
Research Article | DOI: https://doi.org/10.31579/2578-8965/144
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Lecturer of Obstetrics & Gynecology Faculty of Medicine, Beni-Suef University, Egypt.
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Hanan E. Hassan, Fatima H. A. ELhakam, Rasha E. S. Ebrahim, Momen Z. Mohammed. (2023). Female Genital Mutilation: Females' Intention in Northern Upper Egypt. J. Obstetrics Gynecology and Reproductive Sciences, 7(1) DOI: 10.31579/2578-8965/144
Copyright: © 2023 Hanan Elzeblawy Hassan, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 November 2022 | Accepted: 23 December 2022 | Published: 08 February 2023
Keywords: female genital mutilation; intention; northern upper Egypt
Background: Female Genital Mutilation/Cutting is an ancient cultural practice, predating the Bible and therefore the Koran, and has no basis in any religion. It is related to deep social and cultural ideas impeded in several societies regarding femininity and modesty because it is viewed as girls clean and delightful only after being genitally cut. FGM/C is additionally viewed as a protection of virginity, and it prevents premarital sex.
Aim: The present study was carried find out to assess Females' Intention in Northern Upper Egypt regarding Female Genital Mutilation.
Subject & Methods: A Descriptive Cross-sectional study was used. The study was conducted in family health centers (FHCs) in different sitting at Beni-Suef Governorate. A Convenient sample was used. А Structured Interviewing Questionnaire sheet which includes three sections: Socio-demographic data, Intention to practice FGM/C, and Causes for intention or not to practicing FGM/C.
Results: The mean age of the studied participants was 22.6±5. Prevalence of Female Genital Mutilation is 71.4percentage, 29.7percentage of participants are suffering from complications after FGM. About 28.6percentage of females who had mutilated their daughters were planning to mutilate their other daughters in the future. More than one-third of females (35.5percentage) had an unfavorable attitude and 40.5percentage had poor levels of knowledge regarding FGM/C. 71.3percentage of females mentioned that the source of their information about FGM/C was their personal experience.
Conclusion: Northern Upper Egyptian Females' Intention regarding intention of mutilating their daughters was significantly affected by demographic characteristics, level of knowledge, and level of attitude, source information, exposure to complications or pressure from family and neighbors.
Recommendations: Alleviate females' intention toward Female Genital Mutilation should be improving their awareness regarding complications and Egyptian law against FGM, established by improve females' resistance toward family or neighbor regarding bad and harmful traditions.
The terms female genital cutting (FGC) and female genital mutilation/cutting (FGM/C) are often used among practicing communities and individuals. These concepts emphasize the significance of adopting nonjudgmental vocabulary when working with practitioners. When discussing the matter in practice communities, terms like excision or genital cutting are also acceptable [1-7].
The FGM/C is an ancient cultural practice, predating the Bible and therefore the Koran, and has no basis in any religion [8-10]. FGM/C is related to deep social and cultural ideas impeded in several societies regarding femininity and modesty because it is viewed as girls clean and delightful only after being genitally cut. FGM/C is additionally viewed as a protection of virginity, and it prevents premarital sex [11-15].
Sociological causes include what's called “rite de passage” which suggests a transition within the stage of life from girlhood to womanhood and the entrance of the females to the wedding age. These traditions and social norms pass between generations resulting in the continuation of the practice. Psychological causes involve the thought of danger. Some tribes consider the clitoris to be a dangerous organ that has got to be removed. Others see that the removal of the sensitive genital tissues curbs sexual pleasure which successively preserves virginity and chastity and maintains the fidelity of females [16-20].
In Belgium, a study conducted to estimate the number of females who had experienced FGM/C found that 27.4percentage of immigrant females living in Belgium had undergone FGM/C and 8.7percentage of the females were in danger of experiencing FGM/C [21-23].
In Germany, 30percentage of immigrant females from Sub-Saharan Africa had experienced FGM/C before moving to Europe [24-26].
Preventive Strategies of FGM/C:
The eradication of FGM/C necessitates, so WHO reported preventive strategies through three diminutions [28]. (1) Multi-sector: addressing a wide range of issues at multiple levels, including education, justice, finance, women's issues, and health. (2) Sustained: have a long-term impact because progress can be slow. (3) Community-directed projects: have projects driven by communities to assist them in identifying problems, issues, and interventions. These projects aimed at ending FGM/C are non-judgmental and enable people to make their own decisions about whether or not to continue with the practice.
Seven things can be done to assist communities to abandon FGM/C: [29]
Egyptian Strategies & Law for FGM/C prohibition:
First: - the laws:
In 1996, the Ministry of Health issued a decree-law prohibiting the practice of female circumcision, based on the criminal law, which prohibits harm to the body of humans except under medical controls. It should be noted that the criminalization of FGM officially began in 2008 when the Egyptian People’s Assembly (currently the House of Representatives) passed a law punishing the perpetrators of the crime with a fine and imprisonment ranging from three months to two years.
Second: The Legislative Position on Female Genital Mutilation
When the Child Law was amended by Law No. 126 of 2008, the text of Article 242 was added to the Penal Code to toughen the punishment for an intentional wound if it occurred through “female circumcision.”
The new law contains two important articles
Article One: A number of recent legal amendments to the article of the Penal Code relating to female genital mutilation were approved in accordance with Law No. 78 of 2016, which was published in the Official Gazette on September 26, 2016. Article 242 of the Penal Code reads: “A penalty of imprisonment for a period of no less than five Years and not more than seven years for anyone who performs female circumcision by partially or completely removing any of the external genitalia or inflicting injuries on those organs without medical justification".
The penalty shall be hard labor for a period of no less than five years if the person who performs the circumcision referred to in the previous paragraph is a doctor or a practitioner of the profession of nursing. If his crime results in a permanent disability, the penalty shall be aggravated imprisonment for a period of no less than ten years; Temporary imprisonment for a period of no less than fifteen years and not more than twenty years.
In addition to the aforementioned penalties, the court shall decide to deprive its perpetrator, doctors and nurses, of practicing the profession for a period of no less than three years and not more than five years, beginning after the end of the period of execution of the penalty, and the closure of the private facility where the circumcision was performed.
** Replaced by Law No. 10 of 2021 published in the Official Gazette on 4/28/2021
As for the second article, it added to the Penal Code an updated text for the first time, which is the text of Article 242 (a). Anyone who requests female circumcision and it was circumcised at his request, as stipulated in Article 242 of this law, shall be punished with imprisonment.
Anyone who promotes or encourages, or calls in one of the ways set forth in Article (171) of this law to commit the crime of female circumcision, even if there is no effect from his action, shall be punished by imprisonment.
** Replaced by Law No. 10 of 2021 published in the Official Gazette on 4/28/2021
The present study was carried find out to assess Females' Intention in Northern Upper Egypt regarding Female Genital Mutilation
3.1. Research Design: A Descriptive Cross-sectional study was used in the current study.
3.2. Subjects & Setting:
3.2.1. Setting: The study was conducted in family health centers (FHCs) in different sitting at Beni-Suef Governorate. Beni-Suef governorate is divided into seven sectors. From every sector the MCH was randomly selected to geographically represent the sector. As the following mention:
At Beni-Suef sector Salah Salem MCH and Eastern MCH. At Nasser sector Taha Bosh MCH was selected, Beba sector Beba Medical Center and Tarshoup MCH was selected. While Fashen sector Bani Saleh MCH was selected. At Somesta sector Al-shantour MCH was selected. Ehnasia sector El- Mamalik MCH and Elnouira MCH. While Elwasta sector Kamen El-Arouse MCH was selected.
3.2.2. Sample:
3.2.2.1. Sample Type:
A Convenient sample was used.
3.2.2.2. Sample size:
The study population consisted of all females who were accepted to participate in the study at the time of data collection (A period of six months from the start of data collection) and will be included in the study.
3.3 Tools of Data Collection:
A pre-designed structured questionnaire was used to collect data. Data were collected through personal interviews. The questionnaire is divided into three sections:
Section I: А Structured Interviewing Questionnaire sheet which includes the following parts: age, residence, level of education, marital status, occupation and experience with mutilation, etc……
Section II: Intention to practice FGM/C: It included questions about the following:
Section III: Females' Causes for Intention or not to Practicing FGM/C
3.5 Validity & Reliability of the Tool
Α panel of 3 experts in the field of maternity, Obstetrics and Gynecologic Nursing reviewed the tool to test its content validity. Modifications were done accordingly based on their judgment. The reliabilities of the tool were biased on of Cronbаch Αlphа.
3.6. Administrative & Ethical Considerations:
Official permission was obtained by submission of an official letter from the Faculty of Nursing, Beni-Suef University, to the responsible authorities of the study setting to obtain their permission for data collection for the study. All ethical issues were taken into consideration during all the phases of the study; the researcher maintained the anonymity/confidentiality of the women.
The researcher introduced herself to every woman and briefly explained the nature, and the objectives of the study before participation. Participant women were enrolled voluntarily after the oral informed consent.
3.7. Pilot Study
The pilot study was carried out on 10percentage of the studied women in the study setting (that were excluded from)
3.8. Field Work
Data were gathered over six months beginning in November 2021 and ending in April 2022.
3.9. Statistical Analysis
All data were collected, tabulated and statistically analyzed using IBM SPSS 25. Data was supplied, and appropriate analysis was performed for each parameter based on the type of data obtained.
3.9.1. Descriptive Statistics data were expressed as:
3.9.2. Analytical Statistics:
3.9.3. Graphical presentation:
Table (1) showed that the mean age of the studied participants was 22.6±5, most of them were rural residents (70.4percentage), 90.2percentage were highly educated, 57.5percentage were single, 96.8percentage were Muslims, and most of their mothers were educated (72.8percentage), and most of their fathers were educated (83.2percentage). About two-thirds of the participants were a student (65.4percentage).
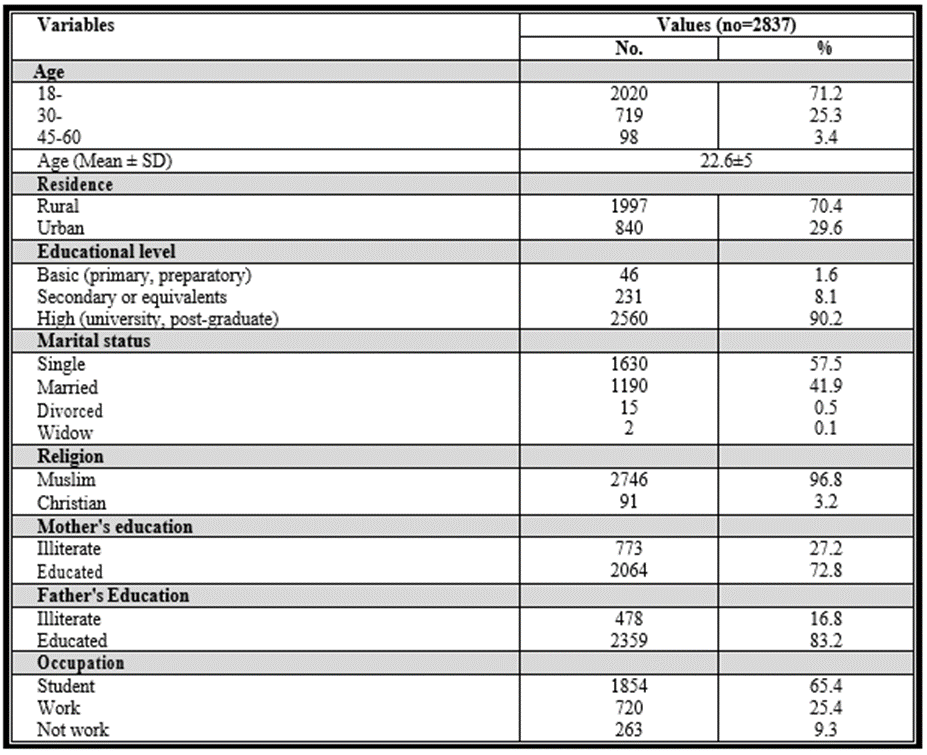
Table (1): Socio-Demographic Characteristics & of the Studied Participants.
Figure (1) presents that the prevalence of Female Genital Mutilation (FGM/C) among total participants (2837) at Beni-Suef is 71.4percentage.

Figure (1): Prevalence of female genital mutilation/cutting.
Figure (2) Presents participants' intention to perform FGM for their sister or daughter. About 28.6percentage of females who had mutilated their daughters were planning to mutilate their other daughters in the future.
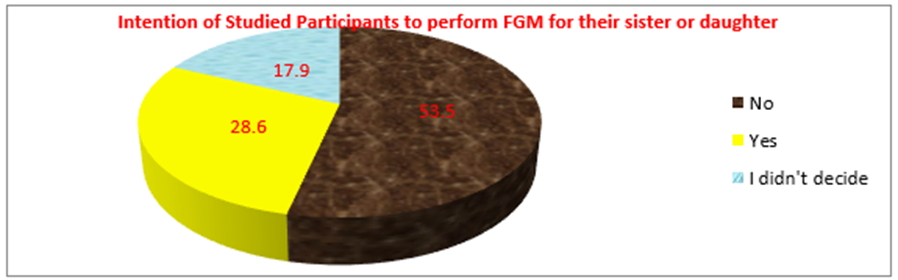
Figure (2): Participants' Intention to perform FGM for their sister or daughter.
Table (2) showed Significant statistical relationship between participants' intention of mutilating their daughters and demographic & personal characteristics (plessthan0.001).
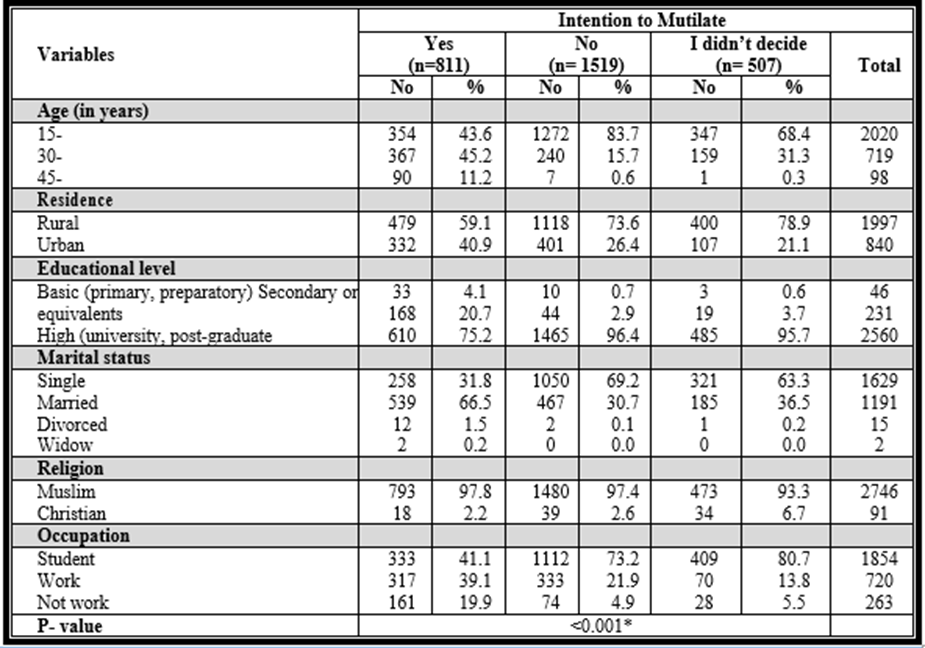
Table (2): Relationship between Females' Intention of Mutilating their daughters and Demographic & Personal Characteristics
*P-value is significant (plessthan0.001)
Table (3) presents the distribution of sample according to their total knowledge score. Only 25.7percentage of females had good knowledge regarding FGM/C, while 40.5percentage and 33.8percentage had poor and fair levels of knowledge.

Table (3): Total Knowledge Scores among the Studied Participants.
Table (4) describes the percent of the distribution of females according to their total attitude score towards FGM/C. More than one-third of females (35.5percentage) had an unfavorable attitude towards (supporting) FGM/C and 44.3 percentage of them had a favorable attitude towards (refusing) FGM/C while 20. 2percentage had a neutral attitude.

Table (4): Attitude categories among the studied participants.
Table (5) presents significant statistical relationship between females' intention of mutilating their daughters and their mutilation experience, level of knowledge, and level of attitude (plessthan0.001).
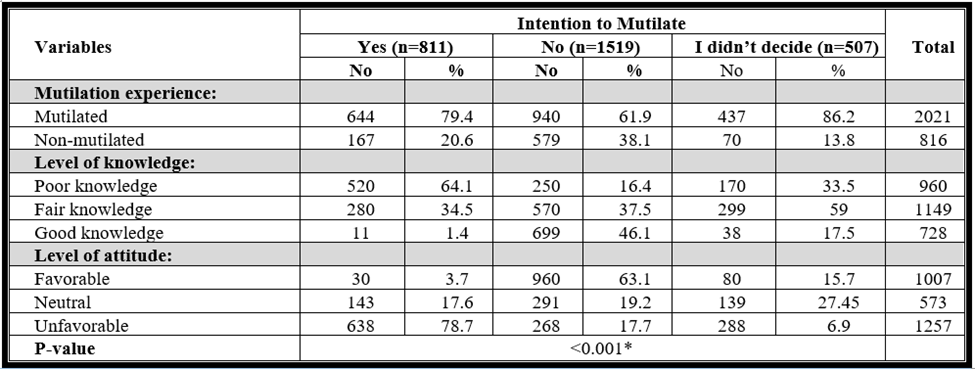
Table (5): Relationship between Females' Intention of Mutilating their daughters and their Mutilation Experience, Level of Knowledge, and Level of Attitude
*P-value is significant (plessthan0.001)
Figure (3) portrays the distribution of females according to their source of information regarding FGM/C. About 71.3percentage of females mentioned that the source of their information about FGM/C was their personal experience, 36.2percentage from friends or neighbors, and 22percentage from TV or radio.
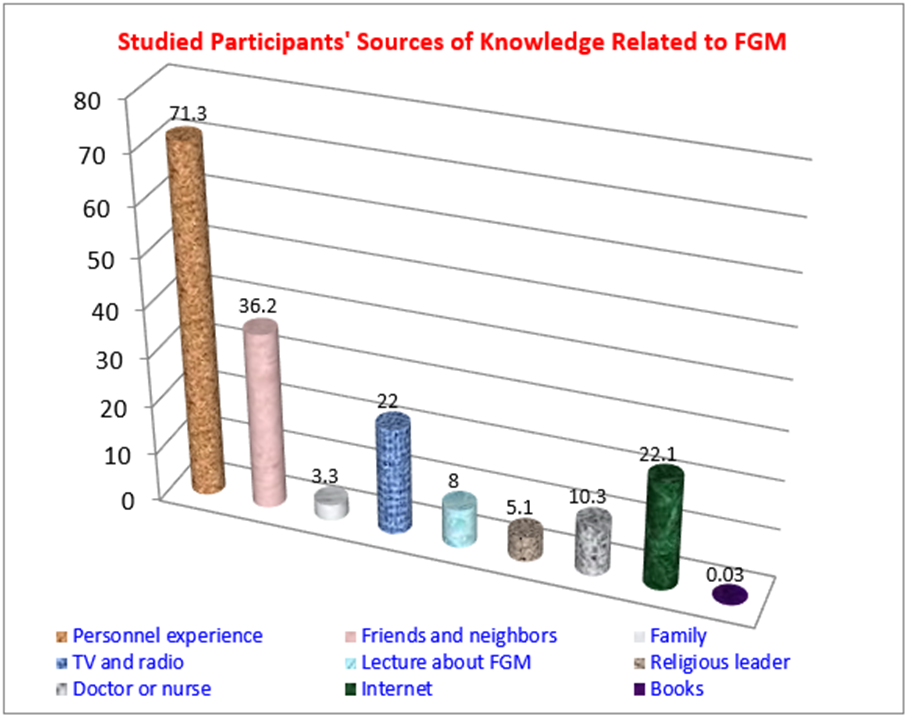
Figure (3): Sources of information regarding FGM among the Studied Participants.
Table (6) shows a significant statistical relationship between women's intention to circumcise their daughters and their source information (plessthan0.001).
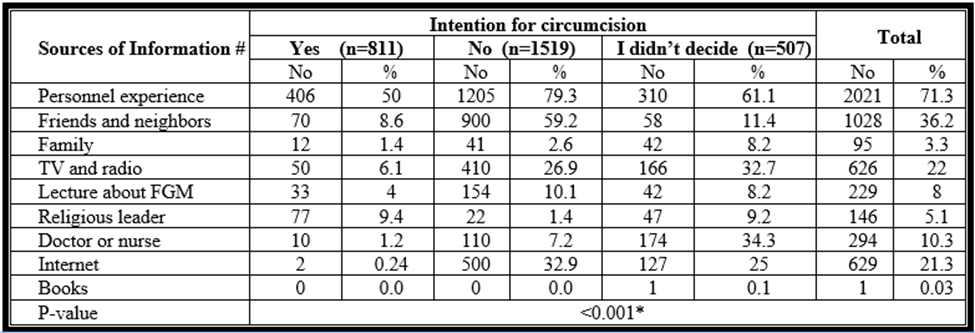
Table (6): Relationship between Source of Information and their Intention to Mutilate their daughters.
*P-value is significant (plessthan0.001) (# more than one answer).
Table (7) reveals that about 29.7percentage of participants are suffering from complications after FGM. About 82.1percentage of them suffered from pain after the surgery. About 79.9percentage of females were facing pressure from a family member to perform FGM/C, and 5.9percentage were facing pressure from a neighbor.
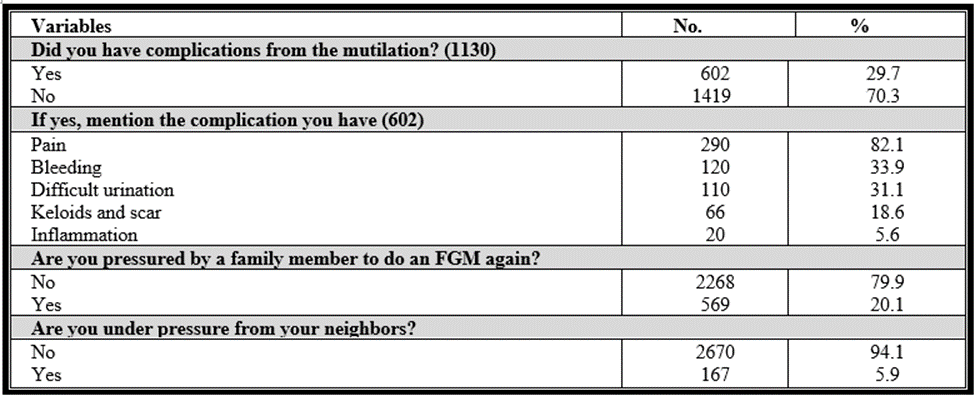
Table (7): Females' exposure to Pressure, and Complication.
Table (8) showed statistically significant relationship between women's intention for mutilation and their exposure to complications or pressure from family and neighbors (plessthan0.001).
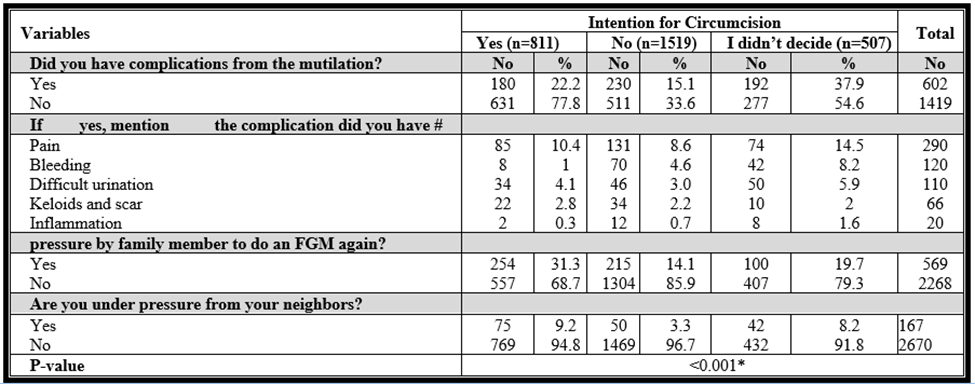
Table (8): Relationship between Women's Intention for Mutilation, Exposed to Pressure, And Complication.
*P-value is significant (plessthan0.001) (# more than one answer).
Figure (4) shows the distribution of females according to their reasons for performing and reasons for refusing FGM/C. Traditions and culture was the main reason for performing FGM/C as stated by females (77.4percentage), followed by religious requirements 21.7 percentage, decrease the sexual desire of females (14.4percentage). Health consequences of FGM/C were the main reason stated by females for refusing the procedure (47.3percentage), followed by 10.3percentage of females who stated that FGM/C is not necessary.
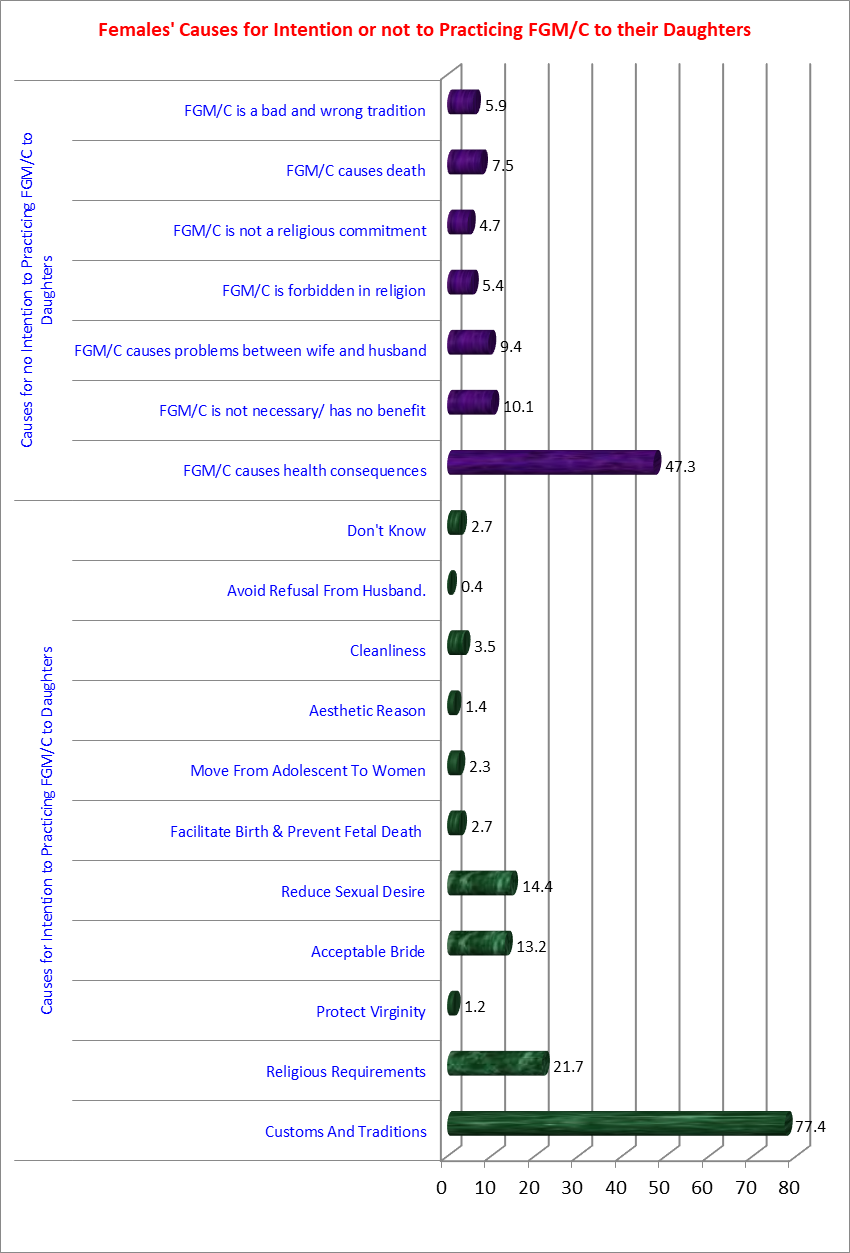
Figure (4): Distribution of Females According to their Causes for Intention or not to Practicing FGM/C.
According to the 2015 Egypt Health Issue Survey (EHIS), the prevalence of FGM/C among females aged 15-19 years was 70percentage, while 80percentage of females aged 20 - 24 had endured FGM/C compared to 89percentage-97percentage of females aged 25-49 who were mutilated. Quite half of the girls aged 1 -14 are probable to experience FGM/C in the future. The prevalence of FGM/C is lower among non-married females compared to ever-married females (68percentage and 93percentage, respectively) [30].
Regarding prevalence of FGM, the presents study revealed that the prevalence of Female Genital Mutilation (FGM/C) at Beni-Suef is 71.4percentage. This result is in accordance with other studies in Upper Egypt that reported that the prevalence of FGC is ranging from 61percentage in Lower Egypt to 97percentage in Upper Egypt. It is practically common in Upper Egypt, with highs of 73.9percentage, 75.5percentage, and 85.5percentage in Beni-Suef, Assiut, and Luxor, respectively [31]. A study conducted among Suhag University students (2015) institute that the prevalence of FGM/C among female students was 86.87percentage [32].
Concerning females' intention in Upper Egypt to perform FGM for their sister or daughter; the results of the current study reveal that, near to one third of females aged 18-60 had the intention to mutilate their daughters. The EHIS statistics showed that two fifth intended to mutilate their daughters, which was higher than the results above [30]. The difference shows advancements in female attitudes, beliefs, and opinions regarding the ending of FGM/C in Egyptian society.
Significant relationships were found between women's intention to practice FGM/C and their level of education, and occupation (p-value lessthan0.001). The results of the present study revealed that their intention decreased with the increase in the level of education. This is close to a study conducted in Iran that revealed that intention decrease with an increased level of education [33]. Moreover, about two fifth of employed female has the intention to practice FGM, while the highest proportion of females who had no intention to practice FGM/C was among student females. This is at odds with a study conducted in UAE that revealed that employed and educated women were less likely to have undergone FGM/C. highlighting the crucial role that women's education plays in efforts to end FGM/C [34].
Female genital mutilation/cutting is seen as a normal part of female socialization in societies that practice it [35]. Regarding statistical relationship between females' intention of mutilating their daughters and their mutilation experience, level of knowledge, and level of attitude, significant statistical relationship was found. About 79.4percentage of females who experienced FGM/C had the intention to mutilate their daughters in the future. This result agrees with a study conducted in Ethiopia, which revealed that the circumcised respondents were nearly three times more likely to intend the continuation of FGM than uncircumcised respondents [36].
Females' intentions to continue performing FGM/C on their daughters were significantly predicted by their prior experience with mutilation, lack of knowledge, an unfavorable attitude, rural residence, and pressure from their families. This was in line with a study conducted in Egypt, which discovered that the desire of females to continue performing FGM/C on their daughters was significantly predicted by the experience of mutilation, lack of education, an unfavorable attitude, and pressure from the spouse [11,37]. In Ethiopia, lack of access to mass media, degree of education, and age all had an impact on women's intentions to undergo FGM or C [38].
The primary sources of information for study's sample regarding FGM were personal experience, friends or neighbors. This is contradicted [39] who conducted research in rural Egypt, found results that contrasted with the findings of the current study because their participants' primary sources of information were radio and television. A significant statistical relationship between women's intention to circumcise their daughters and their source information was found. This highlights the idea that media had an impact on participants' awareness and may be used in delivering the eradication messages required to stop FGM/C practices in Egypt.
A proportional slid of participants are suffering from complications after FGM. They suffered from pain after the surgery, severe bleeding, difficult micturition and keloid and scar from the mutilation. There was an association between women's intention for mutilation and type of complication they have exposed. This expected as bleeding is life threaten. Shabila, et al., (2019) reported that hemorrhage occurs when the arterial blood supply to the genital organs is severed. The hemorrhage can happen right after the procedure or later as a result of a clot sloughing over the blood supply due to the infection [40]. Berg, R. C, 2018 added that severe bleeding after an FGM/C operation can result in a decrease in the volume of circulating blood in the body, leading to hemorrhagic shock. If the female does not receive the emergency help, she requires, she may die soon [41].
Females who were intended to mutilate their daughters in the current study were facing pressure from a family member to perform FGM/C, from their own family or their husband’s family, and neighbors. There was an association between women's intention for mutilation and they're exposed to pressure from family as found by results of the current study. In the present study, about one fifth of females were facing pressure from a family member to perform FGM/C, from their own family or their husband's family, and the minority was facing pressure from a neighbor. One of the main causes of the intention to mutilate daughters was family pressure, according to research done in Upper Egypt to assess how women felt about the prohibition on FGM/C [42,43].
Northern Upper Egyptian Females' Intention regarding intention of mutilating their daughters was significantly affected by demographic characteristics, level of knowledge, and level of attitude, source information, exposure to complications or pressure from family and neighbors
Conflict of interest: The authors have no conflicts of interest to disclose.
Source of funding: The authors did not receive funding for this work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
