
Research Article | DOI: https://doi.org/10.31579/2639-4162/016
*Corresponding Author: Grimar de Oliveira Paula, Study undertaken in the Department of Cytopathology and Anatomical Pathology and Urology of the Federal District Base Institute (NUCAP-IHBDF), Brasília, Brazil.
Citation: Grimar de Oliveira Paula, João Emerson de Alencar Santos, Luiz Carlos de Araújo Souza. Analysis of the Prevalence and Factors Related to Biochemical Relapse in Patients Undergoing Radical Prostatectomy with Lymphadenectomy J. General Medicine and Clinical Practice . DOI: 10.31579/2639-4162/016
Copyright: © 2019 Grimar de Oliveira Paula. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 February 2019 | Accepted: 15 March 2019 | Published: 23 March 2019
Keywords: Prostate Specific Antigen ; Biochemical Recurrence ; Prostate Cancer
Objectives - Analyze the prevalence of biochemical recurrence (BCR) in patients submitted to radical prostatectomy with lymphadenectomy (RP-LD) the most prevalent clinical and pathological staging in the BCR and to correlate the sum of the Gleason score (GS) in the surgical specimen in patients who presented BCR. Method - Analysis of 100 patients diagnosed with prostate adenocarcinoma who performed RP-LD between 2013 to 2017. All subjects underwent transrectal prostate biopsy due to PSA or rectal examination and RP-LD. The lymphadenectomy considered in the study was the iliac-obturator, and the surgical pieces were analyzed to determine the pathological staging and its descriptors. All patients who had two or more PSA measurements >0.2 ng/ml and who had undergone RP-LD were considered postoperative. Results -About 22% of the patients submitted to RP-LD presented BCR. Patients with BCR had a 59-76 age range, mean age of 66.27 years, and median age of 63.50 years. The most prevalent preoperative PSA in patients with BCR was between 10-20 ng/ml (40.90%) and the most prevalent clinical stage was cT2 (59.10%). Regarding the Gleason score, the BCR patients had the most prevalent 6 (36.37%) score in the biopsy and score 7 (4 + 3) (36.37%) in the surgical specimen. All patients (100%) with BCR presented perineural invasion, with pT3 staging (81.81%) and pN0 (77.28%) being the most prevalent in patients with BCR. Patients with BCR presented a correlation (p<0.05) between the increase in the sum of pathological GS and the increase in pTN staging. Conclusion - All these variables were important in the determination of BCR in patients submitted to RP-LD, thus demonstrating the importance of this information in the analysis of the prognosis and in the follow-up of these patients.
Epidemiological studies have shown that in Western countries prostate cancer (PCa) is the most frequently diagnosed malignant neoplasm and the second leading cause of cancer-related death in males. Radical prostatectomy (RP) is the standard surgical treatment and among patients undergoing this treatment there is a survival benefit, especially in cases where the disease is localized1,2.
Biochemical recurrence (BCR) after surgical treatment of PCa is a possible event. Studies have shown that about 25% of men who underwent RP will have PCa BCR, and 34% of patients with BCR will develop metastatic disease3,4,5.
The BCR is directly associated with the presence of positive surgical margins, and the oncological prognosis is impaired in cases where the margins impairment is detected. According to Swindle et al. the positive surgical margin is the only factor that can be influenced by surgery in the oncological prognosis after performing the RP and the incidence ranges from 6 to 41%11,12,13.
Serum prostate-specific antigen (PSA) is the most sensitive indicator of BCR after definitive local therapy for PCa. All patients who develop clinical relapse, local or distant, will have detectable serum levels of PSA3. There are several definitions of relapse after RP. The most used and accepted method consists of two measures of PSA >0.2 ng/ml6,14.
Tumor pathological staging, Gleason score (GS), seminal vesicle invasion, lymphatic invasion and surgical margins were considered as factors to predict the subsequent risk of BCR after RP7,8,9,10. In this sense, our study evaluated the most prevalent clinical and pathological staging in patients with BCR, the compromised surgical margins and the correlation of the Gleason score of the biopsy and the surgical specimen.
Materials and Methods
Descriptors of the analyzed patients
We analyzed 100 patients diagnosed with adenocarcinoma of the prostate who underwent RP-LD between 2013 to 2017. After the selection of these patients, we collected information through electronic medical records and anatomopathological reports retrospectively. All patients enrolled in the study underwent transrectal prostate biopsy because of changes in PSA or rectal examination. The image of the prostate was obtained by transrectal ultrasound, which also guided the collection of the fragments for histopathological analysis by puncture, sextant using a 18-gauge needle. After determination of the Gleason biopsy and surgical indications for RP-LD, patients were surgically treated for curative purposes. The lymphadenectomy performed in the study was iliac-obturator. After surgery, the surgical specimens were analyzed by anatomopathological study to determine: pathological gleason; measurements of prostate length (cm); prostate volume; angiovascular/perineural invasions; invasions of the seminal vesicles; surgical margins (bladder and urethral); pathological staging pTNM. The criteria considered for BCR were all those patients submitted to LD-PR who presented two or more PSA measurements with values above 0.2 ng/ml in post-surgical follow-up.
Approval at the Research Ethics
The present study was approved by the Research Ethics Committee of the Base Institute of the Federal District, Brasília, CAAE: 93792918.8.0000.8153.
Statistical analysis
The descriptors collected retrospectively were grouped in Excel table for grouping and analysis of the variables and the variables analyzed were computed using SPSS 20.0. Variables such as clinical and pathological staging, surgical margins and the sum of the pathological Gleason were considered statistically significant for the correlation of the variables using the Pearson correlation (p <0.05).
After analysis of clinical and pathological characteristics (Table 1), it was found that 22% of the patients submitted to RP-LD presented BCR. Patients with BCR had a 59-76 age range, mean age of 66.27 years, and median age of 63.50 years. The most prevalent preoperative PSA (ng/ml) of patients without BCR were <10 ng/ml (52.26%) and in patients with BCR were between 10-20 ng/ml (40.90%). The most prevalent clinical staging of both non-BCR and BCR patients was cT2 with prevalence of (51.28%) and (59.10%) respectively.
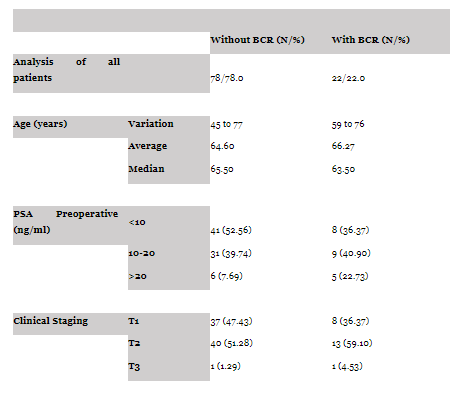
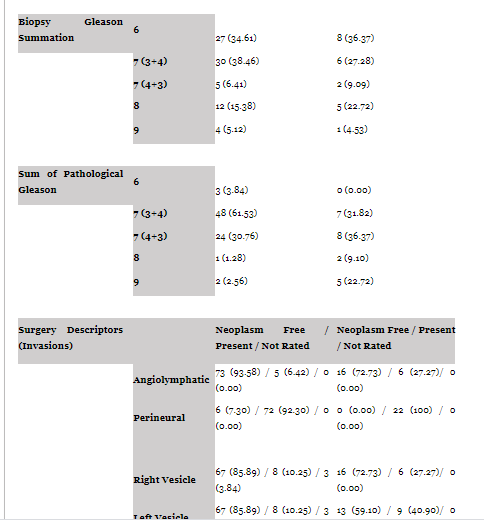

Table 1. General data of the analyzed patients
When the values of the GS of the biopsy and the surgical specimen were added together, we showed that the patients with no BCR obtained the 7 (3 + 4) (38.46%) most prevalent sum in both the biopsy and the surgical specimen (61.53% ), but Gleason 6 (3 + 3) (36.37%) was more prevalent in the biopsy and Gleason 7 (4 + 3) (36.37%) in the surgical specimen.
The anatomic-pathological description of BCR patients showed that the majority (72.73%) were free of angiolymphatic neoplasia and 100% of them had perineural invasion; 72.73% had neoplasia-free right gallbladder; 59.10% had neoplasia-free left vesicle; 68.18% had positive extraprostatic extension; 86.36% had a neoplastic-free bladder surgical margin and 63.64% had a neoplastic-free urethral surgical margin. When analyzing the pathological staging of the surgical specimen, we found that pT3 staging (81.81%) and pN0 (77.28%) are the most prevalent in patients with BCR.
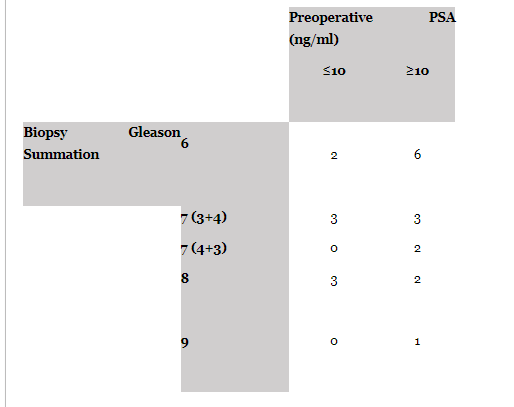
When analyzing the preoperative PSA and GS values of the biopsy in patients with BCR (Table 2), two (9.10%) patients presented preoperative PSA ≤ 10 ng/ml and GS 6 and eight (36.37%) patients presented preoperative PSA ≥10 ng/ml and GS≥7.
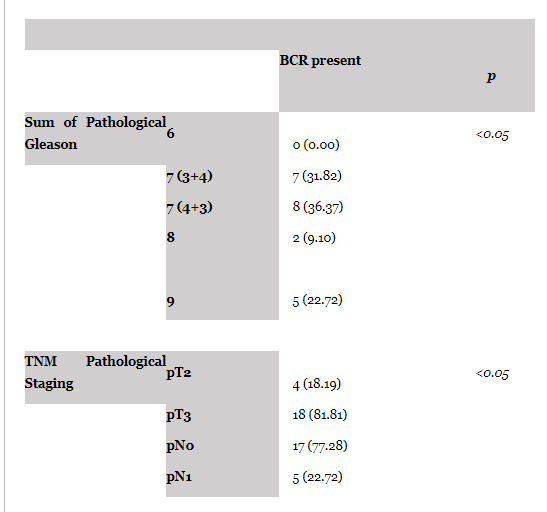
When analyzing the correlation of the multiple variables influenced in all the patients, it was evidenced that the patients with BCR had a correlation (p<0.05) with the increase of the sum of the pathological GS and with the increase of the pTN staging (Table 3). Thus demonstrating the importance of these variables in the prognosis of these patients analyzed.
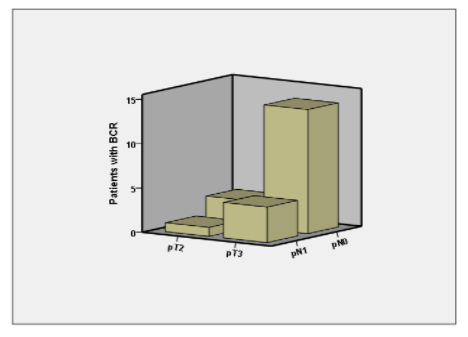
In a cross-analysis of patients with BCR and their pathological stages (Graphic 1), 14 (63.64%) patients had staging (pT3N0) and 4 (18.19%) had staging (pT3N1), 3 (13.64%) had staging (pT2N0) and 1 (4.53%) had staging (pT2N0). These correlated variables did not reach a p<0.05 and, therefore, were not significant.
Discussion
Approximately 20-40% of men undergoing RP will present BCR within 10 years after treatment. It is suggested that there is a relationship between PSA doubling time and the biological behavior of adenocarcinoma of the prostate14. When analyzing 100 patients with prostatic adenocarcinoma who underwent RP, the prevalence of BCR in the study was 22%.
The value of preoperative PSA levels was considered an important predictor in the determination of pathological findings and the best clinical predictor in the determination of BCR after RP15. The combination of clinical PSA and GS biopsy descriptors identified the risk stratification for BCR, with patients with preoperative PSA ≤10 ng/ml and GS ≤6 presenting low risk for BCR and patients with preoperative PSA ≥10 ng/ml and GS ≥7 are at high risk for BCR and distant metastases15. Our study, when analyzing patients with BCR, showed that 14 (63.63%) patients had preoperative PSA ≥10 ng/ml and 14 (63.63%) patients had GS ≥ 7, so that 2 (9.10%) patients presented preoperative PSA ≤10 ng/ml and GS 6 and 8 (36.37%) had preoperative PSA ≥10 ng/ml and GS ≥7. Preoperative PSA prevalence of BCR patients were between 10-20 ng/ml (40.90%) (Table 1 and 2).
Several studies have considered GS as the most powerful predictor of BCR after RP, some studies have determined that the majority of men at risk for BCR after RP have Gleason disease 717,18. In the past, some studies have determined that the proportion of disease with GS pattern within 4/5 within PR specimens was predictive of both BCR and cancer-specific survival after RP19,20,21,22. In this respect, compelling evidence that the differentiation between Gleason 4 + 3 and 3 + 4 is a significant predictor of BCR after RP23. In this sense, studies have determined that a quantitative and more discriminative scoring system within the group of GS 7 patients may improve the ability to predict better and more appropriately which patients with Gleason 7 disease will present BCR17. Stratifying the GS of the biopsy in 3 + 4 and 4 + 3, it was verified that the patients with BCR obtained 6 (36.37%) more prevalent in the biopsy and 7 (4 + 3) (36.37%) in the part and that no patient with GS biopsy 7 (4 + 3) had preoperative PSA ≥10 ng/ml (Table 1 and 2). When correlating pathological GS and pTN staging, a significant correlation (p<0.05) between GS increase, increase in tumor invasion (pT) and lompa node involvement (pN) was observed (Table 3).
Prostate cancer may spread to the base of the gland along the ejaculatory ducts, penetrate the capsule through the perineural spaces, resulting in periprostatic growth, and may reach the seminal vesicles by direct capsule penetration24,25. Based on this, some studies have determiné that the independent predictors of BCR were biopsy GS, positive surgical margins and seminal vesicle invasion. The surgical approach was a significant predictor of BCR in the univariate analyzes, although its significance disappeared in the multivariate analysis26. In our analysis of BCR patients, perineural invasion was found in 100% of the cases, 27.27% in the right gallbladder and 40.90% in the left vesicle, 68.18% had extraprostatic extension, and 31.82% had urethral surgical margin (Table 1). The analysis of pathological staging of the surgical specimen showed that pT3 staging (81.81%) and pN0 (77.28%) were the most prevalent in patients with BCR.
Conclusion
PCa is one of the most prevalent neoplasms in the world and its treatment is still under study. PR remains one of the most common forms of treatment and some patients may develop BCR. In our study, perineural invasion was present in all cases that presented BCR and there was a significant correlation of the increase of pathological GS with the increase of pTN staging evidencing the importance of these descriptors in the evaluation of BCR in patients who performed PR.
Source of financing
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank the team of the Nucleus of Cytopathology and Anatomy-Pathology of the Institute of the Base Hospital of the Federal District (NUCAP-IHBDF) for the help and assistance during the elaboration of this work. Special thanks to the MASTER of Forensic Biosciences, Specialists in Human and Pathological Anatomy Dinaldo de Lima Leite and Hercules Marcelo Gomes for the support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
