
Review Article | DOI: https://doi.org/10.31579/2768-2757/076
Neurosurgery Service, Guemes Sanatorium, CABA, Argentina.
*Corresponding Author: Torres, Pilar, Neurosurgery Service, Guemes Sanatorium, CABA, Argentina.
Citation: Pilar T., Guido B., Martina A., Jeronimo M., Fedra S., Sebastian B., (2023), Factors Influencing the Degree of Resection and Proposed Preoperative Scale for the Management of Skull Base Meningiomas, Journal of Clinical Surgery and Research, 4(3); DOI:10.31579/2768-2757/076
Copyright: © 2023, Torres, Pilar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 May 2023 | Accepted: 18 May 2023 | Published: 26 May 2023
Keywords: meningioma; skull base; Simpson; scale; unicentric study; statistical analysis
Objectives: to identify factors involved in the degree of resection of skull base meningiomas and to propose a scale to calculate the probability of total resection.
Materials and methods: unicenter, observational, retrospective study of patients operated on in the period 06/2018 – 06/2022. The following variables were used: age, clinic, location, size, previous embolization, perilesional edema, intertumoral calcium, characteristics in T2 and T1 and bone invasion. The degree of resection was measured with the traditional Simpson classification and was also divided into total (Simpson I, II and III) and subtotal (Simpson IV and V) resection. With the results, a scale was proposed taking into account the variables with statistical significance (p < 0.05). A literature review of the topic was conducted.
Results: A total of 23 patients were operated. They were statistically significant associated with Simpson's grade, location (p 0.002) and size (p 0.001). Associated with total and subtotal resection, bone invasion (p 0.013). For the scale we use: location (anterior 1 point, posterior 2 points, medial 2 points and medial involving cavernous sinus 3 points), size (<5 cm 1 point, >5 cm 2 points) and bone invasion (not 1 point and if 2 points). We performed an inferential analysis and an association was observed between the scale performed and the degree of resection (p 0.005).
Conclusion: In our study, an association was observed between bone size, location and invasion with the degree of resection achieved. We proposed a scale to measure the probability of total resection.
Meningiomas are the most common primary CNS tumor. They originate from meningothelial cells found in the arachnoid layer of the meninges, may be associated with the dura mater or choroid plexus, and account for 36% of all CNS 1 tumors. They grow along the outer surface of the brain, spinal cord or, less commonly, within the ventricular system. There are 3 grades based on WHO criteria. 80% are grade [1], benign and slow growing; 20 - 25% are grade 2 with higher probability of recurrence; and 1-6% are grade 3, malignant with metastatic potential [2]. They occur at an average age of 65 years. 66% of cerebral meningiomas occur in women, rising to 90% when they are located in the spinal cord [3]. Cases may occasionally occur in the pediatric population, and are generally associated with genetic syndromes or infant radiation [4]. The base of the skull is a complex anatomical region that forms the floor of the cranial cavity. There are several neoplastic processes that can manifest in the skull base, with different distribution depending on their location is anterior, middle or posterior. Meningiomas can develop in any of their locations.Surgery is the first-line treatment for most benign and malignant skull base tumors [5]. Gross total resection is the therapeutic paradigm that is intended to be reached when we diagnose a meningioma. Based on tumor resection, its residual remnant and infiltrated dura mater, Simpson introduced in 1957 a prognostic classification for the extent of resection, which has been widely applied in neurosurgical practice [6]. Simpson Grades I, II, and III can be defined as gross total resection and were associated with lower recurrence compared to Grade IV and V, defined as subtotal resection [7,8]. The surgical challenge of this type of tumor, which as we have mentioned are usually benign lesions in its great majority, is due to the difficult accessibility given the anatomy and its proximity to critical neurovascular structures. To avoid Complications, it is often necessary to perform a subtotal resection and preserve the patient's functional status [9]. Therefore, presurgical planning and the establishment of the objectives of tumor resection are essential parts, and they must be individualized, to provide an adequate surgical result. It is very useful to identify predictive factors obtained in the preoperative assessment that influence the degree of surgical resection. The objective of this study is to identify these factors taking into account characteristics, either patient or tumor, that intervene in the degree of resection of skull base meningiomas, and propose a scale to assess the probability of total resection.
An observational, retrospective study was conducted, collecting data from clinical histories of patients operated with transcranial approach of skull base meningiomas during the period 6/2018 to 6/2022 by our neurosurgical team of the Güemes Sanatorium, CABA, Argentina. Patients older than 18 years, without previous operations and with preoperative contrast MRI and brain tomography were included. Patients younger than 18 years of age, with previous surgical interventions and with incomplete presurgical studies were excluded. Epidemiological and clinical characteristics of the patient were analyzed, as well as characteristics of the tumor, whether location, size, imaging and whether he has previous embolization or not. The degree of resection was measured with the traditional Simpson classification and was also divided into total (Simpson I, II and III) and subtotal (Simpson IV and V) resection (Figure 1).
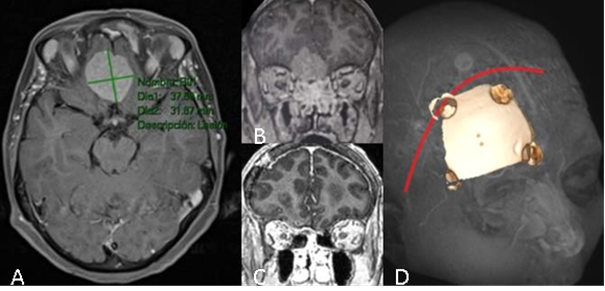
Figure 1: Representative images of patients operated on for meningioma of the anterior skull base of olfactory groove. A: T1 sequence with magnetic resonance contrast, axial slice. B: Same lesion coronal cut C: coronal Cort of postoperative imaging. D: approach and craniotomy performed.
Then, with the results obtained, a scale was proposed to graduate the probability of total or subtotal respectability of meningioma, taking into account the variables that had statistical significance (p < 0.05). Finally, a literature review was conducted in order to compare results with other series.
Protocols and definitions of the variables studied
Patients were analyzed according to age in three cohorts: <40> 60 years. For the clinic, patients were divided into those asymptomatic at the time of diagnosis and symptomatic. Meningiomas of anteromedial localization were defined as those of the olfactory sulcus, sphenoid planum and tuberculum sellae. The anterolaterals are those that arise from the sphenoid wing, including those of the inner segment or clinoidal, those of the medial segment or wings and those of the lateral segment or pterional 10. Those of medial location were those of the cavernous sinus. And those of posterior location the petroclival meningiomas and the cerebellar ponto angle. For the size, the highest value obtained in any of its diameters was taken into account and divided into <3> 5 cm. Among the characteristics we obtained from the imaging studies, we collected whether or not intratumoral calcium was observed, if they had perilesional edema, if they had bone invasion, and their characteristics in sequence T1 and T2. Information was also obtained on whether or not preoperative embolization was performed. Thedegree of resection was categorized according to the Simpson scale based on the intraoperative observation of the surgeon and its description in the surgical part; also comparing the results with resonance with gadolinium postoperative control. Simpson being grade I total removal of meningioma and dura mater, grade II total tumor removal and dura mater coagulation, grade III total tumor removal without dura mater coagulation, grade IV partial resection and grade V decompression or biopsy. We speak of total resection when a Simpson I, II and III was achieved, and subtotal resection with Simpson IV and V.
Taking the results of the variables studied of categorical type and with the database obtained, an analysis was carried out using frequent descriptive statistics and inferential statistics with chi square. SPSS version 25 or JAMOVI was used.
Patient characteristics
A total of 23 patients with skull base meningiomas were operated on during the study period (Table 1). Of these, 95% (n 22) were female. With respect to age, 21.7% (n:5) were younger than 40 years, 39.1% (n:9) between 40 and 60 years old and 39.1% (n:9) were older than 60 years. 73.9% (n:17) had clinical manifestation and 26% were asymptomatic at the time of diagnosis.
Tumor characteristics
The most frequent location was anterolateral with 47.8% (n:11), then posterior with 30.4% (n:7), anteriomedial 17.4% (n:4) and finally medial 4.3% (n:1). 4.3% (n:1) of tumors were smaller than 3 cm, 78.3% (n:18) measured between 3 and 5 cm, and 17.4% (n:4) were smaller than 5 cm; being less than 5 cm 82.6% (n:19).73.9% (n:17) of tumors did not have embolization prior to surgery
Imaging features of the tumor
52.2% (n:12) of meningiomas had perilesional edema and 17.4% (n:4) had intratumoral calcium. Bone invasion was found in 8.7% (n:2). A 34.8% (n: 8) were hyperintense in T2, 43.5% (n: 10) isointense and characteristic heterogenies 21.7% (n:5). Regarding its behavior in sequence T1 30.4% (n: 7) was hypointense and 69.6% (n: 16) isointense.
Degree of exeresis
Simpson I resection was achieved in 4.3% (n:1) of patients, Simpson II in 47.8% (n:11) of patients, Simpson III and IV in 21.7% (n:5) respectively, and Simpson V in 4.3% (n:1).
| Frecuencia | Porcentaje | |
| CLINICA | ||
| Sintomático | 17 | 73,9 |
| Asintomático | 6 | 26,1 |
| EDAD | ||
| <40> | 5 | 21,7 |
| 40-60 | 9 | 39,1 |
| >60 | 9 | 39,1 |
| LOCALIZACION | ||
| Anteromedial | 4 | 17,4 |
| Anterolateral | 11 | 47,8 |
| Medial | 1 | 4,3 |
| Posterior | 7 | 30,4 |
| TAMAÑO | ||
| <3> | 1 | 4,3 |
| 3-5 cm | 18 | 78,3 |
| >5 cm | 4 | 17,4 |
| EMBOLIZACION | ||
| No | 17 | 73,9 |
| Si | 6 | 26,1 |
| EDEMA PERILESIONAL | ||
| No | 11 | 47,8 |
| Si | 12 | 52,2 |
| CALCIO | ||
| no | 19 | 82,6 |
| Si | 4 | 17,4 |
| INVASIONOSEA | ||
| No | 21 | 91,3 |
| Si | 2 | 8,7 |
| T2 | ||
| Hiper | 8 | 34,8 |
| Iso | 10 | 43,5 |
| heterogeneo | 5 | 21,7 |
| T1 | ||
| Iso | 16 | 69,6 |
| Hipo | 7 | 30,4 |
| GRADO DEEXERESIS | ||
| I | 1 | 4,3 |
| II | 11 | 47,8 |
| III | 5 | 21,7 |
| IV | 5 | 21,7 |
| V | 1 | 4,3 |
Table 1: Frequency and percentage of variables.
Regarding inferential results, two types of analysis were performed using the Chi-square test. On the one hand, the study variables were associated with the degree of excision measured with the Simpson scale taking the different five levels I, II, III, IV and V (Table 2). Only associations with location and size were found, with moderate and high effect sizes (Crammer's V).
| (p) | |
| Localización | 0,002 |
| Edad | 0,238 |
| Clínica | 0,487 |
| Tamaño | 0,001 |
| Embolización | 0,724 |
| Edema | 0,172 |
| Calcio | 0,600 |
| Invasión ósea | 0,096 |
| T2 | 0,427 |
| T1 | 0,213 |
Table 2: Association of variables with Simpson's degree.
On the other hand, the variables were associated with the measures of the Simpson scale divided as total resection (I, II and III) partial resection (grade IV and V) (Table 3). Thus, associations were found between bone invasion and grade, with moderate and high effect sizes (Crammer's V). No associations were found between the rest of the variables with the Simpson scale (p > .05).
| (p) | |
| Edad | 0,814 |
| Clínica | 0,091 |
| Localización | 0,131 |
| Tamaño | 0,089 |
| Embolización | 0,638 |
| Edema | 0,408 |
| Calcio | 0,231 |
| Invasión ósea | 0,013 |
| T2 | 0,705 |
| T1 | 0,226 |
Table 3: association with total or subtotal resection.
Proposed scale
Given the results objectified and described above, three variables with statistical significance were found from the inferential analysis: tumor size, location and bone invasion.
For the scale we decided to use the three variables: location (anterior 1 point, posterior 2 points, medial 2 points and medial involving cavernous sinus 3 points), size (<5>5 cm cm 2 points) and bone invasion (not 1 point but 2 points) (Table 4).
| Localización | anterior | 1 |
| posterior | 2 | |
| medial | 2 | |
| medial(C) | 3 | |
| Tamaño | < 5 cm | 1 |
| > 5 cm | 2 | |
| Invasión ósea | No | 1 |
| Si | 2 |
Table 4: Presurgical scale
The minimum score is 3 and the maximum is 7. The probability of total resection with a score of 3, moderate with a score of 4 and low with a score of 5 or more was considered high (Table 5).
| Grado | Puntaje |
| Alto | 3 |
| Moderado | 4 |
| Bajo | >5 |
Table 5: scale score.
Of the total of our series (Table 6) 11 had a score of 3 points and all had total resection (Simpson I, II and III); 10 patients scored 4, 6 of them with total resection and 4 with subtotal resection. Finally, 2 patients had a score of 5 and both had subtotal resection (Figure 2).
| Total (n) | Resección total | Resección subtotal | |
| 3 puntos | 11 | 1 | 0 |
| 4 puntos | 10 | 6 | 4 |
| 5 puntos | 2 | 0 | 2 |
Table 6: Patient score from our study.
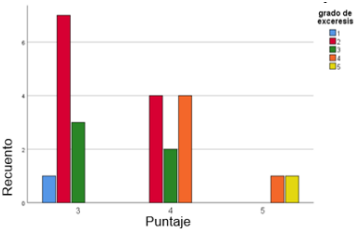
Figure 2: patients with different degrees of excision measured in Simpson and their relationship with the score obtained from our scale.
When performing an inferential analysis, an association was observed between the scale performed and the degree of resection (p: 0.005) (Table 7 and 8).
| Significación asintótica (bilateral) | |
| Chi- cuadrado de Pearson | 0,005 |
Table 7 and 8: association between proposed scale and degree of resection.
In our series, 23 patients were operated on in the period 06/2018 - 06/2022; Within the variables analyzed, we found that both the location, size and bone invasion of the meningioma were related to the degree of resection. Of the total number of patients studied, a complete exeresis (Simpson I, II and III) was achieved in 73.8%. In different publications, a correlation was shown between the location of meningiomas and the degree of excision achieved, with the skull base being the site where less complete resection is achieved11. Meling. et al. in a study of 1148 patients, they found that in 68% of skull base meningiomas achieved total excision, compared to 89?hieved in tumors of another location [12]. In our study, anteromedial and anterolateral skull base meningiomas (which together form the anterior skull base) were the ones with the best degree of exeresis obtained, measured on the Simpson scale. There are currently reviews that describe more resectability in tumors of anterior base compared to those of medium or posterior base [13]. Although when we talk about anterior skull base, we cannot ignore the progress of the endoscopic transnasal approach for the management of this pathology, and although there are still controversies, there are studies in which an increase in the degree of resection has been observed in the transcranial approach and lower comorbidities compared to the endoscopic approach [14]. However, in small patients, the transnasal endoscopic approach for many neurosurgical teams is usually the primary indication [15]. In our series, the size of the meningioma was related to the degree of excision, more than 78% of tumors smaller than 5 cm had a complete resection. Several. Studies took 5 cm as a cut to talk about large meningiomas and described that, especially at the skull base, size influences the degree of excision [16,17,18] Bone invasion may be a preoperative predictor of the extent of surgical resection [19]. A series that incorporated data from 1469 meningiomas and analyzed predictive factors related to the surgical extent of resection concluded that clinic, location at the base of the skull and bone invasion were significant predictors of a low degree of resection (Simpson IV and V) [20]. In our sample, an association was observed between bone invasion and degree of excision, all patients with invasion (8%) had a subtotal resection. Different studies described that in elderly patients’ unfavorable postoperative outcomes are more related to previous functional status and comorbidities and not so much to the degree of excision measured in Simpson [21,22,23]. However, the main predictor of a poor postoperative functional outcome is the intraoperative complications themselves, which are observed in a higher percentage in elderly patients [24]. Therefore, subtotal resection with adequate debulking in exchange for greater safety for meningiomas located near complex neurovascular structures is usually preferable in these patients. In our study, no relationship was observed between Simpson's grade and age. Although in this study no relationship was observed between the patient's clinic, that is, whether he is symptomatic or asymptomatic at the time of diagnosis, with the degree of excision; In a recent study [20] symptomatic patients achieved a lower degree of exeresis compared to asymptomatic patients. In our results, preoperative embolization was not related to the degree of resection. The review did not find any direct benefit associated with the degree of excision of embolized meningiomas before the operation [25]. There have been attempts to objectify the best indication for preoperative embolization and its benefits according to the size and vascularization of the meningioma. A vascularization index has recently been performed by measuring the flow vacuum of the meningioma obtained from a volumetric T2, and better bleeding control was observed in patients with high index and with previous embolization compared to those not embolized [26]. According to the literature, between 38% and 67% of meningiomas have perilesional edema [27]. We found no relationship between the degree of excision and the presence of edema in tumors within our work. Vignes et al in a study of 30 patients where he relates edema and prognosis in meningioma surgery, concludes that the presence of edema affects the surgical prognosis and confers a higher risk of morbidity and postoperative complications, but did not make a direct correlation between meningiomas with perilesional edema and degree of excision [28]. If it has been observed that a high volume of edema correlates with a higher incidence of recurrence, regardless of biological type and histological grade [29]. Approximately 15% of meningiomas may have different patterns of calcification. Zhang et al [30] in a report of 58 cases achieved a Grade III Simpson resection in 52 cases and III in 6. Calcification was associated with high-grade meningiomas and it has been shown that non-calcified tumors may have a greater proliferative potential than calcified tumors [31]. In our study, no relationship was observed between the degree of resection and intertumoral calcium. Given the importance of knowing the type of tumor consistency when addressing this pathology, attempts have been made to predict it in presurgical studies, as well as intraoperative scores have been proposed [32]. There are several studies that related hyperintensity in T2 with soft tumors; It may be related to higher water content. While the lower signal in T2 for hard tumors could be due to less water and more collagen and calcium content. Although there are several articles that show the indication of the T2 signal to predict consistency, it is not yet a validated method [33]. Likewise, in most of the studies reviewed, it has not been found that there is an association between T1 and meningioma consistency. However, Hoover et al found that meningiomas that were hyperintense at T2 and hypointense at T1 were more likely to be soft, while those that were hypointense at T2 and isointense at T1 were probably firm [34]. Elastography is a new technique that takes advantage of the fact that a pathological process alters the elastic properties of the affected tissue. This change in elasticity is detected and visualized by MRI using transverse waves to assess tissue displacement in all directions [35]. Elastography proved to have a good degree of accuracy in predicting the consistency of meningiomas as well as other types of tumors [36]. Although it is not yet available, it is a tool to be taken into account when its accessibility is no longer limited [37]. In our analysis, hyperintensity at T2 or hypointensity at T1 did not correlate with the degree of excision; and then analyzing patients in which hyperintensity in T2 and hypointensity in T1 were combined, no relationship was observed with resection. Since the prognosis and survival of the patient differs markedly if the meningioma is WHO grade I, II or III, it is important to know that many factors that complicate total resection are also factors that are associated with suspected malignancy. Clinic, size, perilesional edema, irregularity and heterogeneity, as well as imaging aspects based on ADC, were shown to be factors that increase the probability of meningioma malignancy; as well as the location outside the skull base [38,39,40]. Among the different characteristics, size is the only one that had statistical significance at the time of subtotal resection in our series [41]. It was observed that the recurrence of meningiomas, regardless of their location, varies according to the degree of malignancy only from a Simpson IV resection. Although we proposed a scale with presurgical data, the contribution of histomolecular studies gives us a more adequate prognosis, so it is necessary to take them into account. Studies focusing on factors predicting meningioma recurrence after subtotal resection suggest that minimizing residual tumor volume of less than 4 to 5 cm3 may be associated with increased recurrence-free survival. The goal should be to minimize the residual volume so that it is amenable to postoperative radiosurgery. Some authors have even shown that the combination of radiotherapy with subtotal resection is associated with recurrence-free and overall survival rates similar to those of total resection [42]. After the statistical analysis we proposed a preoperative graduation scale, with which according to the total score obtained we can infer the probability of total excision. For the scale we used location, size and bone invasion as parameters (Figure 3, 4 and 5). Within location, cavernous sinus meningiomas had a higher score (3 points). The justification for this particularity is based on the fact that, given the difficulty and complications involved in surgery, the current trend is decompression followed by radiosurgery [43]. Different scales have been tried previously [44].

Figure 3: Patient with anteromedial skull base meningioma (AM) (1 point), size less than 5 cm (1 point), no bone invasion (1 point), total score: 3, high probability of total resection. A: location of lesion at the base of the skull. B: 3D reconstruction with approach. C: resonance with presurgical sagittal cut contrast. D: postsurgical sagittal cut contrast resonance with total resection.

Figure 4: Patient with anterolateral skull base meningioma (LA) (1 point), size more than 5 cm (2 points) without bone invasion (1 point), total: 4 points, moderate probability of total resection. A: location of lesion at the base of the skull. B:
Resonance with presurgical sagittal cut contrast. C: intraoperative image showing meningioma with arachnoid plane. D: emptying and reducing size with scalpel blade 11. E: resection partial dura mater and coagulation of the same. F: surgical lodge without tumor remnant, Simpson resection 2. Postsurgical sagittal cut with subtotal resection of lesion.

Figure 5: Patient with petroclival skull base meningioma (PC) (2 points), in its maximum diameter measured 5 cm (2 points) without bone invasion, total: 5 points, low probability of total resection. A: location of lesion at the base of the skull. B: combined approach. C: resonance with presurgical sagittal cut contrast. D: resonance with contrast.
One of the most widespread is that of Magitll. and col. of the meningiomas of tuberculum sellae. They proposed a score based on tumor size, optic canal invasion, and arterial encapsulation that could predict EOR (extent of resection) and postoperative visual outcomes. Like us, they used tumor size, but they observed that a smaller tumor size was significantly associated with better or stable vision after the operation, but not with the extent of resection [45]. Although with the particularities of the tumor that make us reach a low or high score it can already be deduced whether or not the surgery will provide a total resection; We think that, with a simple scale, easy to perform and with information that is obtained without much complexity within the presurgical evaluation, the expected result can be dichotomized quickly and thus plan the surgery taking into account realistic objectives. It can also help us to know what tools, whether diagnostic, intrasurgical and post-surgical may be required. In order to provide the patient with adequate treatment and with the least possible morbidity.
Among the most complex procedures of the neurosurgical specialty, without a doubt, are the surgeries of the skull base meningiomas. Achieving the highest degree of resection with the lowest postoperative morbidity remain the objectives pursued in this type of surgery. Taking into account the different particularities of the tumor, as well as that of the patient and its comorbidities, it is often not only necessary but beneficial to perform a subtotal resection. To obtain good results by providing individualized planning, it is important to take into account the different characteristics that influence surgery and that allow us to predict the degree of excision, and thus anticipate surgical results and the requirement for adjuvant treatment. Our study showed a statistically significant relationship between the location (0.002), size (0.001) and bone invasion (0.013) of the meningioma with the degree of excision achieved. We proposed a simple scale to measure the possibility of total resection taking into account these variables
Given the low number of patients (n23) because it is a rare pathology, the associations between variables may be biased, leading to a high probability of committing type II error (that there are differences, but cannot be detected by inferential analyses), and a low statistical power. Together, we understand its limitations as it is a retrospective observational study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
