
Research Article | DOI: https://doi.org/10.31579/2692-9392/161
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Lecturer of Obstetrics & Gynecology Faculty of Medicine, Beni-Suef University.
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Fatima Hosny Abd-ELhakam, Rasha El-Syed Ebrahim, Momen Zakria Mohammed and Hanan Elzeblawy Hassan , (2022) Rel Female Genital Mutilation: Impact on Knowledge, Attitude, Sexual Score Domains and Intention of Females in Northern Upper Egypt. Archives of Medical Case Reports and Case Study, 6(5); DOI:10.31579/2692-9392/161
Copyright: © 2022, Hanan Elzeblawy Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 November 2022 | Accepted: 12 December 2022 | Published: 30 December 2022
Keywords: female genital mutilation; knowledge; attitude; intention; sexual domains
Background: Female genital mutilation/cutting is extensively done in societies where it is believed to promote marriageability. As a result, the practice of FGM/C will continue because parents believe it will provide a better future for their daughters, and some girls may even desire to be mutilated to find a husband.
Aim: The aim of this study was Estimate effect of FGM on Females' knowledge, Attitude, Sexual Score Domains, and Intention in Northern Upper Egypt.
Subject & Methods: A descriptive cross-sectional study was used. The study population consisted of 2837 females in family health centers (FHCs) in different sitting at Beni-Suef.
Tool: Α Structured Interviewing Questionnaire sheet was used to collect data related females' knowledge, attitude, and intention. Female Sexual Function Index (FSDI) to assess female sexual function.
Results: The prevalence of Female Genital Mutilation (FGM/C) among total participants at Beni-Suef is 71.4%. Good knowledge score (27%) was more prevalent among non-mutilated females. Unfavorable and neutral attitude score (49.3%) was more prevalent among females with FGM. that there was a significantly higher Desire domain (5.8±1.8), Arousal domain (13.7±2.9), Lubrication domain (16±3.4), Orgasm domain (11.7±2.6), Satisfaction domain (13.3±2.4), and Total score among not circumcised married participants than circumcised ones but the Pain domain didn't differ significantly between circumcised (9.7±3.3), and not circumcised (9.3±2.2). About 79.4% of females who experienced FGM/C had the intention to mutilate their daughters in the future.
Conclusion: Good knowledge score was more prevalent among non-mutilated females. There was a significant relationship between FGM and knowledge, attitude, Sexual Score Domains, and intention to mutilate their daughters in the future (p-value <0.001).
More than 31 countries in Africa, a few in Asia, and the Middle East all practice female genital mutilation or circumcision. (UNICEF, 2018). According to UNICEF, FGM/C global databases (February 2020), the prevalence of FGM/C in Uganda became 0% compared to a quarter within the update on February 2018. The prevalence of FGM/C among females aged 15 - 49 years ranged from 1% in Cameroon to 98% in Somalia, while among girls aged 0 - 14 years it has ranged between 0.1% in Benin and 83% in Mali (UNICEF, 2020). The prevalence of FGM/C exceeds 90% in Guinea, Djibouti, and Mali, while it is about 10% in Niger, Ghana, Togo, and Benin (UNICEF, 2020).
In Egypt, although the prevalence of FGM/C among females aged 15- 49 declined from 97% in 1985 to 87% in 2015, the prevalence remains high despite governmental efforts (MOHP, et al., 2015). The prevalence of FGM/C among adolescent girls and women has dropped from 94% in 2008 to 88% in 2014(Alkhalaileh, et al., 2018).
Female genital mutilation/cutting has complicated social and cultural foundations that outweigh the requirements and ideas of individuals. Female genital mutilation/cutting is seen as a normal part of female socialization in societies that practice it. The reasons for continuing FGM/C in these societies include religious obligations, beauty in the form of smooth and small genitalia, delighting future families and sexual partners, having social significance, and being accepted for marriage (Matanda, et al., 2018).
Female genital mutilation/cutting is extensively done in societies where it is believed to promote marriageability. As a result, the practice of FGM/C will continue because parents believe it will provide a better future for their daughters, and some girls may even desire to be mutilated to find a husband. The hypothesis also suggests that in places where FGM/C is a part of the culture, no one will want to stop doing it because families are afraid of deviating from community norms (UNICEF, 2016).
The present study was carried find out about FGM in Beni-Suef Governorate through:
3.1. Research Design: A Descriptive Cross-sectional study was used to achieve the aim of the current study.
3.2. Subjects & Setting:
3.2.1. Setting: The study was conducted in family health centers (FHCs) in different sitting at Beni-Suef Governorate. Beni-Suef governorate is divided into seven sectors. From every sector the MCH was randomly selected to geographically represent the sector. As the following mention:
Salah Salem MCH and Eastern MCH, Taha Bosh MCH was selected, Beba Medical Center, Tarshoup, Bani Saleh MCH, Al-shantour MCH, El-Mamalik MCH, Elnouira MCH, Kamen El-Arouse MCH.
3.2.2. Sample:
3.2.2.1. Sample Type:
3.2.2.2. Sample size:
The study population consisted of all females who were accepted to participate in the study at the time of data collection (A period of six months from the start of data collection) and will be included in the study.
3.3. Tools of Data Collection:
A pre-designed structured questionnaire was used to collect data. Data were collected through personal interviews. The questionnaire is divided into six sections:
Section I: А Structured Interviewing Questionnaire sheet which includes the following parts: age, residence, level of education, marital status, occupation and experience with mutilation, etc……
Section II: Knowledge of females regarding FGM/C: Females' knowledge was assessed using both single-response and multiple-response questions.
a. Single response questions:
They included knowledge of females about the spread, types, and procedures of FGM/C, side effects, and health consequences of FGM/C and FGM/C in Egyptian law.
Scoring system
Multiple response questions:
They included knowledge of females regarding the immediate and long-term health consequences of FGM/C. Participants were expected to select the right responses and not select the wrong responses.
Scoring system
The scores are then turned into percentages, and the overall score is divided into the following categories:
Section III: Attitudes of females regarding FGM/C:
A Likert scale was used to assess attitudes, ranging from agree to disagree. FGM/C from a social standpoint; FGM/C and its effect on female genitalia; FGM/C violation and disability; FGM/C from a religious standpoint; FGM/C practice encouragement in society; FGM/C and marriage; and finally, FGM/C law were all included.
Scoring system
The scores are then turned into percentages, and the overall score is divided into the following categories:
Section IV: Intention to practice FGM/C: It included questions about the following:
Section V: Reasons for practicing FGM/C and reasons for refusing FGM Section
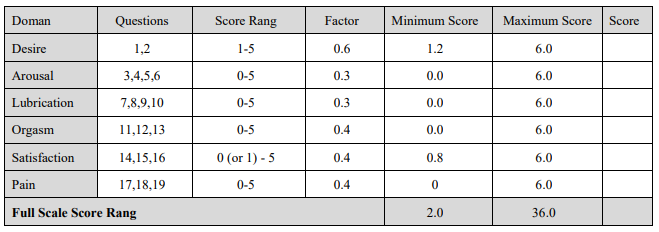
VI: Female Sexual Function Index (FSDI).
A four-week self-reported questionnaire that examines the key characteristics of female sexual function. It consists of 19 multiple-choice questions that assess six domains. Each dimension was rated on a scale of 0/1 (no sexual activity or sexual dysfunction) to 5 (complete sexual activity).
Researchers used the Arabic version of the FSFI, which was translated by (Anis, et al., 2011), to determine the full-scale score. The domain score is calculated by summing the scores of the domain's questions and multiplying the total by the domain factor. (=2 to 36). It was approved for use among Egyptians.
For the Arabic version of the FSFI, a total score of 28.1 was used as the cutoff point to distinguish between women with FSD and those with normal functions (sensitivity 96.7%, specificity 93.2%). The scale has been translated into Arabic.
Scoring system for (Female Sexual Function Index) (FSDI):
A formula can be used to calculate the FSFI's individual domain scores and full-scale (overall) scores. Add the scores of the individual items that make up the domain and multiply the total by the domain factor.
For the Arabic version of the FSFI, a total score of 28.1 was used to discriminate between women with FSD and those with normal functions. A domain score of 0 implies that the subject reported no sexual activity in the previous month within the specific domains.
3.4. Validity of the Tool
All tools were tested for content validity by а jury of five experts in the obstetrics and gynecological nursing, pediatric nursing professor and one from biostatistics field.
3.6. Reliability of the Tool
Reliability of tools was tested by using Cronbаch’s Alphа coefficient test. Consisted of relatively homogenous items as indicated by high reliability which was (0.405) for knowledge and (0.764) for attitude.
3.7. Ethical Considerations:
Informed consent was taken from each female to participate in the study after explaining the purpose of the study, and its importance for her, it will haven’t any harmful effect on them, the information will be confidential and they can withdraw from the study at any time.
3.8. Administrative Considerations:
Official permission was obtained by submission of an official letters from the Faculty of Nursing, Beni-Suef University to the responsible authorities of the study setting (family health centers (FHCs)) to obtain their permission for data collection for our study. These letters provided the study's goal as well as photocopies of data collecting materials to obtain their consent and assistance with data collection.
3.9. Pilot Study
The pilot study was conducted on 10.0% of the total sample to test the feasibility & the applicability of the tool, find out the possible obstacles or problems that might face the researchers and interfere with data collection, detect any problems peculiar to the statements as sequence of questions, clarity and estimate the time needed for data collection. The samples of the women included in the pilot study were excluded from the main study sample
3.10. Field Work
The process of data collection was carried out in the period from November 2021 and completed by April 2022, 3 days/week Saturday, Tuesday and Thursday from 9am to 2pm in three phases: The researcher begins filling out the interviewing questionnaire to assess women's demographic characteristics, knowledge of FGM/C, attitudes toward FGM/C, intention to practice FGM/C, reasons for practicing FGM/C, and reasons for refusing FGM/C, and Female Sexual Function Index (FSDI). The instruction was given to each woman individually for 3 sessions each session ranging from 15-20 minutes on an individual.
3.11. Statistical Analysis
All data were collected, tabulated and statistically analyzed using IBM SPSS 25. Data was supplied, and appropriate analysis was performed for each parameter based on the type of data obtained.
3.11.1. Descriptive Statistics data were expressed as:
3.11.2. Analytical Statistics:
3.11.3. Graphical presentation:
Figure (1): Presents Female Genital Mutilation Experience among Participant Study Sample. The prevalence of Female Genital Mutilation (FGM/C) among total participants (2837) at Beni-Suef is 71.4%.
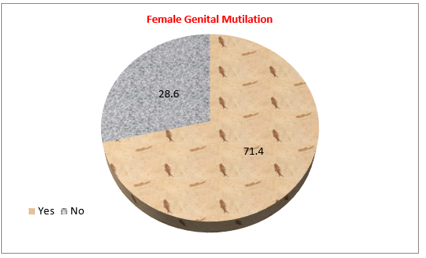
Figure (1): Female Genital Mutilation Experience among Participant Study Sample
Figure (2) showed an association between participants' total knowledge and their exposure to FGM. Good knowledge score (27%) was more prevalent among non-mutilated females. Also, fair knowledge was more prevalent (51.9%) among un-circumcised ones. While poor knowledge score (37.1%) was more prevalent among females with FGM There was a significant relationship between circumcision and participant knowledge (p-value <0>
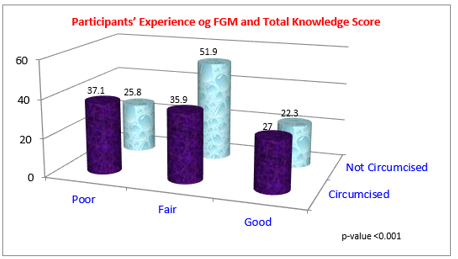
Figure (2): Participants’ Experience of FGM and Total Knowledge Score
Figure (3): Presents Association between Participants’ Experience of FGM and their Total Attitude score. It showed an association between experience of FGM and total Attitude score among participant females. Unfavorable and neutral attitude score (49.3%) was more prevalent among females with FGM, while the favorable attitude (52%) was associated with the absence of FGM. There was a significant relationship between FGM and the participant's attitude.
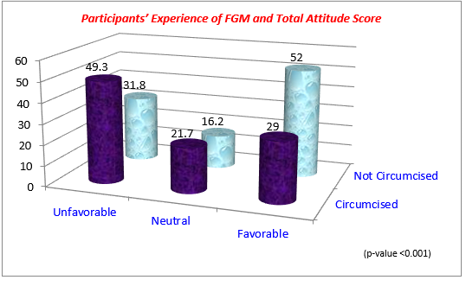
Figure (3): Participants’ Experience of FGM and Total Attitude Score
Figure (3): Participants’ Experience of FGM and Total Attitude Score
Table (1) Presents the Association between FGM and the Sexual Score Domains and Total Score. It showed that there was a significantly higher Desire domain (5.8±1.8), Arousal domain (13.7±2.9), Lubrication domain (16±3.4), Orgasm domain (11.7±2.6), Satisfaction domain (13.3±2.4), and Total score among not circumcised married participants than circumcised ones but the Pain domain didn't differ significantly between circumcised (9.7±3.3), and not circumcised (9.3±2.2).
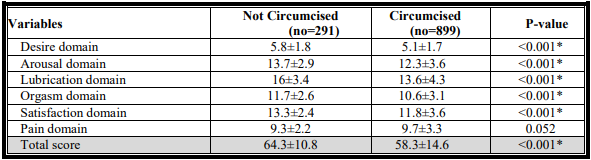
*P-value is significant (p less than 0.001)
Figure (4): Presents Participants’ Experience of FGM and Intention of Mutilating their Daughters. An association between females' intention of mutilating their daughters and their mutilation experience was found. About 79.4% of females who experienced FGM/C had the intention to mutilate their daughters in the future, while only 20.6% of females who did not experience FGM/C had the intention to mutilate their daughters in the future.
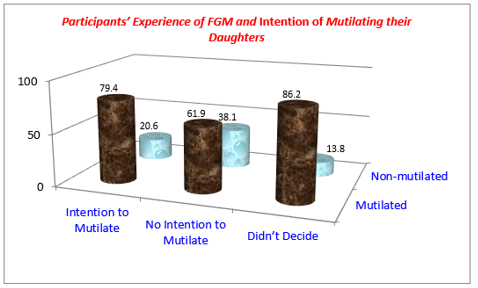
Figure (4): Participants’ Experience of FGM and Intention of Mutilating their Daughters
The results of the current study revealed that the prevalence of Female Genital Mutilation (FGM/C) among total participants was 71.4%. This result is in accordance with other researches. In Nigeria, according to a 2013 Department of Health (DHS) report, one in every four women aged 15 to 49 has had FGM, with 82% of the procedures occurring before the age of five. The prevalence of FGM in Nigerian women aged 15 to 49 has been steadily decreasing, from 30% in 2008 to 25% in 2013 (Ogbuoji, 2017). According to a study conducted in 2020 in the southern-eastern part of Nigeria, FGM was found to be 13.4% prevalent (Obijiofor, et al., 2020).
A study of Iraqi Kurdish females indicated that 70.3 percent of the participants had undergone FGM/C, but only 58.6 percent of them had been mutilated when clinically assessed. Female genital mutilation was most common in Erbil (62.9%) and Sulaimany (55.8%) governorates in Iraq's Kurdistan Region (Shabila, 2019). According to a study conducted in Iran, FGM was found to be prevalent in 50.5% of the population between the ages of 21 and 30 (Bahrami, et al., 2018).
Several nations, including Sudan, Ethiopia, and Nigeria, have conducted studies on females' knowledge of FGM. FGM is viewed differently by girls and women in different countries. Mali, Sierra Leone, Guinea, and Somalia had the highest levels of support for FGM, with more than half of the female population believing the practice should continue (Abolfotouh, S. M & Abolfotouh, M. A, 2015).
Significant statistical relationship between participants' experiences to FGM and their total score of knowledge was revealed (p-value <0>
The understanding of females, males, midwives, and health care practitioners regarding FGM/C was the subject of much of the research, which was largely conducted in African countries. They intended to look at their participants' basic knowledge and attitudes about FGM/C, as well as its determinants, to see whether any intervention strategies could assist abolish the practice (Adigüzel, et al., 2019). Other research was conducted in the Eastern Mediterranean region, Europe, and the United States (Ahmed, et al., 2018; González-Timoneda, et al., 2018).
Regarding the association between attitudes and FGM, the result of the current study revealed that unfavorable attitude score was more prevalent among mutilated females, while the favorable attitude was associated with the absence of FGM. There was a significant relationship between FGM and the participant's attitude(p-value <0>
FGM/C is extensively done in societies where it is believed to promote marriageability. As a result, the practice of FGM/C will continue because parents believe it will provide a better future for their daughters, and some girls may even desire to be mutilated to find a husband. The hypothesis also suggests that in places where FGM/C is a part of the culture, no one will want to stop doing it because families are afraid of deviating from community norms (UNICEF, 2016).
Regarding the effect of FGM/C on Female Sexual Function there was a significantly significant total score of among not mutilated married participants than mutilated ones. This is agreeing with other studies that reported that un-mutilated subjects scored considerably higher on desire, arousal, lubrication, orgasm, and satisfaction than the mutilated participants. Regarding the sexual pain domain, no apparent difference between the two groups was reported. (Anis, et al., 2012; Ismail, et al., 2017) According to a study conducted by KHEIR, et al., (2017); the study suggests that FSFI domains were significantly lower in women with FGM: for desire, arousal, lubrication, orgasm, satisfaction, and pain (Pérez-López, et al., 2020). In contrast, in a study conducted in Sudan, there were no discernible differences between mutilated and non-mutilated women in terms of desire arousal, orgasm, or pain. This lack of discernible changes could be attributed to the traditional obligation of most women to conceal these experiences (KHEIR, et al., 2017).
Concerning participants’ experience of FGM and intention of mutilating their daughters; an association between females' intention of mutilating their daughters and their mutilation experience was found. Most of females who experienced FGM/C had the intention to mutilate their daughters in the future, while females who did not experience FGM/C had the intention to mutilate their daughters in the future. This may attribute to that culture, education, and residence play a curial role in individual intention. This is close to a study conducted in Iran that revealed that intention decrease with an increased level of education (Pashaei, et al., 2012).
Good knowledge score was more prevalent among non-mutilated females. There was a significant relationship between FGM and knowledge, attitude, Sexual Score Domains, and intention to mutilate their daughters in the future (p-value <0>
1.Study Knowledge, attitude, and practice of medical care providers regarding FGM/C.
2.Inter-sectorial cooperation is being used by the MOHP, the Ministry of Justice, and the National Counsel for Women, the Egyptian Medical Syndicate, and the media to carry out a national program aimed at stopping FGM/C by healthcare professionals.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
