
Research Article | DOI: https://doi.org/10.31579/2578-8868/326
1Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
2Federal State budgetary Educational Institution of Higher Education «St. Petersburg State Pediatric Medical University», 194100, Litovskaya st., 2, Saint-Petersburg, Russia.
3Almazov National Medical Research Centre, 197341, Accuratova st., 2, Saint-Petersburg, Russia.4The North-Western State Medical University named after I.I. Mechnikov, 191015, Kirochnaia st., 41, Saint-Petersburg, Russia.
*Corresponding Author: Darya Sitovskaya, Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
Citation: Sitovskaya D.A., Naumova A.D., Sokolova T.V., Krapivin M.I., and Dinikina Yu.V, et al, (2024), Features of Vascular Endothelial Growth Factor А (Vegf-А) Expression in Atypical Teratoid-Rhabdoid Tumor of the Central Nervous System in Children, J. Neuroscience and Neurological Surgery, 15(5); DOI:10.31579/2578-8868/326
Copyright: ©, 2024, Darya Sitovskaya. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 20 June 2024 | Accepted: 08 July 2024 | Published: 22 July 2024
Keywords: atypical teratoid/rhabdoid tumor; AT/RT; VEGF; children; tumors of the central nervous system
Atypical teratoid rhabdoid tumors (AT/RT) are highly malignant neoplasms composed of poorly differentiated germline cells and a variable number of rhabdoid cells that can differentiate into different cell types. A key diagnostic factor for AT/RT is the absence of nuclear expression of the INI1 protein (SMARCB1 gene product) when tested with an anti-INI1 antibody in an immunohistochemical study. Currently, there is no standard treatment for AT/RT, but treatment approaches have become more aggressive and multimodal. In one study, AT/RT was found to be positive for VEGF. The purpose of our study was to examine the expression of VEGF-A in AT/RT in the central nervous system of children. We analyzed biopsy samples from 6 male patients aged 3 months to 8 years (average age 4.5 years). The level of VEGF-A expression was measured by counting the number of brown pixels in the cytoplasm of tumor cells using the PhotoM program in 1 mm2 of tumor tissue. Immunohistochemistry (IHC) revealed varying levels of cytoplasmic staining with an antibody to VEGF-A in 5 out of 6 patients, with the youngest patient (No. 6) showing staining only in endothelial cells. In conclusion, children with AT/RT exhibit different patterns of VEGF-A expression, potentially dependent on the molecular subgroup. Identifying this marker in these highly aggressive tumors could aid in developing new treatment protocols and determining which patients would benefit most from treatment.
Atypical teratoid rhabdoid tumors (AT/RT) are highly malignant neoplasms composed of poorly differentiated germline cells and a variable number of rhabdoid cells. These tumors have the potential to differentiate along neuroepithelial, epithelial, and mesenchymal lineages. AT/RTs can occur throughout the nervous system, with supratentorial tumors being more common in older adults and infratentorial tumors being more prevalent in children. Localization in the spinal cord is rare [1]. While AT/RTs account for only 1-2% of all central nervous system (CNS) tumors in children, they are relatively common in early childhood, accounting for up to 20% of all malignant CNS tumors in children under 3 years of age [2]. The average age of diagnosis is 16-30 months, with a consistent male predominance. Due to the primitive state of the tumor cells and their multilineage differentiation, the histological and immunohistochemical features of AT/RTs can vary greatly. Cell nests often show positivity for synaptophysin, glial fibrillary acidic protein (GFAP), cytokeratins, epithelial membrane antigen (EMA), and smooth muscle actin (SMA) [3]. A significant diagnostic criterion is the absence of nuclear expression of the INI1 protein with anti-INI1 antibody in the case of AT/RTs, while maintaining internal control. This is observed as a result of mutations in the SMARCB1 gene. A small portion of AT/RTs may retain SMARCB1/INI1 expression but may also contain mutations in SMARCA4 [4]. Currently, there is no standard treatment for AT/RTs [5, 6]. Treatment strategies have evolved towards an aggressive multimodal approach, with an overall trend towards improved outcomes. However, the relative contribution of each method (surgery, high-dose chemotherapy, intrathecal chemotherapy, radiation therapy) is still unclear and may depend on the unique biology of the tumor [4].
A hypoxic environment is known to induce the differentiation of cancer stem cells (CSCs) towards endothelial progenitor cells and mature endothelium, which in turn form new blood vessels within the tumor. Tumors generate abnormal and functionally immature blood vessels due to dysregulated factors in the process of pathological angiogenesis. The progression of a brain tumor is closely related to the formation of new blood vessels. Brain tumor angiogenesis is mediated by the action of many angiogenic factors, including VEGF, basic fibroblast growth factor (bFGF), hepatocyte growth factor (HGF), platelet-derived growth factor (PDGF), angiopoietins (Angs), and others [7]. Vascular endothelial growth factor (VEGF, OMIM 192240) is a heparin-binding growth factor specific for vascular endothelial cells that is capable of inducing angiogenesis in vivo. It is the only mitogen that specifically acts on endothelial cells, but it also affects neurogenesis [8]. VEGF has six isoforms (VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, and placental growth factor) [7]. In the nervous system, VEGF-A directly regulates neuronal migration and axon guidance independent of its role in blood vessels. Additionally, VEGF-A has been proposed to play multiple pleiotropic roles in pathological conditions of the central nervous system, such as malignancies and neurodegeneration. VEGF-A also has new functions that act inside the cell, resulting in its expression in an intracrine manner. Intracellularly localized VEGF becomes an important signaling molecule regulating cell growth, survival, and metabolism [9]. A single study showed that VEGF immunopositivity was observed in 83.3% of cases [10]. Therefore, VEGF expression can serve as a prognostic biomarker and be used to determine treatment regimens for atypical teratoid-rhabdoid tumor of the central nervous system in children.
Purpose of the study
To study the features of VEGF-A expression in atypical teratoid-rhabdoid tumor of the central nervous system in children.
Biopsy samples were obtained from brain fragments of 6 male patients with atypical teratoid rhabdoid tumor, ranging in age from 3 months to 8 years with an average age of 4.5 years, from Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre. The samples were collected intraoperatively and fixed in 10% buffered formalin. Standard dehydration and paraffin embedding techniques were used. Histological sections were stained with hematoxylin and eosin, and immunohistochemical (IHC) reactions were performed using antibodies to VEGF-A, as well as diagnostic markers GFAP, SMA, EMA, synaptophysin, and INI1 (antibodies from Dako (USA), EnVision imaging system). Fluorescent in situ hybridization (FISH) was also performed using probes for the MYC and SMARCB1 genes. Histological analysis and microphotography were conducted using a Leica Aperio AT2 scanning microscope and AperioImageScope image manager (Leica Microsystems, USA). The results of the reaction with antibodies to VEGF-A were evaluated by counting the number of pixels of the required color (according to the color passport) in the cytoplasm of tumor cells using PhotoM programs (Russia) and further processed using software in the Python programming language. Endothelial cells stained with anti-VEGF-A antibody were excluded from the study. Statistical analysis was not performed due to the small number of patients. The study was conducted in accordance with the Helsinki Declaration of Human Rights, and all patients (or their representatives) provided informed voluntary consent to participate. Preoperative examinations and surgical treatments were carried out in accordance with the Clinical Guidelines of the Association of Neurosurgeons of Russia 2015.
The histological examination of the resected tumors (Fig. 1a-d) revealed a highly malignant, diffusely growing hypercellular tumor with pronounced cellular-nuclear polymorphism. The main pool of cells consisted of clusters of large cells with abundant eosinophilic and light cytoplasm and an eccentrically located round nucleus. The nuclei showed vesicular chromatin and large basophilic nucleoli. Foci of small, monomorphic, embryonic-like cells were also identified, with scant eosinophilic cytoplasm and hyperchromic round nuclei with granular chromatin. In one patient, the embryonic component of the tumor was predominant. The intercellular matrix was scanty, and the tumor stroma was vascularized with thin-walled capillary-type vessels. Foci of ischemic necrosis, high mitotic activity (up to 3 mitoses in 1 field of view at ×400 magnification), and apoptotic bodies were detected. Immunohistochemical examination revealed loss of staining with the INI1 marker in the nuclei of all tumor cells (Fig. 1c). Additionally, deletion of the SMARCB1 gene was detected in two cases (Fig. 1d).
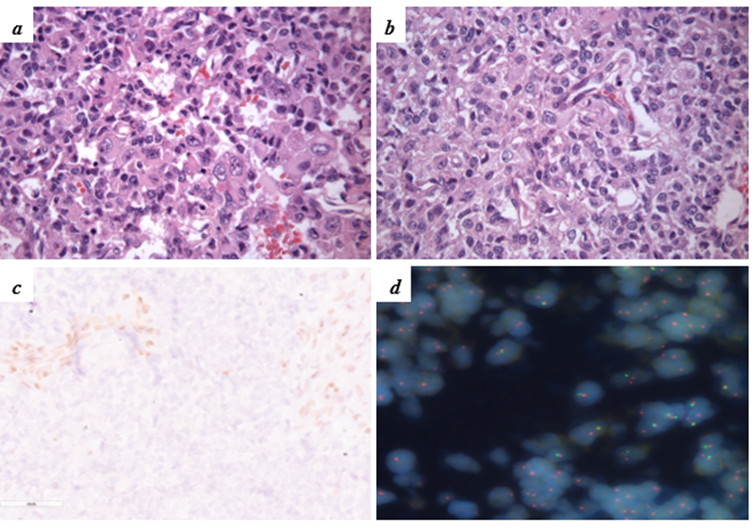
Figure 1. Histological features of AT/RT and results of diagnostic studies.
a-b – diffuse tumor consisting of large cells with abundant eosinophilic cytoplasm and an eccentrically located round nucleus with vesicular chromatin and large basophilic nucleoli. H&E stain, ×400
c – immunohistochemical reaction with antibody to INI1: loss of staining in the nuclei of tumor cells, staining is preserved in the nuclei of the vascular endothelium, ×400.
d – FISH results with a probe to the SMARCB1 gene. Signals to the KREMEN1 (reference) gene are indicated in red, signals to the SMARCB1 gene are indicated in green. Most cells do not carry a single copy of the SMARCB1 gene, ×630.
In addition, the tumor cells exhibited varying levels of staining with antibodies to synaptophysin (Figure. 2a), EMA (Figure. 2b), GFAP (Figure. 2c), SMA (Figure. 2d), and high molecular weight cytokeratins AE1/AE3. The proliferative activity, as indicated by Ki67 staining, was high with an average of 15-20% and reaching up to 30% in "hot" lesions (Figure. 2e).
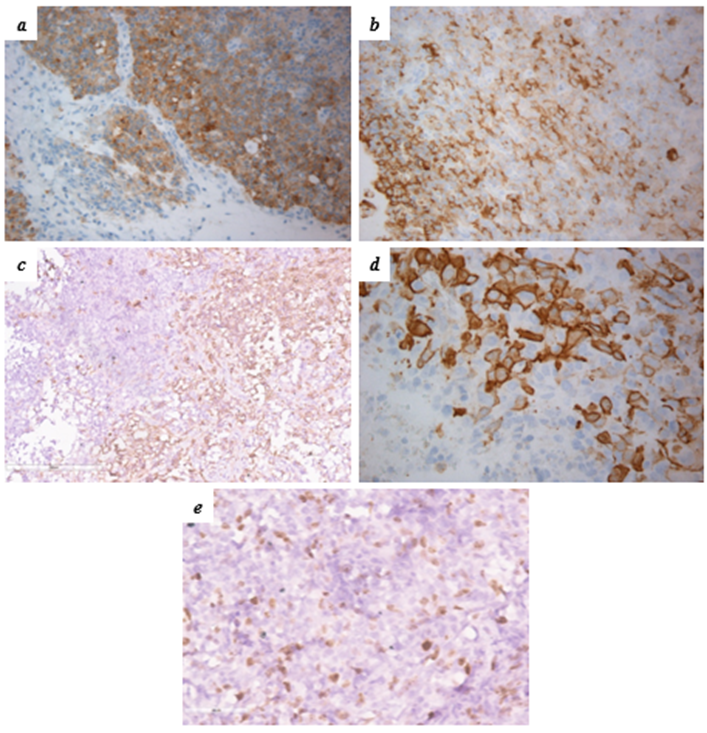
Figure 2. Results of immunohistochemical reactions in the studied tumors.
a – IHC with antibodies to synaptophysin, ×200
b – IHC with antibodies to EMA, ×200
c – IHC with antibodies to GFAP, ×200
d – IHC with antibodies to SMA, ×400
e – The level of proliferative activity for Ki67 was 15-20%, in “hot” foci up to 30%, ×400
An immunohistochemical study using an antibody to VEGF-A (Figure. 3) showed cytoplasmic staining of varying severity in 5 out of 6 (83.3%) patients, ranging from dot-like to focal-diffuse. In patient No. 6 (the youngest in the study group, 3 months old), staining was only observed in endothelial cells.
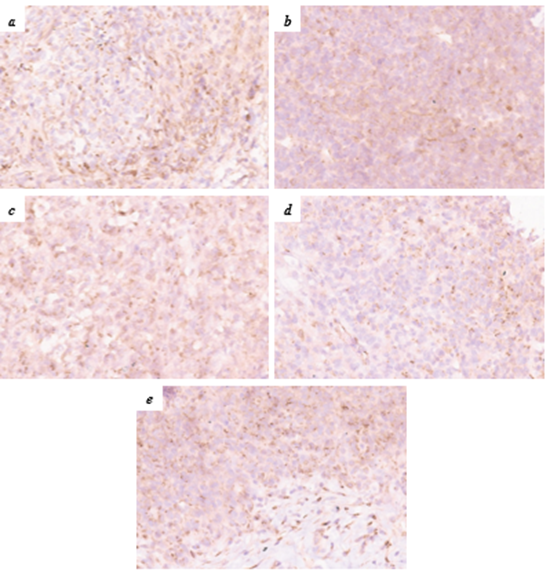
Figure 3. Expression of VEGF-A in AT/RT in children (description in text).
Immunohistochemical reaction, ×400 a-e – patients No. 1-5.
The level of VEGF-A expression, calculated by the number of pixels with a positive reaction in the cytoplasm of cells (symbol units, s.u.) per 1 mm2 of tumor tissue, ranged from 0.014 to 0.454 s.u. (μ = 0.173±0.09). The highest values (0.12-0.45 s.u., μ = 0.29±0.13) were found in a patient with a dominant embryonic component in the histological examination. In patients with a homozygous (biallelic) deletion of the SMARCB1 gene (22q11), the level of VEGF-A expression was relatively low, ranging from 0.115 to 0.283 s.u. (μ = 0.19±0.06) and 0.014 to 0.199 s.u. (μn = 0.07±0.06), respectively (Table 1).
| Patient | Gender | Age | VEGF-A expression level, s.u. | Mean (μ) ± standard deviation | SMARCB1 gene deletion | MYC gene amplification | |
| From | To | ||||||
| 1 – D. | male | 4,8 | 0,082 | 0,126 | 0,11 ± 0,02 | – | – |
| 2 – S. | male | 7,2 | 0,12 | 0,45 | 0,29 ± 0,13 | – | – |
| 3 – K. | male | 8,1 | 0,12 | 0,28 | 0,19 ± 0,06 | + | – |
| 4 – N. | male | 4,9 | 0,13 | 0,32 | 0,2 ± 0,08 | – | – |
| 5 – A. | male | 1,7 | 0,01 | 0,2 | 0,07 ± 0,06 | + | – |
| 6 – K. | male | 0,3 | 0 | 0 | 0 | – | – |
Table 1. Patients Information, VEGF-A Expression Morphometry Results, and Molecular Genetic Research Findings
Currently, three molecular subtypes of AT/RT have been identified based on gene expression profiles associated with gender and tumor location. These subtypes, AT/RT-MYC, AT/RT-SHH, and AT/RT-TYR, may have prognostic and therapeutic significance [4, 11]. The AT/RT-TYR subgroup is named after the tyrosinase enzyme, which is overexpressed in most AT/RT-TYR cases but not in other AT/RT subgroups or other brain tumors [11]. This enzyme plays a crucial role in the development of the neural tube by catalyzing the synthesis of melanin in melanocytes. The genetically prototypical type of biallelic inactivation of SMARCB1 in the AT/RT-TYR group is the complete or partial loss of one copy of chromosome 22, accompanied by an inactivating mutation in the other allele of SMARCB1. Clinically, patients in this subgroup are typically the youngest, with a median age at diagnosis of 12 months (range 0–108 months) [1]. This subgroup also has the highest proportion of patients under 3 years of age at diagnosis. The AT/RT-SHH subgroup shows overexpression of both sonic hedgehog (SHH) pathway elements and Notch pathway elements, such as GLI2, PTCH1, and BOC or ASCL1, HES1, DTX1 [12]. All SHH pathway marker genes overexpressed in this subset (such as GLI2) are likely to be activated directly or indirectly by loss of SMARCB1 in these tumors. The AT/RT-MYC subgroup is named based on increased expression of the MYC oncogene (it should be noted that the MYCN oncogene is upregulated in the AT/RT-SHH group). The typical genetic pattern that leads to SMARCB1 inactivation in this group of tumors is homozygous extensive loss of SMARCB1. The mean age of patients with AT/RT-MYC is significantly higher than in the other two subgroups [11]. In our study, due to limitations of the method, it was not possible to determine the exact molecular subgroup. However, in patients who, according to clinical and morphological data, most likely belong to the AT/RT-MYC group, lower levels of VEGF-A expression were noted. It should be noted that due to the small sample size, a conclusion cannot be made. Our study also found that the only infant (3 months) had no expression of VEGF-A. These results raise the question for researchers about the need for routine determination of VEGF-A levels in CNS AT/RT, stratification of expression levels, and potential for chemotherapy.
Children with AT/RT have varying patterns of VEGF-A expression within the tumor structure, potentially influenced by the molecular subgroup. The identification of this marker in these highly aggressive tumors could have significant implications for the development of new therapeutic protocols and for determining which patients would benefit most from treatment.
The authors declare no conflict of interest.
The study was performed without external funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
