PPI is feasible and safe even in the small for gestational age, newborn baby to counter the refractory CCHB. The device can be successfully positioned in the thorax without any complications, and the leads should be attached to the LV to avoid the ventricular dyssynchrony and MR and heart failure.[21] Based upon recent literature, attention has been drawn to the fact that left-inserted epicardial pacing wires should probably be considered for pediatric patients in whom A-V or inter-ventricular pacing might not be possible to achieve, or else as a consistent approach for small patients requiring VVI epicardial pacing to prevent the LV dyssynchrony.[27] Above all, the successful surgical PPI in a small for gestational age, newborn with refractory CCHB requires a multidisciplinary approach

Figure 4a &b. (Central picture). The perioperative picture depicts that the permanent pacemaker device was shielded in the handmade Gor-Tex pouch and fixed in the extra pleural subcostal region of the left hemithorax (arrow). In addition, both the pacemaker leads are attached to the LV at 1Cm distance(arrow). This case demonstrates that permanent pacemaker insertion is feasible even in the small for gestational age, newborn baby to counter the refractory CCHB. The pacemaker device should be secured in the Gor-Tex pouch to avoid the adhesions and fibrosis around the device and to facilitate the easy replacement in the future. The device can be successfully positioned in the thorax without any complications, and the leads should be attached to the LV to avoid the ventricular dyssynchrony and mitral regurgitation and heart failure.
The maternal autoimmune diseases may be associated with the CCHB in the fetus. This single case demonstrates that CCHB in fetus can be diagnosed by fetal heart echocardiography performed between 18- 22 weeks of gestation. Early diagnosis and prompt management of the case is important for a better prognosis and prevention of associated complications. Following proper planned caesarean delivery, the newborn should be subjected to the echocardiography for assessment of CCHB and associated cardiac anomalies, and ECG for assessment the HR and
rhythm. The LV epicardial PPI can be performed safely within 24 hrs of the birth, even in the small for gestational age (2.4 Kg) newborn. The pacemaker can be fixed in left thoracic cavity, and leads are attached to LV anterior wall at 1cm distance for LV pacing (HR of 120 bpm) using VVI mode to avoid the LV dyssynchrony. Newborn with a CCHB should be managed by experienced multidisciplinary team at a tertiary care centre, and the only definite treatment is insertion of a permanent pacemaker
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
