
Research Article | DOI: https://doi.org/10.31579/2768-0487/165
1 Demonstrator of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Lecturer of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
3 Professor of Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
*Corresponding Author: Hanan Elzeblawy Hassan., Demonstrator of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Sahar G Zaki., Fatma S Nady., Hanan E Hassan., (2025). Female Workers’ Total Practices Regarding Breast Self-Examination at Beni-Suef University., Journal of Clinical and Laboratory Research 8(2); DOI:10.31579/2768-0487/165
Copyright: © 2025, Hanan Elzeblawy Hassan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 January 2025 | Accepted: 10 February 2025 | Published: 17 February 2025
Keywords: practices; breast self-examination; female workers
Background: Women who self-examine their breasts get familiar with their appearance and feel, and they can identify any changes in their breasts as soon as feasible.
Aim: assess female workers’ total practices regarding breast self-examination at Beni-Suef University. Subjects and Methods: A descriptive sample of 323 working women at Beni-Suef University was selected.
Tools: (I): A Structured Interviewing Questionnaire Sheet. (II): Breast Self-Examination Checklist.
Results: It revealed that 53.8% of the studied sample were married at ages 17-22 years, 82.8 had practiced breastfeeding, 65.4% stopped menstruation at age >45 years, 71.8% had used contraception, 73.1% didn’t have family history of breast cancer, 93.5% didn’t performed mammogram. Related to BSE, 50.5% knew that breast self-examination was the first method in the early diagnosis of breast cancer, 74.9% did not practice breast self-examination, 48.3% not knowing how it was practiced. Also, 90.1% of the female workers having inadequate total practices level regarding breast self-examination, 44.9% get information from social media.
Conclusion: Based on the findings of the present study, it can be concluded that there were statistically significant relation between the studied female workers total practices level regarding breast self-examination score with their educational level and place of residence, family history of breast cancer. A highly statistically significant relation with their total practice level of breast self-examination and source of information was observed. Recommendations: Implement an educational program to enhance women’s practices regarding breast self-examination.
Physical breast examination, breast self-examination, and a clinical breast examination are all included in the physical breast examination. Breast self-examination involves utilizing a mirror and one's hands to check for changes in one's breasts and underarms. In contrast, a doctor performing a clinical breast examination looks for lumps and other abnormalities that could indicate breast cancer. Clinicians perform physical examinations, which involve examining the breasts, the region surrounding the neck and collarbone, and the armpits (axillae). Breast abnormalities, such as lumps or other signs of breast cancer, are observed. Lymph nodes are also examined as they are typically enlarged in breast cancer patients [1-4].
Women who self-examine their breasts get familiar with their appearance and feel, and they can identify any changes in their breasts as soon as feasible. Since many breast cancers are discovered by women themselves, breast self-examination is best done after menstruation (days 5 to 7, if one counts the first day of menses as day 1). Teaching all women how and when to inspect their breasts is a top goal. Women who self-examine their breasts significantly contribute to the early detection of breast cancer and the decrease in cancer-related deaths [5-8].
It has been discovered that nurses use three different methods to look for lumps during a breast self-examination: Tissue sections can be examined in three different ways: 1) the concentric circle method, which looks in increasing or decreasing concentric spheres; 2) the radial spoke, which looks at the edges and moves in a circular pattern toward the nipple; and 3) the vertical strip approach, which examines the breast in perpendicular pieces that intersect and move throughout the chest [9-11].
Aim Of the Study
The current study was conducted to assess female workers’ total practices regarding breast self-examination at Beni-Suef University.
Subject And Method
A descriptive sample was used and selected from working women at Beni-Suef University were selected according to the following inclusion criteria: Females aged 18-60, Free from any type of cancer, did not receive any chemotherapy or radiotherapy, and free from any diagnosed psychological disorders
Sample Size:
The sample was calculated by the following equation using the Chandrasekharan equation to calculate the sample size from the next formula (Chandrasekharan et al., 2019): n = N/{1 + N(e)2} Where n = sample size, N = population size is 1700, and e = 0.05. The total number of working women at Beni-Suef University at the time of conducting the study was 1700 women, so the target population of this study was 323 women. The sample size calculation was done using the following equation: n = 1700 / {1 + 1700(0.0025)} = 323. The study sample consists of 323 women who were working at Beni-Suef University and accepted to participate in the study at the time of the data collection.
Tools of data collection:
Tool I: A Structured Interviewing Questionnaire Sheet
It contains women's personal and socio-demographic data.
Tool II: Breast Cancer Preventive Measures Checklist:
Breast Self-Examination Observational Checklist was comprised of practical steps to evaluate and track women's breast self-examination performance.
Scoring system: Each step was scored a zero grade (if the step was not done) and a one grade (if the step was done) with a total score of 35 degrees. The total practical scores were calculated into two groups:
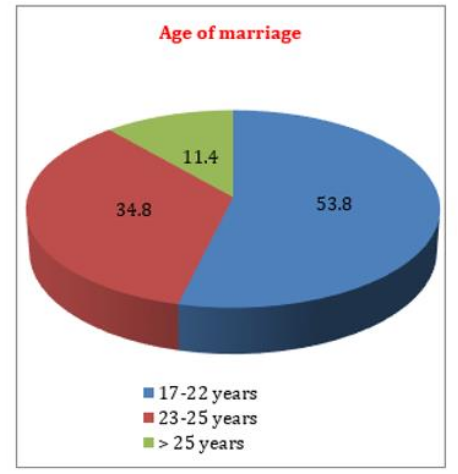
Figure 1: Age of marriage foe the studied female workers.
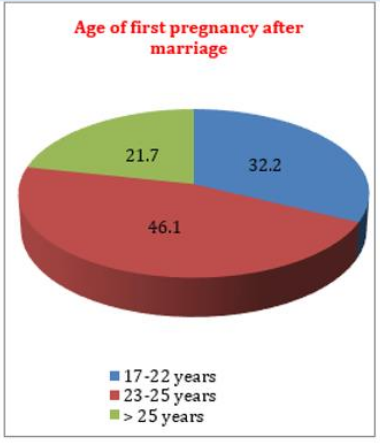
Figure 2: Age of the first pregnancy after marriage for the
studied female workers
Figure 1 & 2: reveals that more than half (53.8%) of them were married at ages 17-22 years, and less than half (46.1%) of them had their first pregnancy at ages 23-25 years.
Figure (3) showed that the majority (82.8%) of them had practiced breastfeeding, while non-breastfeeding women due to rejection of the child were less than three quarters (73.9%).
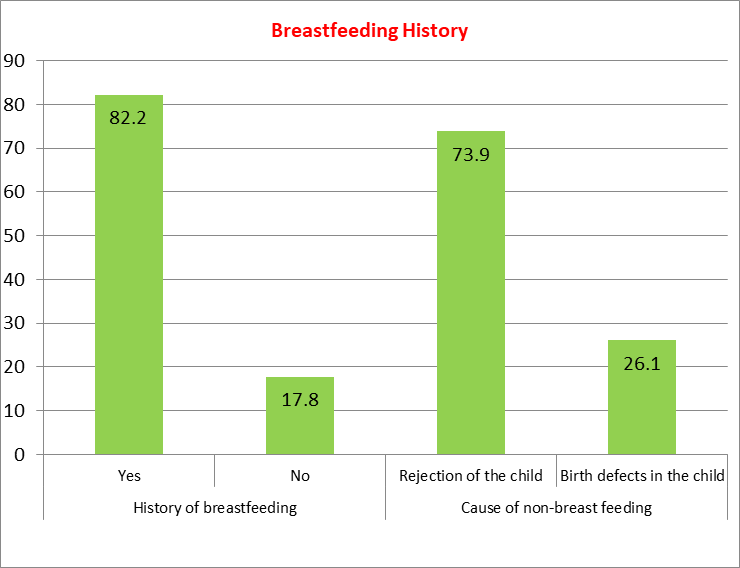
Figure 3: Breastfeeding History of the studied female workers.
Figure (4) revealed that most of the studied women (83.9%) had not had their menstrual cycle stopped, and less than two-thirds (65.4%) had it stopped at age >45 years.
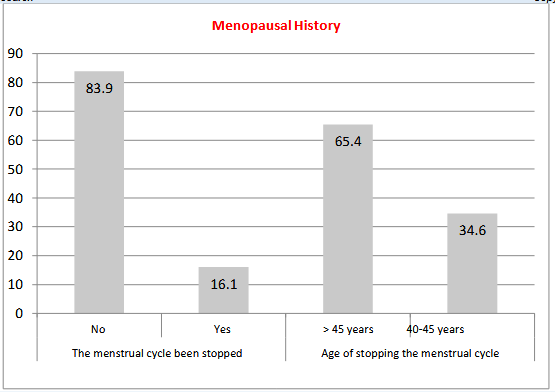
Figure 4: Menopausal History of the studied female workers.
Figure (5) revealed that less than three-quarters (71.8%) of them had used contraception from them; less than two-thirds (63.8%) had used vaginal IUDs, and less than two-thirds (61.6%) of them used contraception for more than 2 years. Regarding the complication of contraception, almost three-quarters (75.0%) of them had no complications, while women who had complications due to bleeding were more than half (58.6%).
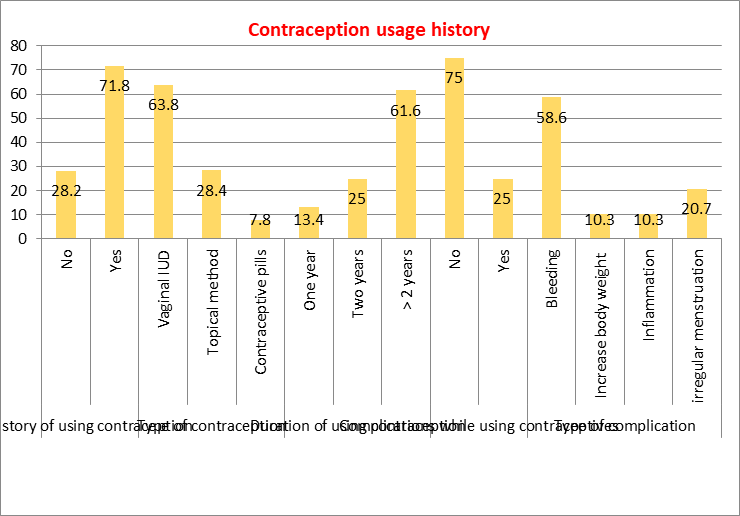
Figure 5: Contraception usage History of the studied female workers.
Figure (6) presents that, less than three quarter (73.1%) of the studied female workers didn’t have family history of breast cancer while female who had family history of breast cancer with first degree relatives (mother) were less than half (40.0%). Additionally, majority (93.5%) of them didn’t performed mammogram. Meanwhile, less than three quarter (70.0%) of them didn’t have breast problems while less than one third (33.0%) of them had problem due to discharge. Despite that, more than half (59.8%) of female who had breast problem hadn’t done any special investigation for this problem and less than two thirds (64.1%) of female who perform investigations had done medical breast examination.
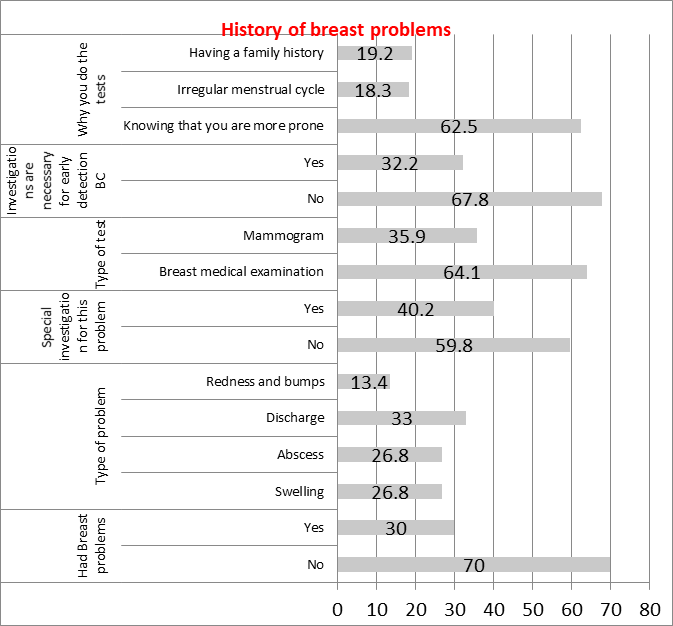
Figure 6: History of breast problems of the studied female workers.
Table (7) Related to BSE, more than half (50.5%) of them knew that breast self-examination was the first method in the early diagnosis of breast cancer. In addition, nearly three-quarters (74.9%) of them did not practice breast self-examination, with less than half (48.3%) not knowing how it was practiced.
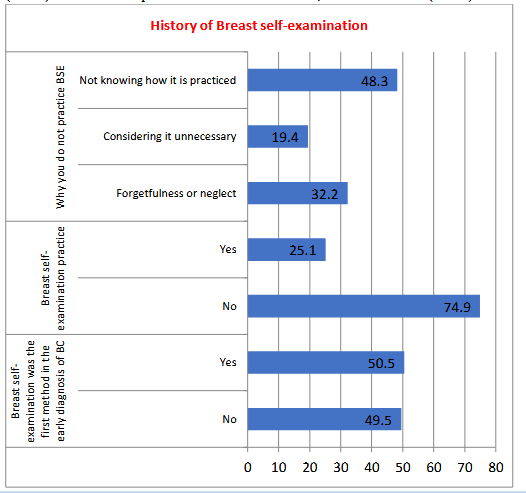
Figure 7: History of Breast self-examination of the studied female workers.
Figure (8) presents that 73.1% of the studied female workers didn’t have a family history of breast cancer, while females who had a family history of breast cancer with first-degree relatives (mothers) were 40.0%.
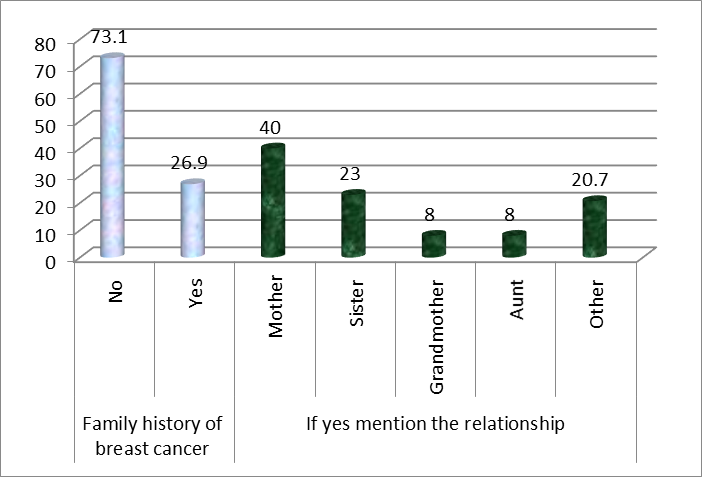
Figure 8: Percentage distribution of the studied female workers regarding their family history of breast cancer (n=323).
Figure (9) shows most of the studied sample have inadequate level regarding their Sub-items of breast self-examination practices (examination preparation 76.2%, examination by consideration 88.2%, asymmetry in the nipple, areola, or breast90.4%, and tactile examination 91.6%) compared to adequate level (23.8%, 11.8%. 9.6%, 8.4), respectively.
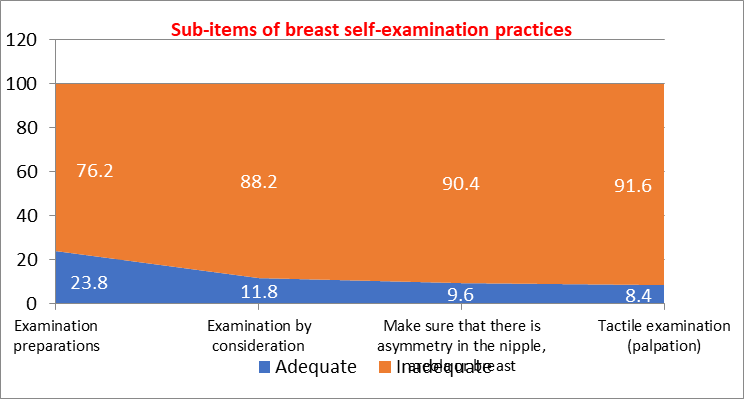
Figure 9: Percentage distribution of the studied female workers regarding their Sub-items of breast self-examination practices (n=323).
Figure (10) illustrates that female workers’ total practice level regarding breast self-examination, less than one-tenth (9.9%) of the female workers having adequate practice compared to 90.1% inadequate.
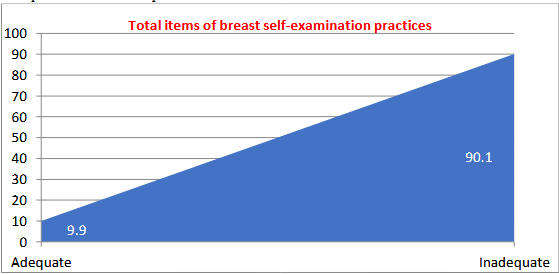
Figure 10: Percentage distribution of the studied female workers regarding their Total-items of breast self-examination practices (n=323).
Figure (11) presents the source of information about breast cancer, less than half (44.9%) of them get information from social media.
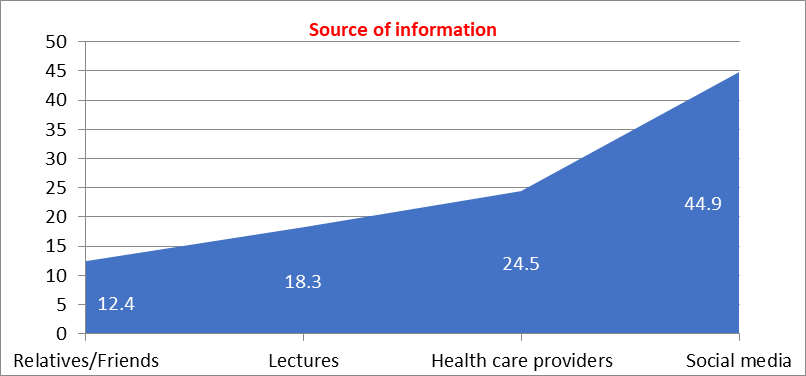
Figure 11: studied female workers regarding their source of information about breast cancer.
Table (1) and Figure (12) reveals that there was a highly statistically significant relation between the studied female workers total practices level regarding breast self-examination score with their educational level and place of residence, as P-value = 0.000 & 0.001, respectively.
| Items | No. | Inadequate (n=291) | Adequate (n=32) | X2 p value |
| % | % | |||
| Age | ||||
| 20 > 30 yrs. | 89 | 25.7 | 1.9 | 9.003 (0.011*) |
| 30 > 40 yrs. | 164 | 43.4 | 7.4 | |
| ≥40 yrs. | 70 | 21.0 | 0.6 | |
| Educational level | ||||
| Intermediate education | 97 | 28.5 | 1.5 | 28.533 (0.000**) |
| University education | 148 | 43.7 | 2.2 | |
| Above university | 78 | 17.9 | 6.2 | |
| Marital status | ||||
| Single | 53 | 16.0 | 0.3 | 6.297 (0.043*) |
| Married | 245 | 66.6 | 9.3 | |
| Divorced | 25 | 7.5 | 0.3 | |
| Place of residence | ||||
| Rural area | 100 | 30.4 | 0.6 | 10.146 (0.001**) |
| Urban area | 223 | 59.7 | 9.3 | |
| Monthly income of family | ||||
| Enough and increases | 13 | 4.0 | 0.0 | 4.360 (0.113) |
| Enough | 272 | 74.6 | 9.6 | |
| Not enough | 38 | 11.5 | 0.3 |
| Not enough | 38 | 11.5 | 0.3 |
Table 1: Relation between socio-demographic characteristics of the studied female workers and their total practices level regarding breast self-examination (n=323).
* Statistically significant at p≤0.05 ** Highly statistical significant at p≤0.01
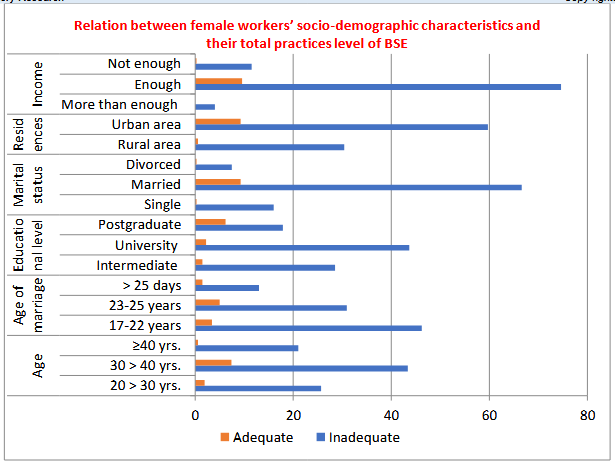
Figure 12: Relation between socio-demographic characteristics of the studied female workers and their total practices level of breast self-examination.
Figure (13) illustrates a statistically significant relation between family history of breast cancer and their total practices level of breast self-examination as P-value = 0.018
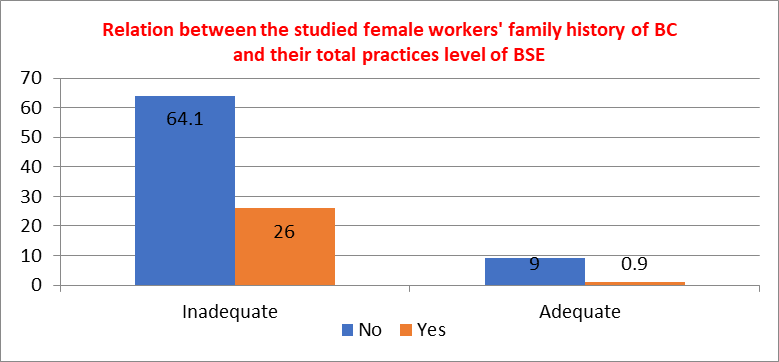
Figure 13: Relation between the studied female workers' family history of breast cancer and their total practices level of breast self-examination (p= 0.018*).
Figure (14) illustrates that there was no statistically significant relation between of the studied female workers and their total practices level regarding breast self-examination as p= 0.414.
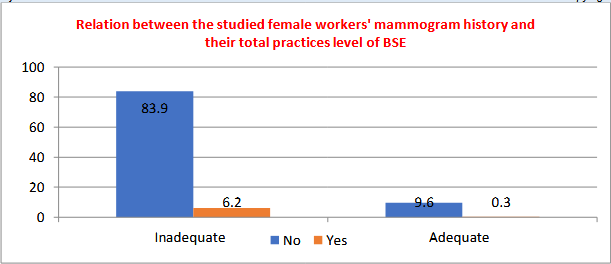
Figure 14: Relation between the studied female workers' mammogram history and their total practices level of breast self-examination (p= 0.269).
Figure (15) illustrates that there was no statistically significant relation between history of breast problems of the studied female workers and their total practices level regarding breast self-examination as P= 0.513
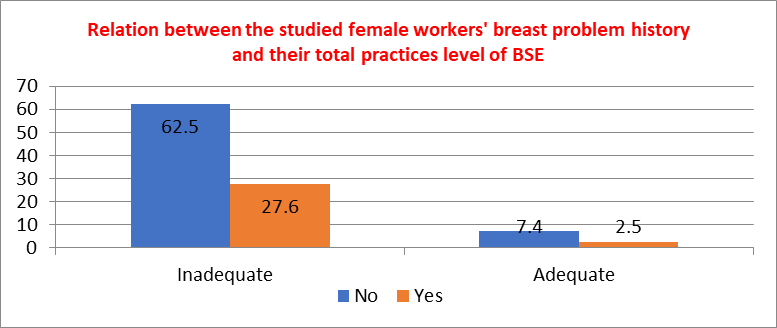
Figure 15: Relation between the studied female workers' breast problem history and their total practices level of breast self-examination (p= 0.339).
Figure (16) illustrates that there the source of information about breast cancer, there is a highly statistically significant relation with their total practice level of breast self-examination as P-value = 0.000.
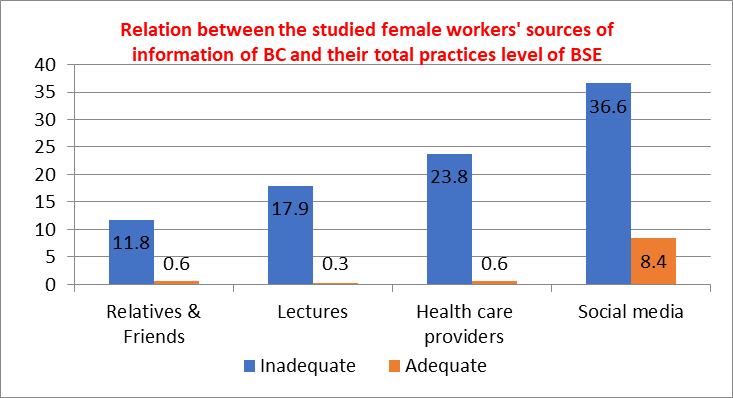
Figure 16: Relation between the studied female workers' sources of information of breast cancer and their total practices level of breast self-examination (p=0.000**).
Self-examination of breasts helps women identify changes and identify breast cancers early, especially after menstruation, as many breast cancers are discovered by women themselves [12-17]. The aim of the study was assess female workers’ total practices regarding breast self-examination at Beni-Suef University. Regarding items for practice of breast self-examination (BSE) the current study announced that most of participated women had inadequate practices of breast self-examination regarding all sub-item (Examination preparations, Examination by consideration, Make sure that there is an asymmetry in the nipple, areola, or breast, and Tactile examination or palpation). The finding was in the same line with Akarsu & Andsoy (2022) [18]. Concerning total BSE practices, it noticed that majority of females had inadequate practice regarding BSE. This finding was in the same line with Alameer et al. (2018) [19]. Regarding the source of information about breast cancer, the current study illustrated that less than half of female workers get information from social media. This finding disagrees with Hajian and Auladi (2015), who studied “awareness, attitude, and practice of breast cancer screening women, and the associated socio-demographic characteristics, in northern Iran” and reported that the source of information was health care workers, and magazines, books, and brochures were the most common sources [20]. From the researcher's point of view, this finding might be due to a lack of breast cancer mass programs, and the majority of studied women did not have a family history of breast cancer. The study found a significant relationship between socio-demographic characteristics and breast self-examination practices among female workers, with age pretest showing a significant association, while no significant relationship was found for the minority aged 30-40 years, similar to Mahmoud et al.'s 2020 findings [21]. Moreover, the study found a significant relationship between female workers' breast self-examination practices and their educational level, with university-educated females having adequate practice. This supports Ahmed and Shrief's (2019) findings, suggesting that education improves understanding and application of BSE steps [22]. Additionally, the study found no significant relationship between female workers' breast self-examination practices and their family income. However, a minority of females with sufficient monthly income had adequate practice, contradicting previous research suggesting a link between income and BSE practice Dündar et al. (2006) and Marinho et al. (2008) [23-24]. Also, there was a statistically significant relationship between the studied female workers total practices level of breast self-examination score with their marital status level. In which less than one-tenth of married women had adequate practice regarding breast self-examination. This finding is also in the same line with Montazeri et al. (2008), who clarified that performing BSE was significantly related to age, marital status, and educational level. Regarding place of residence, there was a highly statistically significant relationship between the studied female workers total practices level of breast self-examination score and their place of residence [25]. In which the minority of females who lived in urban areas had adequate practice regarding breast self-examination. This finding is similar to Mahmoud et al. (2020), who showed that there is a statistically significant association between women's total practice scores and residence. From the researcher's point of view, females who live in urban areas have the ability to receive information and practice BSE, even if it causes embarrassment. Unlike women who live in rural areas [21]. For the relationship between the family history of breast cancer of the studied women and their total practice level of breast self-examination, the results revealed a statistically significant relationship. In which the minority of females who didn’t have a family history of breast cancer had adequate practice regarding breast self-examination. Also, this finding is supported by Meilina et al. (2024), who investigated “the relationship of knowledge, attitudes, and family history of breast cancer to breast self-examination (BSE) behavior in women” and revealed that there was no relationship between family breast cancer history and BSE [26]. Concerning the relation between the studied female workers' mammogram history and breast problem history and their total practice level of breast self-examination, the results revealed that no statistically significant relationship was found for both. However, the majority of females who have neither breast problem nor mammogram history had inadequate practice regarding breast self-examination As regard the source of information about breast cancer, there was a highly statistically significant relationship with their total practice level of breast self-examination. In which the minority of females who get their information from social media have adequate practice regarding breast self-examination. This finding is similar to Parsa et al. (2008), who assessed “knowledge and behavior regarding breast cancer screening among female teachers in Selangor, Malaysia” and revealed that there was no significant association between the sources of information and breast cancer screening practices [27].
Based on the findings of the present study, it can be concluded that there were statistically significant relation between the studied female workers total practices level regarding breast self-examination score with their educational level and place of residence, family history of breast cancer. A highly statistically significant relation with their total practice level of breast self-examination and source of information was observed.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
