
Research Article | DOI: https://doi.org/10.31579/2690-8808/203
Department of Public Health, Faculty of Health Science, Imo State University Owerri.
*Corresponding Author: Nwanyaka Henry Ifeanyi, Department of Public Health, Faculty of Health Science, Imo State University Owerri.
Citation: Nwanyaka H. Ifeanyi and Okemma E. Uwaezu (2024), Female genital mutilation's effects on women's physical, mental, and social health, J, Clinical Case Reports and Studies, 5(5); DOI:10.31579/2690-8808/203
Copyright: ©, 2024, Nwanyaka Henry Ifeanyi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 June 2024 | Accepted: 17 June 2024 | Published: 26 June 2024
Keywords: physical, psychological, social health genital mutilation
The non-medical cutting or removal of some or all of the external female genitalia is known as female genital mutilation, or FGM. Physical health issues such scarring or keloids formation, infertility, infections, and irregular menstruation are reported to result from it. In addition, it causes perineal tears, protracted labor, and postpartum hemorrhage, among other difficulties during labor and delivery. Depression, low self-esteem, and post-traumatic stress disorder are possible psychological outcomes. Sexual dysfunction, including arousal, orgasm, lubrication, and satisfaction, can lead to a loss of connection for sufferers and, indirectly, for significant others. The purpose of this study was to ascertain the impact of female genital mutilation on the body, society, and mind. There were 200 FGM and 200 non-genital multination participants in this study. The impacts of female genital mutilation (FGM) on the victims' social, psychological, and physical well-being were assessed. The family of FGM group (N = 129) had a monthly family income of 50000 Naira or less, compared to 46 families (23%) earning 50000-100000 and 25 families (12.9%) having an income above 100000 naira. With regard to employment, 63 fathers (31.5%) described themselves as Traders. 55 (27.5%) of them were farmers, 18 (26.6%) of them were skilled workers, Civil Servants 42 (21%), and Self-employed 32 (16%). 8 (4%) fathers were retired. There are no differences between this group and the other. The findings showed that female with genital mutilation, had greater rates of somatic disturbance, anxiety disorder, and depression than those without female without genital multilation. Therefore, this study offers additional proof to medical professionals so they may start providing FGM patients with high-quality care right away.
Female genital mutilation (FGM), comprises none medical removal of some parts or the complete external female genitalia. This simply means that it is a traditional practice in which the female genital organs are partly or completely removed for cultural or other non-therapeutic reasons (Berg and Dennison). It is practiced in many Africa and in some countries in the Middle East and Asia. However, there is limited data, it is speculated that female circumcision is practiced by immigrant communities in a number of countries. It is forbidden by law in various African and Western countries [1].
The current WHO classification describes four types of female circumcision: Type I known as clitoridectomy, consist of partial or complete removal of the clitoris and/or the prepuce. Type II also refers to as excision, comprises partial or complete removal of the clitoris and the labia minora, with or without excision of the labia majora. Type III known as infibulation, involves narrowing of the vaginal orifice with creation of a covering seal by cutting and appositioning the labia minora and/or the labia majora, with or without excision of the clitoris. Type IV, other, involves all other harmful procedures to the female genitalia for non-medical purposes, for instance: pricking, piercing, incising, scraping and cauterization. There is differences in prevalence, reflecting ethnicity, tradition and sociodemographic factors [2,3]
This practice of female circumcision is based on social conventions with regards to psycho-sexual and social reasons including control of women’s sexuality and family honor which is implemented by the community [4]. This is known to result to physical health problems such as scaring or formation of keloids, infertility, infections as well as menstrual abnormalities. It equally causes complications during labor and delivery, which involves a long period of labor, perineal tears and hemorrhage after delivery [5]. Psychological disorders are major effects such as depression, low self-esteem and indeed post-traumatic stress syndrome. Social health problems to victims of FGM and indirectly to others may include lack of intimacy related to sexual disorders like arousal, orgasm, lubrication and satisfaction [6,7] The practice of FGM is common in some African countries. The effects of this FGM have global impacts. Some frantic efforts are being made to try and reduce the suffering of the victims as well as trying to stop the practice by educating communities. This has been done through their leaders, men involvement and coming up with strategies and policies that protect the rights of women against such gender based violence [8,9]
Female genital mutilation is recognized as a harmful practice which abrogates human rights. It is linked to various health problems such as intensive pain, bleeding, shock, infections, and difficulty in passing urine and faeces. Caesarean section, blood loss, and increased perinatal mortality are associated birth risks. This in other words results in psychological, social and physical consequences [10,11].
Indeed, some works have been carried out on female circumcision but still there is literature gap on the global physical, social and psychological effects of Female genital mutilation. The effects of Female genital mutilation need to be studied particularly on the victims as the study group and the survivors as the control group. Such studies may provide some significant evidence to healthcare providers to effectively commence high standard medical care to both the victims and the survivors of female genital mutilation.
Study area
The study area was in south East Nigeria
Population
The estimated population is 25.8 million and the population density varies from 230-1,400 people per square kilometer.
Study design
Descriptive and analytical study designs were used in this study. This included and knowledge, attitude and perception studies. Descriptive design was used to investigate the distribution of FGM. Women who had female genital mutilation aged between 12 and 14 were involved and non FGM served as control
Method of data collection
Research instrument for data collection were questionnaires, Personal Interview and Telephonic Surveys
Questionnaires
Well structured questionnaires will be used to obtain data from respondents; the questionnaires were arranged in the following order:
Questionnaire 1
This was used to elicit information from the general populace. It will be organized into the following sections:
Section A: Demographic data
Section B: Knowledge of female genital mutilation
Section C: Social impact of female genital mutilation
Section D: Physical impact of female genital mutilation
Section E: Physiological impact of female genital mutilation
Validity of research instrument
The questionnaires was well structured according to the two categories of respondents: namely; those with FGN and those without FGN
Reliability of research instrument
In order to make the research instruments reliable, pilot or test studies was carried out using five copies of each of the two different categories of questionnaires which were administered to the respective groups of respondents. After an interval of two weeks, another set of five copies of the same instruments was administered on different sets of respondents. At the end of these preliminary studies, the questionnaires were then fine tuned and structured to attain the highest reliability standard.
Ethical consideration
Letters of approval/permission to administer questionnaires on respondents were presented to management of health institutions for approval before they were administered to respondents. Also, the consent of those with FGM were sought for before they were presented with questionnaires. Similar consent were sought from those without FGM.
Statistical analysis
Generated data will be put into Tables and Charts. The data were analyzed using the Statistical Package for the Social Sciences, SPSS version 11.0 for Windows. Descriptive statistics was used to present the characteristics of the sample.
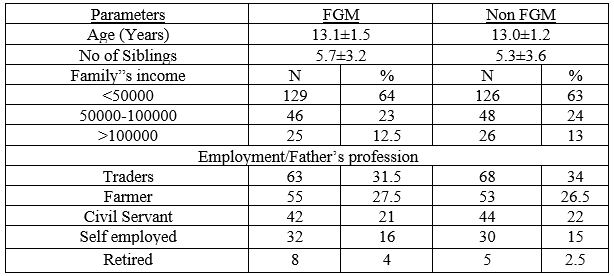
Table 1. Comparison of FGM and non FGM with respect to demographic variables
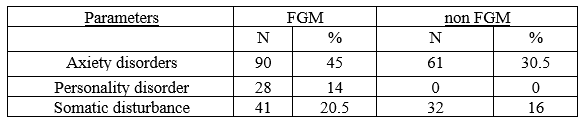
Table 2: Psychological disorders in FGM and Non FGM
| Groups | Depression | Self esteem |
| FGM | 34.10±3.8 | 24.23±4.21 |
| Non FGM | 11.53±2.1 | 8.41±2.80 |
Table 3: Sociological disorders in FGM and Non FGM
| Groups | Scars | Pains |
| FGM | 14.26±3.7 | 11.53 ±4.1 |
| Non FGM | 2.11±3.1 | 3.0±2.6 |
Table 4: Physical impact in FGM and Non FGM
According to the study's findings, female genital mutilation is probably going to lead to a range of emotional problems, which could lead to psychological diseases. It was discovered that the high rate of depression was higher than average. These results are consistent with earlier research on abused and traumatized youngsters. The study's findings also shown that self-esteem and depressive symptoms together formed an index with statistical significance that could be used to distinguish between the two groups [12,13]
The findings suggest that cultural embedding does not prevent the onset of depression, even though female genital mutilation is a part of the individuals' ethnic heritage [14]. While the study's findings lend credence to the idea that female genital mutilation has a significant detrimental effect on mental health that extends beyond physical issues, care should be taken when interpreting the findings [15,16]
Furthermore, there is a growing movement against female genital mutilation in public spaces like schools where people are taught about its harmful effects [17,18]. Because of this, the way the trauma is assimilated may alter depending on whether or not circumcision is more common. Of course, there are a plethora of additional variables that could also have a significant impact on the mental health outcome, including coping mechanisms, past traumatic experiences, information before to circumcision, and sexual encounters [19,20].
However, this study offers yet another compelling reason in favor of disseminating culturally grounded knowledge that may aid in the elimination of female genital mutilation. In keeping with psychology's growing contribution to the documentation of violations of human rights, it is critical to support women experiencing mental distress and to carry out additional study [21]. Researchers and doctors should focus more on the urgent needs of FGM girls and women, as demonstrated by the startlingly high prevalence of psychological disorders among this population of FGM girls.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
