
Opinion | DOI: https://doi.org/10.31579/2578-8965/176
Department of Pediatrics Louisiana State University Health Sciences Center at Shreveport 1501 Kings Hwy, Shreveport, LA, 71103
*Corresponding Author: Shabih Manzar, Department of Pediatrics Louisiana State University Health Sciences Center at Shreveport 1501 Kings Hwy, Shreveport, LA, 71103
Citation: Shabih Manzar, (2023), Fetal Atrial Flutter: Early Detection and Treatment, J. Obstetrics Gynecology and Reproductive Sciences, 7(5) DOI:10.31579/2578-8965/176
Copyright: © 2023, Shabih Manzar. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 June 2023 | Accepted: 07 July 2023 | Published: 17 July 2023
Keywords: .
Fetal atrial flutter (AF) can occur with structurally normal hearts or congenital heart disease, including atrioventricular septal defect, hypoplastic left heart syndrome, pulmonary atresia, and Ebstein's malformation. 1 It is important to detect fetal AF early and treat it appropriately. We present a case of fetal AF that was treated timely, resulting in no associated complications. The infant was born by cesarean section at a gestational age of 37 weeks with an Apgar score of 9 and 9. The birth weight was 2860 grams. The antenatal history was positive for fetal tachycardia. A fetal echocardiogram (Figure 1, panels A and B) showed atrial flutter with 2:1 conduction (atrial rate of 414 beats per minute with a ventricular rate of 202 beats per minute).

Figure 1: The fetal echocardiogram in M-mode shows discordant atrial (Panel A) and ventricular heart rates (Panel B).
The mother was admitted to the ICU and placed on sotalol. We noted the termination of fetal tachyarrhythmia after treatment. No maternal risk factors were identified. The infant, after birth, remained stable with a heart rate of 130-145 beats per minute and had a normal sinus rhythm on an electrocardiogram (ECG). An echocardiogram showed moderate to large patent ductus arteriosus with bidirectional shunting, torturous aortic arch with normal left and right ventricular function. A cardiac computed tomography angiography confirmed a right-sided aortic arch with Kommerell diverticulum and aberrant left subclavian artery (Figure 2, panels A and B).
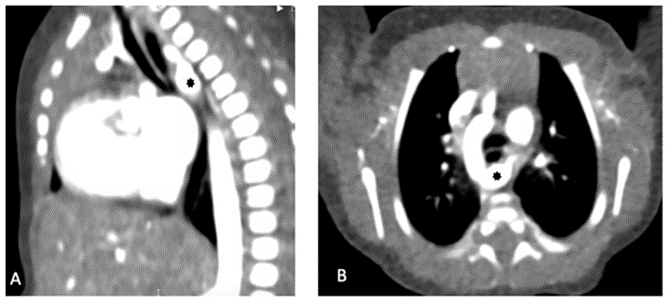
Figure 2: Panel A: Cardiac computed tomography angiography (Sagittal view), showing aberrant left subclavian artery with prominent common Kommerell diverticulum (black asterisk) compressing the esophagus posteriorly.
Panel B: Cardiac computed tomography angiography (Axial view), showing right-sided aortic arch with aberrant left subclavian artery with prominent common Kommerell diverticulum (black asterisk) compressing the esophagus posteriorly.
The infant was observed for 72 hours with no reoccurrence of any arrhythmias. The infant remained asymptomatic, had a normal modified barium swallow, and was discharged home with close follow-up.
Based on Edwards's classification, the case presented has a Type II right-sided aortic arch.2 Kommerell diverticulum (KD) with right-sided aortic arch (Type II) is usually seen in 0.05–0.1% of the population. 3 Fetal atrial
flutter (AF) association noted with the Type II right-sided aortic arch is most likely coincidental. The exact mechanism of how the right-sided aortic arch cause fetal arrhythmia is unknown, but an abnormality in the conductive pathway or electrophysiology is plausible. 4 The association between AF and KD noted in the case needs further investigation
Dr. Manzar conceptualized and wrote the draft.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
