
Research Article | DOI: https://doi.org/10.31579/2692-9406/139
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Lecturer of Obstetrics & Gynecology Faculty of Medicine, Beni-Suef University.
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Fatima Hosny Abd-ELhakam, Rasha El-Syed Ebrahim, Momen Zakria Mohammed and Hanan Elzeblawy Hassan (2023), Female Genital Mutilation: Females' Related Knowledge. Biomedical Research and Clinical Reviews. 8(1); DOI:10.31579/2692-9406/139
Copyright: © 2023, Hanan Elzeblawy Hassan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 November 2022 | Accepted: 21 December 2022 | Published: 19 January 2023
Keywords: female genital mutilation; knowledge
Background: According to a representative from the United Nations Population Fund in Cairo, Egypt's rate is so high that it accounts for one-fourth of all cases worldwide. Female genital cutting roots are unknown, but it is supposed to predate all religions, including Judaism, Christianity, and Islam, and to have been performed within all of these religions.Aim: Assess the level of total knowledge of females toward the practice of FGM.Subject & Methods:A descriptive cross-sectional study was used. The study population consisted of 2837 females in family health centers (FHCs) in different sitting at Beni-Suef. Α Structured Interviewing Questionnaire sheet was used to collect data.Results: The most of studied participants (71.2%) their age was 15-30 years old. The majority of studied participants (90.2%) were highly educated. More than half (57.5%) of studied participants were single, round two-thirds (65.4%) of studied participants were students. Only 25.7% of females had good knowledge regarding FGM/C, while 40.5% and 33.8% had poor and fair levels of knowledge, 71.3% of females mentioned that the source of their information about FGM/C was their personal experience. Poor knowledge score (37.1%) was more prevalent among females with circumcision (p-value <0.001).Conclusion: Knowledge score regarding FGM was poor for the most of participants. The main source of females' information was their personal experience. Poor knowledge score was more prevalent among mutilated females.Recommendations: Development of an educational programs and brochures for mothers about FGM is required to increase their awareness.
The expression of “female genital mutilation” began to gain support within the late 1970s because it established a transparent distinction from male circumcision. The word mutilation gave a lightweight to the violation of the act and thus gained national and international support for its elimination (Shell-Duncan, 2022).
According to a representative from the United Nations Population Fund in Cairo, Egypt's rate is so high that it accounts for one-fourth of all cases worldwide (Abdelhafeez, et al., 2020). Female genital cutting roots are unknown, but it is supposed to predate all religions, including Judaism, Christianity, and Islam, and to have been performed within all of these religions (Gharib, 2019). The practice's earliest traces in Africa can be traced back to ancient Egyptian Pharaohs, but some say that FGC has long existed in African cultures as a significant rite of passage from childhood to adolescence and maturity (Werunga, 2020).
Female genital mutilation/cutting Female genital mutilation/cutting Female genital mutilation/cutting Female genital mutilation/cutting is also seen as a technique for cleaning girls in some societies. They believe that FGM/C should be continued as a source of femininity and to protect virginity (WHO, 2020). The concept of the girl as a source of shame influences attitudes toward the continuance of FGM/C. People feel that because FGM/C lowers female desire, it reduces premarital sex and sexual relationships (Khalil & Orabi, 2017).
The procedure of FGM/C is typically applied by knives, scissors, scalpels, glass, or razor blades. Additional damage occurs as a result of poor lighting, non-sterile equipment, and aseptic conditions. The procedure is typically administered by traditional healers, traditional birth attendants, barbers, or health care providers like midwives, nurses, and physicians. Members of the family help the performer by holding the girls to stop their movements and also the procedure usually takes from 15 to 20 minutes betting on the experience of the performer and the resistance of the girls. The age at which FGM/C is completed varies but it's usually done between the age of 4 and 14 years (Odukogbe, et al., 2017).
The present study was carried out to:
1. Assess the level of total knowledge of females toward the practice of FGM
2. Assess Participants' Sources of Knowledge Related to FGM
3. Assess the Effect of Female Genital Mutilation on Females' Related Knowledge
1.1. Research Questions
1. What is the level of knowledge of females regarding the practice of FGM at Beni-Suef.?
2. What are Sources of Knowledge Related to FGM?
3. Is there Relationship between Female Genital Mutilation and Females' Related Knowledge?
3. Subjects and Methods
3.1. Research Design: A Descriptive Cross-sectional study was used to achieve the aim of the current study.
3.2. Subjects & Setting:
3.3.1. Setting: The study was conducted in family health centers (FHCs) in different sitting at Beni-Suef Governorate. Beni-Suef governorate is divided into seven sectors. From every sector the MCH was randomly selected to geographically represent the sector.
3.2.2. Sample:
3.2.2.1. Sample Type:
A Convenient sample was used. The study sample was selected according to the following Inclusion criteria: 18-60 years old women and Can read and write
3.2.2.2. Sample size:
The study population consisted of all females who were accepted to participate in the study at the time of data collection (A period of six months from the start of data collection) and will be included in the study.
3.3. Tools of Data Collection:
A pre-designed structured questionnaire was used to collect data. Data were collected through personal interviews. The questionnaire is divided into six sections:
Section I: А Structured Interviewing Questionnaire sheet which includes the following parts: age, residence, level of education, marital status, occupation and experience with mutilation, etc.,
Section II: Knowledge of females regarding FGM/C: Females' knowledge was assessed using both single-response and multiple-response questions.
a. Single response questions:
They included knowledge of females about the spread, types, and procedures of FGM/C, side effects, and health consequences of FGM/C and FGM/C in Egyptian law.
Scoring system
It received (0) if the answers were wrong or don't know
It received (1) if the answers were incomplete correct
It received (2) if the answers were complete correct
a. Multiple response questions:
They included knowledge of females regarding the immediate and long-term health consequences of FGM/C. Participants were expected to select the right responses and not select the wrong responses.
Scoring system
It received (0) if less than 25% of the answers were correct.
It received (1) if ≥25 percent to less than 50% of the responses were correct.
It received (2) if ≥50% of the answers were correct.
The scores are then turned into percentages, and the overall score is divided into the following categories:
Good level of knowledge ≥75%.
A fair level of knowledge is ≥50% to less than 75%.
Poor level of knowledge less than 50%.
3.4. Validity of the Tool
All tools were tested for content validity by a jury of four expertise in the woman health nursing and one from biostatistics field to ascertain its relevance and completeness.
3.5. Reliability of the Tool
Reliability of the tool (knowledge assessment sheet) was evaluated by using Cronbach‘s Alpha coefficient test. The tool consisted of relatively homogeneous items as indicated by the high reliability. Internal consistency of the second tool = 0.405
3.6. Ethical and Administrative Considerations:
After approval of the research from the nursing college/Beni-Suef University, an official letter was directed from nursing college to the head of MCH Centers at Beni-Suef in order to get his approval to conduct the study after clarifying its aim. Then oral consent was taken from each participant after clarification of the study aim and interventions. Each one was assured about the confidentiality of her data, her right to refuse participation and her right to withdraw from the study without any consequences.
3.8. Pilot Study
A pilot study was conducted on 10.0% of the total subjects to test the clarity and applicability of the study tools. Participants included in the pilot study were excluded from the study subjects.
3.9. Field Work
Data collection was done over a period of six months from the beginning of November 2021till the end of April 2022. The sample was taken three days a week; (Saturday, Tuesday and Thursday) from 9 A.m. to 2 P.m.
3.10. Statistical Analysis
All data were collected, tabulated and statistically analyzed using IBM SPSS 25. Data was supplied, and appropriate analysis was performed for each parameter based on the type of data obtained.
3.10.1. Descriptive Statistics data were expressed as:
3.10.2. Analytical Statistics:
3.10.3. Inter Quartile Range (IQR)
Figure (1) showed that the most of studied participants (71.2%) their age was 15-30 years old.
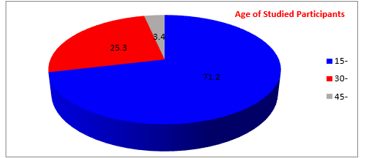
Figure 1: Age of the Studied Participants
Figure (2) showed that the majority of studied participants (90.2%) were highly educated.
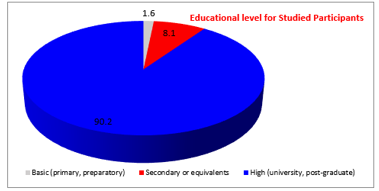
Figure 2: Educational Status of the Studied Participants
Figure (3) showed that the more than half (57.5%) of studied participants were single.
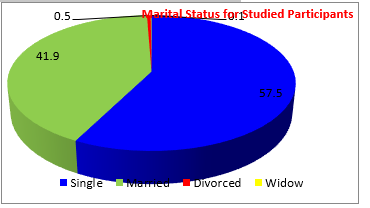
Figure 3: Marital Status of the Studied Participants
Figure (4) showed that around two-thirds (65.4%) of studied participants were students.
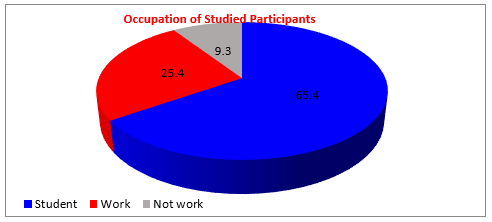
Figure 4: Occupation of the Studied Participants
Table (1): presents the distribution of females aged 18-60 years according to their total knowledge score. Only 25.7% of females had good knowledge regarding FGM/C, while 40.5% and 33.8% had poor and fair levels of knowledge,

Table 1: Total Knowledge Score categories among the studied participants
Figure (5): presents the Studied Participants' Sources of Knowledge Related to FGM. About 71.3% of females mentioned that the source of their information about FGM/C was their personal experience, 36.2% from friends or neighbors, 22% from TV or radio, 22.1% from the internet, 5.1% mentioned religious leaders,10.3% from doctors and nurse, 8% from the lecture about FGM and 0.03% of females read about FGM/C health consequences in books.
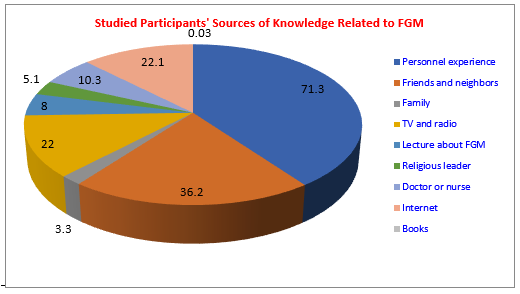
Figure 5: Studied Participants' Sources of Knowledge Related to FGM
Table (2) showed an association between poor knowledge and circumcision. Poor knowledge score (37.1%) was more prevalent among females with circumcision. While fair knowledge was more prevalent (51.9%) among un- circumcised ones. There was a significant relationship between circumcision and participant knowledge (p-value <0>
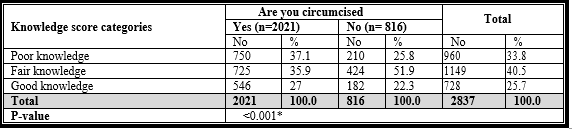
*P-value is significant
Table 2: Association between the Participants’ Knowledge and their Circumcision.
The current study was conducted to assess the level of total knowledge of females toward the practice of FGM, and assess participants' sources of knowledge related to FGM. In the current study, less than one third of females had good knowledge about FGM/C. This may attribute to that the most of the studied females were young aged and rural residents. This result was much lower than results reported in Sudan (Esmeal, et al., 2016) and Nigeria (Ibekwe, et al., 2012) which reported that most females had a good level of knowledge relating to FGM/C.
Several nations, including Sudan, Ethiopia, and Nigeria, have conducted studies on females' knowledge of FGM. FGM is viewed differently by girls and women in different countries. Mali, Sierra Leone, Guinea, and Somalia had the highest levels of support for FGM, with more than half of the female population believing the practice should continue (Abolfotouh, S. M & Abolfotouh, M. A, 2015).
In Mauritania, Ouldzeidoune (2013) discovered that 91.7 percent of females had heard about FGM/C and 64.4 percent of them wanted the practice to continue (had an unfavorable attitude), whereas in Somalia, Adigüzel et al., 2019 discovered that the majority of females had a good level of knowledge about FGM/C, 92.1 percent of them saw FGM/C as a health problem, and 91 percent wanted the practice to be In Ethiopia, females' knowledge and attitudes toward FGM/C varied by area and ethnicity of the interviewees (Melese, et al., 2020).
Additionally, it was lower than Mohammed, et al., (2018) studies' findings, which showed that more than half of the female participants had a good level of understanding. The fact that the present study covered a wide range of FGM/C knowledge topics, including names, occurrence, types, complications, and legalization of FGM/C in Egyptian law, as opposed to other studies that focused primarily on the health issues related to FGM/C, may help to explain the difference in knowledge levels.
Significant statistical relationship between participants' experiences to FGM and their total score of knowledge was revealed (p-value less than 0.001). It showed an association between good knowledge and circumcision. Good knowledge score was more prevalent among mutilated females. This may be due to their exposure to that experience give and encourage them to read and find out information related circumcision.
Knowledge score regarding FGM was poor for the most of participants. The main source of females' information was their personal experience. Poor knowledge score was more prevalent among mutilated females.
Development of an educational programs and brochures for mothers about FGM is required to increase their awareness.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
