
Research Article | DOI: https://doi.org/10.31579/2692-9759/154
1Department of Biostatistics and Epidemiology, University of Health and Allied Sciences, Ho, Ghana.
2Department of Health, Physical Education and Recreation, University of Cape Coast, Cape Coast, Ghana.
*Corresponding Author: Anthony Edward Boakye, Department of Health, Physical Education and Recreation, University of Cape Coast, Cape Coast, Ghana.
Citation: Rita Tekpertey, Anthony Edward Boakye, (2025), Factors Influencing Patients’ Adherence to Tuberculosis Treatment Before and During COVID 19 Era in the Hohoe Municipality, Ghana, Cardiology Research and Reports, 7(2); DOI:10.31579/2692-9759/154
Copyright: © 2025, Anthony Edward Boakye. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 March 2025 | Accepted: 13 March 2025 | Published: 24 March 2025
Keywords: adherence, COVID 19, pandemic, patients, tuberculosis treatment
Background: Obviously, if a TB patient does not adhere to treatment, symptoms may not be relieved or the disorder may not be cured.
Objective: The study investigates the factors influencing patients’ TB treatment adherence before and during the COVID-19 pandemic period in the Hohoe Municipality, Ghana.
Methods: This descriptive study employed cross-sectional study design with 114 participants who were randomly selected from the Directly Observed treatment, short–course (DOTs) register. Descriptive analysis was conducted to summarise participants’ responses under each research question. Simple logistic regression analysis was done to determine factors that influence TB patients’ treatment adherence before and during COVID-19. Results: The study revealed an increase in treatment success rate during the COVID-19 period. That is from 82.7% before COVID-19 to 89.1% during COVID-19. The study revealed a decrease in default 1.1% and death 4.3% during the COVID-19 period. Out of 114 participants, majority (81.6%) indicated that there was an adequate supply of medicine during the COVID-19 period for their intake anytime they visited the TB clinic. About seventy-three (72.8%) of the participants reported that they had difficulties in receiving their medication due to the lockdown during the COVID-19 period. Participants who received counselling about TB before treatment was significant at [AOR=4.90(CI: 1.34-17.81), p=0.016]. Satisfied with TB health services was significant at [AOR=18.2 (CI: 5.16-64.12), p=0.001]. Participants who attained a tertiary level of education was significant at [AOR=0.07 (CI:0.01–0.47), p=0.005].
Conclusion: Despite the significant disruption of healthcare activities during the COVID-19 pandemic, verified TB treatment adherence at the Hohoe Municipality, Volta Regional Hospital was sustained in the setting of increased vDOT utilization.
Tuberculosis (TB) is a preventable and usually curable disease [1, 2]. Yet in 2023, it became the world’s leading cause of death when it claimed the lives of 1.25 mil-lion people from a single infectious agent including 161 000 people with HIV [3]. It has been estimated that every year more than 10 million people fall ill with TB. It is noted to be the leading cause of death of people with HIV and also a major contributor to antimicrobial resistance [4, 5]. Globally, the total TB cases estimated in 2023 were at 10.8 million a slight increase from 10.7 million in 2022 although still much higher than 10.4 million in 2021 and 10.1 million in 2020 [3, 1]. Most of the people who develop TB disease each year are in 30 high TB burden countries, which accounted for 87% of the global total in 2023. Five countries accounted for 56% of the worldwide total: India (26%), Indonesia (10%), China (6.8%), the Philippines (6.8%) and Pakistan (6.3%) [6]. In 2023, 55% of people who developed TB were men, 33% were women and 12% were children and young adolescents [7]. TB is present in all countries and age groups. TB, which usually affects the lungs can be treated with antibiotics but can be serious if not treated [8].
TB treatment involves taking antibiotic medicines [9]. Treatment can last 4 to 9 months or longer [10]. Taking TB medicines and completing treatment will not only cure TB but it will also improve the body’s ability to fight other infections [11]. TB treatment varies in duration, types of anti-TB drugs prescribed and dose and frequency of each drug [12, 13]. Currently, the recommended treatment for drug-susceptible TB is a six-month course of four antibiotics namely (isoniazid, rifampicin, ethambutol and pyrazinamide) [14]. To be effective, medications need to be taken daily for 4–6 months [15, 16]. It is dangerous to stop the medications early or without medical advice as it can prompt TB bacteria in the body to become resistant to the drugs [17].
Drug-resistant TB can take longer to treat and be more complicated. Multidrug-resistant TB (MDR-TB) remains a public health crisis and a health security threat [18]. Only about 2 in 5 people with drug resistant TB accessed treatment in 2023 [19, 20]. Global efforts to combat TB have saved an estimated 79 million lives since the year 2000. Ending the TB epidemic by 2030 is among the health targets of the United Nations Sustainable Development Goals (SDGs) [21, 22]. Promoting TB drug adherence for TB patients is vital to lessen the impact of the disease [23, 24].
Adherence is defined by the World Health Organisation (WHO) as the extent to which a person’s behaviour—taking medication, following a diet, and/or executing lifestyle changes—corresponds with agreed recommendations from a health care provider [25]. Obviously, if a person does not adhere to TB treatment, symptoms may not be relieved or the disorder may not be cured [26, 27]. However, not adhering may have other serious or costly consequences [28]. Not adhering is estimated to result in 125,000 deaths [29, 30]. In addition, it is thought that up to 23% of nursing home admissions, 10% of hospital admissions, and many doctor visits, diagnostic tests, and unnecessary treatments could be avoided if people take their drugs as directed [31]. Not only does not adhering add to the cost of medical care, it can also worsen the quality of life. Not taking all prescribed doses of an anti-biotic can cause an infection to flash up again and may be contributing to the problem of drug-resistant bacteria [32, 33, 34]. People are more likely to adhere to treatment if they have a good relationship with their doctor and pharmacist [35, 36].
Worldwide, non-compliance is a major obstacle to the effective delivery of health care [37, 38]. Efforts to im-prove compliance have been aimed at simplifying medication packaging, providing effective medication reminders, improving patient education, and limiting the number of medications prescribed simultaneously [38]. An estimated half of those for whom treatment regimens are pre-scribed do not follow them as directed [39, 40]. It is estimated that over half the medications prescribed for people with chronic diseases are not taken as directed [41]. Taking medication correctly may seem like a simple or personal matter, but non-adherence, or not taking medication as directed, is a complicated and common problem [38].
However, COVID-19 had a major impact on National TB Programme, since the patients stopped visiting or could not visit hospitals due to the pandemic and result-ant lockdowns [42]. There were serious impacts since the resources and personnel allotted for TB were diverted for COVID-19 work [42, 43]. Despite that, diagnosis of TB came down drastically [44]. Even when people had cough, they stopped visiting hospitals due to fear of getting COVID or getting isolated [45]. This in return paved way for spreading of infection to other family members too. Many patients suffered during the Pandemic, which even caused several deaths among TB patients [46]. The COVID 19 adversely affected treatment adherence and adverse drug reaction monitoring as health workers were deployed to the COVID-19 response [47, 48]. Yet, the WHO stressed the importance of continuing essential health services to protect affected persons and those at risk [49, 50]. Therefore, it was crucial that national pro-grammes continue to provide TB services while at the same time maintaining their response to the COVID-19 outbreak [48, 51]. During the pandemic, tuberculosis-related deaths rose from 5.0%-to-12.7% [52].
Ghana’s adherence strategy currently involves the use of the DOTS under Community Based Treatment Care. Under this, treatment supporters are chosen together by the health worker and the TB client to monitor their daily doses of treatment at the community level and supervised by the nearest health facility staff [53, 54, 55]. People do not realize the real damage or effects of non-adherence. When people with chronic conditions such as TB disease do not take medication as directed, the repercussions can be severe [56]. Patients with TB are expected to adhere to treatment plans at a level of more than 90% to facilitate a cure or have a favourable outcome [57, 58].
Sadly, studies conducted in Ghana recorded low rate of TB treatment adherence. For instance, [59] recorded an adherence rate of 75%, [60] found a 63%adherence rate, [61] reported a prevalence of 22% noncompliance to treatment among TB patients. Despite local, national, and worldwide efforts to prevent and control TB, patients continue to stop taking their medications before they may be declared cured [53, 56, 62]. Therefore, a deeper com-prehension of the factors influencing patients’ TB treatment adherence before (2017-2018) and during COVID 19 (2019-2020) period is necessary to improve TB treatment outcomes. Hence the focus of the study.
Specifically, the study sought to assess the TB treatment outcome before covid-19 (2017-2018) and during the covid-19 pandemic (2019-2020) in the Hohoe Municipality, Ghana; analyse TB treatment adherence challenges patients encounter during covid-19 pandemic period in the Hohoe Municipality, Ghana; examine health facility-related factors that influence patients’ adherence to TB treatment in the Hohoe Municipality, Ghana and lastly, ascertain the factors that are associated with patients’ adherence to TB treatment before (2017-2018) and during the covid-19 (2019-2020) period in the Hohoe Municipality, Ghana.
Study Site and Participants
Hohoe Municipality was chosen for the study. The Municipality was chosen because in 2013, 1763 TB cases were detected in the Volta Region [63], out of which 1,340 are undergoing treatment. 344 of them have been completely cured. Moreover, TB is noted as among the three top causes of death among women from 15-to-44years [63]. Records available in the Volta Region show that TB cases remain high, with about 60 and 58.2 TB cases per 100,000 population estimated in 2016 and 2017, respectively [61]. The study participants included TB patients who registered and received treatment at the counselling unit of Hohoe Municipal hospital before covid-19 (2017-2018) and during the period 2019 to 2020. Also, all records on TB patients for the period January 2017 to December 2020 were reviewed. The Volta Regional Hospital is a moderately-sized public hospital serving the Hohoe municipality in the northern part of the Volta Region of Ghana.
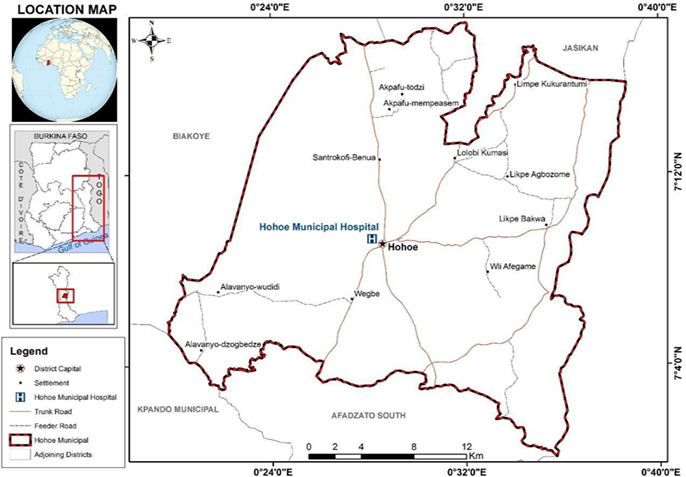
Figure 1: Map of Hohoe Municipality.
Source: CERGIS (2022).
Study Design and Data Source
A descriptive cross-sectional study design was adopted. The design was appropriate as it enables data to be collected on an individual’s characteristics at the time of the study alongside information about the outcome, and the association between the individual’s characteristics and the outcome of interest [64, 65]. Data were collected from TB patients who registered and received treatment at the counselling unit of Hohoe Municipal hospital before (2017-2018) and during the covid-19 period (2019 to 2020). As well, a retrospective review of TB treatment cards of patients who received tuberculosis treatment in the counselling unit of the hospital were also used.
Inclusion Criteria
All available TB records from January 2017 to December 2020 was extracted. Also, the study included all TB patients who were on treatment at the Volta Regional Hospital in the midst of COVID-19 pandemic.
Exclusion Criteria
Records with incomplete data were excluded from the study as well as TB patients who could not be reached via the contact telephone number or address provided in the register were excluded.
Sampling Procedure
Systematic random sampling technique was employed for the study. This technique helped the investigators to select participants to be included in the sample based on a systematic rule, using a fixed interval. In the field, the rule permitted us to include the last patient from every 5 patients. Therefore, we included patients with the following numbers (5, 10, 15, 20, 25, ...etc.) [66].
Sample Size Determination
A sample size of 114 was recruited for the study with the help of [67] sample size determination formula. The sample was selected from TB clients registered at the Volta Regional Hospital from the year 2017 to 2020 cohort.
Where;
s= required sample size,
X = the table value of chi-size for 1 degree of freedom at the desired confidence level (3.841)
N = the TB population size (118), Hohoe
p= the population proportion (as assumed to be 0.50 since this will produce the maximum sample size),
d = the degree of accuracy expressed as a proportion (0.05)
s = 109
Adding a non-response rate of 5%, actual sample size = (109×0.05) + 109 = 114. Therefore, the sample size for the study was 114 TB patients.
Data Collection Procedure
Data were collected from participants in the field with the help of three research assistants using a standardized questionnaire designed in a Kobo Collect software. Treatment outcomes were investigated by reviewing the records of all TB patients who had been diagnosed with active TB as defined by WHO criteria and who received anti-TB treatment between January 2017 and December 2020 using a data collection sheet. The data collection sheet contained socio-demographic characteristics of the study participants and information on treatment outcomes (cured, treatment completed, defaulted, died or treatment failed).
Quality Control
The following measures were put in place to ensure that the data collected were of good quality:
Three research assistants were recruited and trained to assist in data collection for the study.
The principal investigator supervised the data collection.
The data collected were critically examined at the end of each day. Data handled by the research assistants were cross-checked by the principal investigator for consistency and completeness by verifying from the source records (TB cards). Research assistants double- checked data gathered by the principal investigator with the aim to achieve accuracy.
The questionnaire was pretested at the Ho Teaching Hospital (Trafalgar) to know what to add or remove from the items on the questionnaire.
Both data collected from the field and that obtained from the retrospective record review of previously treated TB patients were analyzed using STATA version 17.0. The effects of predefined potential risk factors on the likelihood of adherence were modeled using logistic regression, and odds ratios with corresponding 95% confidence intervals was reported as the measures of the degree of associations. Variables significantly associated with the likelihood of treatment adherence in the analysis (i.e., P value<0.05) were included in a multivariable logistic regression model to determine their adjusted relative contributions in predicting the likelihood of treatment adherence. Using the retrospectively extracted treatment outcomes and other patient factors, similar procedures were followed to identify variables which were significantly associated with the likelihood of having unsuccessful treatment outcomes while simultaneously adjusting for the effect of other variables. Results were reported as being statistically significant whenever p value was not greater than the cutoff 0.05.
Ethical issues
Data collection commenced after the University of Health and Allied Sciences Ethical Review Committee had ap-proved the research protocol and granted ethical clearance (with ID number UHAS-REC A./111/21-22). Additionally, in the field, informed consent was obtained from participants after the aims, significance, benefits and risks involved were fully explained to them. Anonymity was ensured by assigning code and numbers to the questionnaire instead of using their names. The respondents were assured that the information gathered was for the purposes of academic and nothing else. The participants were allowed to decide whether to participate in the study or not.
This section presents the findings of the study. The results are presented in line with the objectives of the study.
Socio-Demographic Characteristics of Respondents
The mean age of the participants was 41.3(SD: +17.1) years. Twenty-nine per cent (29.0%) of the participants were between 50years and above. About fifty-three per cent (52.6%) of the participants were within the married category at the time of the study. A little above thirty-five per cent (35.1%) were Ewes and close to 15 per cent (14.9%) had primary school education. More than half (50.9%) of the respondents stay at a distance of 0-5km close to their clinic (Table 1).
| Variables | F | % |
| Sex | ||
| Male | 90 | 79.0 |
| Female | 24 | 21.0 |
| Age(years) Mean Age (SD) | 41.3(±17.1) | |
| Less than 20 | 16 | 14.0 |
| 21-30 | 21 | 18.4 |
| 31-40 | 18 | 15.8 |
| 41-50 | 26 | 22.8 |
| 50+ | 33 | 29.0 |
| Ethnicity | ||
| Ewe | 40 | 35.1 |
| Guan | 15 | 13.2 |
| Akan | 25 | 21.9 |
| Ga | 18 | 15.8 |
| Others | 16 | 14.0 |
| Education level | ||
| No formal education | 23 | 20.2 |
| Primarylevel | 17 | 14.9 |
| JHS | 30 | 26.3 |
| Secondary | 20 | 17.5 |
| Tertiary level | 24 | 21.1 |
| Marital status | ||
| Single | 31 | 27.2 |
| Married | 60 | 52.6 |
| Divorced | 23 | 20.2 |
| Distance home-clinic (km) | ||
| 0-5km | 58 | 50.9 |
| >5km | 56 | 49.1 |
| Residence area | ||
| Rural | 46 | 40.4 |
| Urban | 68 | 59.6 |
| HIV status | ||
| Positive | 17 | 14.9 |
| Negative | 97 | 85.1 |
| Alcohol use | ||
| No | 71 | 62.3 |
| Yes | 43 | 37.7 |
| Smoking | ||
| No | 98 | 86.0 |
| Yes | 16 | 14.0 |
Table 1: Socio-Demographic Characteristics of Respondents
Source: Fieldwork (2022).
TB Treatment outcome Before COVID-19 (2017-2018) and During COVID-19 Pandemic (2019-2020)
Figure 2 below represents the treatment outcomes for 344 records, for the period before COVID-19 (2017-2018) and during COVID-19 (2019-2020). The figure shows an increase in treatment success rate during the COVID-19 period from 82.7% (cured 46.4%+36.3%) before COVID-19 to 89.1% (cured 47.3%+41.8%) during COVID-19 (see Figure 1). Again, the figure revealed a decrease in loss-to-follow up from 1.7% before covid-19(2017-2018) to 0.6% during COVID-19(2019-2020) and death from 14.6% be-fore COVID-19(2017-2018) to 10.3% during the COVID-19(2019-2020) period (see Figure 1). The various treatment outcomes such as treatment failure etc. and their rates are presented in the graph.

TB Treatment Adherence Challenges During COVID-19 Era
In our pursuit to unravel TB treatment adherence chal-lenges during covid-19 instigated a number of questions ranging from medicine availability at DOTs centre, find it difficult to receive medication, etc. The results are pre-sented in Table 2.
| Variables | F | % |
| Availability of medicines at the DOTSCentre | ||
| No | 21 | 18.4 |
| Yes | 93 | 81.6 |
| Difficult in receiving medication due to the lockdown | ||
| No | 31 | 27.2 |
| Yes | 83 | 72.8 |
| Difficult to go for medication due to the fear of COVID 19 | ||
| No | 43 | 37.7 |
| Yes | 71 | 62.3 |
| Fail to collect yourmedication because of transportation problems during the COVID 19 pandemic | ||
| No | 99 | 86.8 |
| Yes | 15 | 13.2 |
| Fail to visit the facility for your medicine because you had no access to food | ||
| No | 107 | 93.9 |
| Yes | 7 | 6.1 |
| Sometimes forget to take TB pills during the COVID 19 pandemic | ||
| No | 74 | 64.9 |
| Yes | 40 | 35.1 |
| Family members encourage you to continue taking your medicines during the pandemic | ||
| No | 53 | 46.5 |
| Yes | 61 | 53.5 |
| Sometimes stop taking your medication, when you felt better | ||
| No | 81 | 71.1 |
| Yes | 33 | 28.9 |
| Felt hassle about sticking to your TB treatment plan during the COVID 19 pandemic | ||
| Yes | 5 | 4.4 |
| No | 109 | 95.6 |
| Long distance hindered you from collecting your medications from the facility during Covid-19 | ||
| No | 97 | 85.1 |
| Yes | 17 | 14.9 |
Source: Fieldwork (2022).
Table 2: Patient Adherence to TB Treatment during Covid-19 Pandemic
Out of 114 participants, majority (81.6%) indicated that there was an adequate supply of medicine during the COVID-19 period for their intake anytime they visit the TB clinic (see Table 2). More than seventy per cent (72.8%) of the participants reported that they had diffi-culties in receiving their medication due to the lockdown during the COVID-19 period. Also, less than half (37.7%) of the participants indicated fear of COVID-19 as a reason why they could not go for their medication (see Table 2). Less than ten per cent of the participants (6.1%) indicated that access to food was a reason why they could not visit the health facility for their medication (see Table 2). About sixty-five per cent (64.9%) of the participants re-ported that they sometimes forget their TB pills during the pandemic. More than half (53.5%) of the participants in-dicated that they were encouraged to take their TB medi-cation by their family members (see Table 2).
Participants’ Adherence level to TB Treatment during COVID-19
Figure 3 below is a pie chart showing the distribution of adherence levels to TB treatment among participants. Out of the 114 participants, about sixty-one per cent (60.5%) reported good adherence to TB treatment during COVID-19 while 39.5% reported poor adherence to treatment during COVID-19.
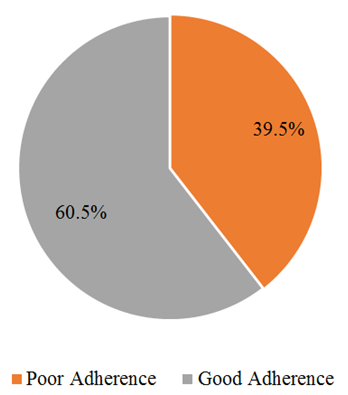
Figure 3: Participants’ adherence level to TB treatment during COVID-19
Source: Fieldwork (2022).
Factors Associated with Adherence to TB Treatment During COVID 19 Period
To be able to ascertain factors associated with TB treatment adherence, participants were asked a number of questions ranging from health education, monthly appointment, counselling, delays, service satisfaction and health facility privacy. The results are presented in Table 3.
| Variables | F | % |
| Health education provided during treatment | ||
| No | 12 | 10.5 |
| Yes | 102 | 89.5 |
| Taking monthly appointment card | ||
| No | 22 | 19.3 |
| Yes | 92 | 80.7 |
| Receive counselling about TB treatment | ||
| No | 26 | 22.8 |
| Yes | 88 | 77.2 |
| Delayed before being served at the DOTs unit | ||
| No | 89 | 78.1 |
| Yes | 25 | 21.9 |
| Satisfy with health service | ||
| No | 49 | 43.0 |
| Yes | 65 | 57.0 |
| Enjoy privacy at the health facility | ||
| No | 62 | 54.4 |
| Yes | 52 | 45.6 |
Table 3: Factors Associated with Adherence to TB Treatment During COVID 19 Period
Source: Fieldwork (2022).
Out of the 114 participants, majority (89.5%) reported that they were provided with health education before they started their treatment while less than twenty per cent (19.3%) indicated they did not take their monthly appointment card (see Table 3). Most, 77.2% of the participants said they were counselled about TB when they visited the facility (see Table 3). Nearly twenty-two per cent (21.9%) of the participants reported that they were delayed at the DOTs center when they went for their medications. More than half (57.0%) of the participants said they were satisfied with the service provided to them at the TB clinic (see Table 3).
Factors Associated with Adherence to TB Treatment During the COVID-19 Period
After adjusting for the possible confounding effect of the variables, participants who attained a tertiary level of education were less likely to adhere to TB treatment during the COVID-19 period with a reduced odd of 93% [AOR=0.07 (CI:0.01–0.47), p=0.005]. The odds among participants who received counselling about TB before treatment were 4.9 times more likely to adhere to TB treatment during the COVID-19 period than those who did not receive any counseling [AOR=4.90(CI: 1.34-17.81), p=0.016]. Participants who were satisfied with TB health services were 18.2 times more likely to adhere to TB treatment during the COVID-19 period than those who were not satisfied [AOR=18.2 (CI: 5.16-64.12), p=0.001].
| Variables | Poor adherence | Good adherence | COR (95%CI), p-value | AOR (95%CI), p-value |
| Sex | ||||
| Male | 34(75.6) | 56(81.2) | Ref | |
| Female | 11(24.4) | 13(18.8) | 0.72(0.29-1.78)0.474 | |
| Age | ||||
| Less than 20 | 10(22.2) | 6(8.7) | Ref | |
| 21-30 | 7(15.6) | 14(20.3) | 3.33(0.85-13.0)0.083 | |
| 31-40 | 7(15.6) | 11(15.9) | 2.62(0.65-10.5)0.174 | |
| 41-50 | 9(20.0) | 17(24.6) | 3.15(0.86-11.5)0.83 | |
| 51 above years | 12(26.7) | 21(30.4) | 2.92(0.85-10.03)0.090 | |
| Ethnicity | ||||
| Ewe | 18(40.0) | 22(31.9) | Ref | |
| Guan | 6(13.3) | 9(13.0) | 1.23(0.37-4.10)0.739 | |
| Akan | 8(17.8) | 17(24.6) | 1.73(0.61-4.95)0.300 | |
| Ga | 8(17.8) | 10(14.5) | 1.02(0.33-3.13)0.969 | |
| Others | 5(11.1) | 11(15.9) | 1.8(0.53-6.14)0.348 | |
| Education level | ||||
| No formal education | 6(13.3) | 17(24.6) | Ref | Ref |
| Primary level | 5(11.1) | 12(17.4) | 0.85(0.21-3.43)0.816 | 1.54(0.15-4.90) 0.858 |
| JHS | 11(24.4) | 19(27.5) | 0.61(0.19-2.01)0.415 | 0 .61(0.59-3.50)0.586 |
| Secondary | 7(15.6) | 13(18.8) | 0.66(0.18-2.42)0.527 | 1.48(0.24-9.27)0.677 |
| Tertiary level | 16(35.6) | 8(11.7) | 0.18(0.05-0.62)0.007 | 0.07(0.012-0.47)0.005 |
| Marital status | ||||
| Never married | 21(46.7) | 10(14.5) | Ref | Ref |
| Married | 16(35.6) | 44(63.8) | 5.78(2.24-14.87)0.000 | 3.19(0.83-12.25)0.092 |
| Divorced | 8(17.8) | 15(21.7) | 3.94(1.26-12.33)0.019 | 1.62(0.31-8.40)0.569 |
| Distance home-clinic (km) | ||||
| 0-5km | 26(57.8) | 32(46.4) | Ref | |
| >5km | 19(42.2) | 37(53.6) | 1.58(0.74-3.37)0.235 | |
| Residence area | ||||
| Rural | 12(26.7) | 34(49.3) | Ref | Ref |
| Urban | 33(73.3) | 35(50.7) | 0.37(0.17-0.84)0.018 | 0.50(0.16-1.51)0.219 |
| HIV status | ||||
| Positive | 38(84.4) | 59(85.1) | Ref | |
| Negative | 7(15.6) | 10(14.5) | 0.92(0.32-2.63)0.876 | |
| Alcohol use | ||||
| No | 29(64.4) | 42(60.9) | Ref | |
| Yes | 16(35.6) | 27(39.1) | 1.12(0.53-2.54)0.700 | |
| Smoking | ||||
| No | 42(93.3) | 56(81.2) | Ref | |
| Yes | 3(6.7) | 13(18.8) | 3.25(0.87-12.12)0.080 | |
| Health education during treatment | ||||
| No | 3(6.7) | 9(13.0) | Ref | |
| Yes | 42(93.3) | 60(87.0) | 0.48(0.12-1.86)0.287 | |
| Taking monthly appointment card | ||||
| No | 10(22.2) | 12(17.4) | Ref | |
| Yes | 35(77.8) | 57(82.7) | 1.36(0.53-3.47)0.52 | |
| Counselling about TB before treatment | ||||
| No | 17(37.8) | 9(13.0) | Ref | Ref |
| Yes | 28(62.2) | 60(87.0) | 4.05(1.61-10.20)0.003 | 4.90(1.34-17.81)0.016 |
| Delayed at the DOTs unit | ||||
| No | 34(75.6) | 55(79.7) | Ref | |
| Yes | 11(24.4) | 14(20.3) | 0.79(0.32-1.93)0.601 | |
| Patient satisfaction with health service | ||||
| No | 34(75.6) | 15(21.7) | Ref | Ref |
| Yes | 11(24.4) | 54(78.3) | 11.13(4.58-27.06)0.000 | 18.2(5.16-64.12)0.00 |
| Privacy by health providers | ||||
| No | 21(46.7) | 41(59.4) | Ref | |
| Yes | 24(53.3) | 28(40.6) | 0.60(0.28-1.27)0.183 |
Table 4: Factors Associated with Adherence Level to TB Care During the COVID-19 Period
Source: Fieldwork (2022). Significant 0.05
TB Treatment Outcome Before COVID (2017-2018) and During the COVID-19 Pandemic (2019-2020)
The COVID-19 pandemic threatens to reverse recent gains in reducing the global burden of tuberculosis disease, and creative approaches to ensuring the continuity of TB care during the COVID-19 pandemic are urgently needed. The overall treatment success rate was lower than national and international targets of at least 90% success rate but consistent with the Volta Region’s performance of less than 85%. The success rate is similar to other studies which reported increase in treatment success among TB patients, 82% in Brazil [68, 69], 83% in Argentina [70], 82% in Mogadishu of Somalia [71]. The difference observed could be ascribed to the differences in the study sample size and characteristics of study participants. A larger sample size was used in the previous studies com-pared to the current study. Treatment success rates im-proved during the pandemic at the Volta Regional Hospital. This could be because TB patients knew they were at high risk of contracting COVID-19 due to their compromised immune system. Therefore, they were more diligent in taking their medication leading to improved treatment outcomes. Also, loss to follow up decreased and this could be as a result of the lockdown which confined people in their places of abode, districts and regions where they could still access the TB treatment which eventually brought to the fore reduction in the lost to follow up.
Patients Adherence to TB Treatment During COVID-19 Pandemic
The adherence rate (60.5%) in this study (was higher than that recorded in Southern Ethiopia (25%) [13], Northwest Ethiopia (21%) [72] and Equatorial Guinea (17.8%) [73], South Korea (56.5%) [74] but lower than rates reported in Ketu North District in the Volta Region of Ghana (81.6%) [75], and Ethiopia (90.0%) [76]. The plausible explanations for the higher adherence rate in our study include increased awareness of TB infection via effective health education in the district and the relatively greater proportion of volunteered treatment supporters. Moreover, differences in methodology including study design, type of sampling technique, sample size, and definition of adherence could account for the dissimilarities in the adherence rates between our study and those recorded in South Korea, Equatorial Guinea and Ethiopia.
Factors Associated with Adherence to TB Treatment During the COVID-19 Period
Participants who attained a tertiary level of education were less likely to adhere to TB treatment during COVID-19 period than their counterparts in this current study. This agrees to a study by [77] that, respondents with a high level of education were less likely to adhere to TB treatment than respondents who had a low level of education. The reason could be that people who are more educated can read and understand available information on TB therefore healthcare workers might assume they al-ready know about TB and may not give them in-depth counselling prior to starting treatment. Also, participants who received some form of counselling before starting their TB treatment were more likely to adhere to treatment during the COVID-19 period. This finding affirms a study by [78] that, patients who receive some counselling before starting their TB treatment always adhere to treatment. The implication is that health counselling improves knowledge related to TB, reduces stigma, stress, and reinforces acceptance within the family and community. It confirms a study by [79] that patient-focused interventions through counselling affect medication adherence, improved knowledge, quality of life, social support, depression, and stigma reduction.
Counselling is essential for people with TB to encourage them to control, take medication regularly, and find a cure. The review pro-vides scientific evidence that health counselling is required by TB patients during the medication to gain knowledge, emotional, psychological, and spiritual support and reduce stigma. Consequently, it will improve medication adherence. Moreover, patient satisfaction was statistically significant related to adherence to TB treatment. An increase overall patient satisfaction on TB treatment service has a positive effect on patient adherence to TB treatment. This is consistent with the study done in Kenya by [80] that higher patient satisfaction with the service at the hospital was significantly associated with higher levels of adherence.
Limitation of this study could be a recall bias since the participants had already completed their treatment and could not remember vividly some of the things that influenced them during the pandemic.
The study sought to investigate the factors influencing patients’ adherence to TB treatment before (2017-2018) and during COVID-19 pandemic (2019-2020) era in the Hohoe Municipality, Ghana using Volta Regional Hospital as the case study. The study found an increase in treatment success rate during the Covid-19 period from 82.7% to 89.1%). The study found good adherence to TB treatment during the COVID-19 pandemic. Attaining a tertiary level of education, receiving counselling about TB before treatment and being satisfied with TB health services during COVID-19 period were the factors associated with adherence to TB care in this current study. Despite the significant disruption of healthcare activities during the COVID-19 pandemic, verified TB treatment adherence at the Hohoe Municipality, Volta Regional Hospital was sustained in the setting of increased vDOT utilization.
Recommendations for Policy
The study recommends that the Ghana Health Service should continue to provide health education and counsel-ling programmes on the disease and treatment adherence to patients on TB treatment.
Stakeholders and NGOs should help provide a package of treatment adherence interventions to patients on TB treatment in conjunction with the selection of a suitable treatment administration option.
CERGIS : The Centre for Remote Sensing and Geographic Information Services
COVID 19: Coronavirus Disease
DOTs : Directly Observed Treatment, Short-course
HIV : Human Immunodeficiency Virus
MDR-TB : Multidrug-resistant Tuberculosis
NGOs : Non-governmental Organizations
SDGs : Sustainable Development Goals
TB : Tuberculosis
WHO : World Health Organisation
I thank the respondents for sacrificing their time to take part in the study and the research assistants for helping in the data collection.
Rita Tekpertey: Conceptualise the study, data curation, formal analysis, writing – review & editing, and methodology.
Anthony Edward Boakye: Writing – original draft, Software and proof reading
Ethical Approval
Ethical approval (with ID number UHAS-RCE A./10/111/21-22) to conduct the study was taken from the Research Ethics Committee of the University of Health and Allied Sciences, Ho, Ghana.
In the field, verbal consent was taken before a participant could take part in the study.
Consent to Publish
Participants were told that the study was strictly aca-demic and that the results would be published for the purposes of contributing to building academic literature.
Funding
The study was self-funded.
Data Availability Statement:The data is only available to the author hence it was a primary data.
Conflicts of Interest: The authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
