
Research Article | DOI: https://doi.org/10.31579/2578-8965/185
1 Tengandogo Teaching Hospital, Burkina Faso.
2 Yalgado Ouédraogo Teaching Hospital, Burkina Faso.
3 Bogodogo Teaching Hospital, Burkina Faso.
*Corresponding Author: Dantola Paul Kain, Joseph Ki-Zerbo University, 03 BP 7021 Ouagadougou 03, Burkina Faso.
Citation: Dantola P. Kain, Hyacinthe Zamané, Adama Ouattara, Assétou Zongo, Sibraogo Kiemtoré, et al, (2023), Factors Associated with Reaching the 6th Antenatal Care Contact within Toma Health District in Burkina Faso, J. Obstetrics Gynecology and Reproductive Sciences, 7(7) DOI:10.31579/2578-8965/185
Copyright: © 2023, Dantola Paul Kain. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 September 2023 | Accepted: 04 October 2023 | Published: 13 October 2023
Keywords: pregnant woman; 6 contacts; antenatal care; associated factors; toma
Background/Aim: The 6th contact is the end-of-pregnancy consultation at 36 weeks. This study aimed at determining the factors associated with reaching at least 6 antenatal care contacts within Toma health district.
Materials and Methods: This was a descriptive and analytical cross-sectional study involving 34 health facilities in Toma health district. It was carried out from December 01st , 2020 to November 30rd, 2022 with a prospective collection method. Only pregnant women monitored with the REC-Maternity application and who had given birth during the study period were included.
Results: The study included 7275 patients. Women were over 25 years in 57% of cases, and 67% of them lived between 0 and 4 km away from the health facility. The proportion of women who achieved at least 6 healthcare contacts was estimated at 8.7%. Logistic regression showed that the presence of a complaint (OR=2.8; P<0.001), the distance travelled between 0 and 4km (P<0.001), the fact of being accompanied (OR=1.33; P=0.021), the presence of means of transport (OR=1.6; P=0.015) had a positive and significant influence at a threshold of 5% on reaching at least 6 antenatal care contacts within Toma health district. On the other hand, having no educational level, being under 19 years, being unmarried (OR=0.7; P=0.032) and being late for ANC (OR=0.25; P<0.001) have a negative and significant influence at a threshold of 5% on reaching at least 6 antenatal care contacts in the district.
Conclusion: The frequency of 6 antenatal care contacts was relatively very low. Advice on the risk of discontinuity of antenatal care on the mother’s and newborn’s health is urgently needed within the district health facilities at every contact of the woman with the maternity ward.
Worl wide has 295,000 maternal deaths corresponding to 211 maternal deaths per 100,000 live births in 2017[1]. This maternal mortality rate is higher in developing countries than in developed ones. For example, in 2015, according to the World Health Organization (WHO) the maternal mortality ratio within developed countries is estimated at 12 per 100,000 live births against 239 per 100,000 live births within developing countries [2]
The maternal health situation in Burkina Faso is not satisfactory. Indeed, the country has had 320 deaths per 100,000 live births in 2017[3]. This figure is far from the Sustainable Development Goals (SDGs) estimated at 70 deaths per 100,000 live births. It is of paramount importance to focus on antenatal care in order to reduce as much as possible maternal and neonatal mortality.
In order to meet these sustainable development goals, WHO has developed some recommendations in 2016 in order to enhance antenatal care quality. Thus, 8 antenatal care contacts (ANC) are recommended instead of four consultations. The 6th contact is the end-of-pregnancy consultation at 36 weeks whose purpose is to establish the prognosis for delivery, such as examination of the maternal pelvis, fetal weight and presentation. This contact enables any observed abnormalities to be managed, and even a prophylactic caesarean section to be planned [4]. This 6th contact is of crucial importance in reducing maternal and neonatal mortality and morbidity.
However, the literature review on the determinants of the 6th antenatal care contact in Burkina Faso is almost lacking. The aim of the article was to investigate the factors associated with reaching the 6th antenatal care contact in order to enhance pregnant women’s access to antenatal care.
This was a descriptive study conducted in 34 health facilities within Toma health district of Burkina Faso. The sample was drawn from pregnant women in the Toma health district registered in the Rec-maternity electronic consultation database from November 2020 to July 2021.
To determine the factors associated with the 6th antenatal care contact, the sampling was exhaustive for all women received in antenatal care and who gave birth in one of the 34 health facilities within Toma district and who were registered in the REC-Maternity software (Electronical Maternity Consultation Register). This information comes from the action plan of the Toma health district for the year 2019.
The variables studied were related to socio-demographic characteristics, to clinical and health policies aspects.
The data collection consisted in extracting data from REC-Maternity which were sent to the server after tablets synchronization. Antenatal care data from November 2020 to July 2021 were extracted for analysis so to find women in our database who had at least reached 6 antenatal care contacts.
After data extraction, variables of interest were checked while some were coded. Data analysis was performed using Rstudio software version 4.0.3. As for qualitative variables, frequency was determined. The chi-square test as used to determine the association between the variable to be explained and the explanatory variables. The association between the two variables was deemed significant when p-value<0>
Ethical and deontological aspects were complied with when collecting data with Rec-Maternity.
A total of 4354 patients from 34 health facilities were included in the study. The prevalence of reaching the 6th antenatal care contact was estimated at 4%.
Patients were at least 25 years old in 59.6% of cases; 86.6% of them were married and 61.1% illiterate. 88.7% of cases were housewives and their spouses were farmers in 88.8% of cases. They were multiparous in 80% of cases and 63.5 % of them lived at less than 4 km away from the health facility.
The results of the individual association between reaching at least 6 antenatal care contacts and the independent qualitative variables of interest are presented in tables 1, 2 and 3.
Our study results show that there is an association between reaching of at least 6 antenatal care contact and the following factors: the educational level, the distance travelled, the means of transport, the financial savings, the presence of a companion, presence of complaints and history of a deceased newborn.
Educational level: in fact, women with a higher educational level are more likely to reach 6 antenatal care contacts (5%). Then come those with primary educational level (4.9%), secondary educational level (4.8%) and those who are literate (4.7%).
Distance travelled: women who live between 0 and 4 km away from the health facility are more likely to reach 6 antenatal care contacts (4.2%) than those who live between 5 and 9km (2.4%), and those living at more than 10km away (2.6%) from it.
Means of transport: women who have their own means of transport manage to reach at least 6 antenatal care contacts than those with no means of transport (4.3% against 1.2% respectively).
Financial savings: women who have financial savings and reach at least 6 antenatal care contacts outnumber 4 times those who have no financial savings with respectively (4% against 0.6%).
Patient’s companion: women who are accompanied are more likely to reach 6 antenatal care contacts (5.5%) than those who are not (3.3%).
Complaints: women with complaints were 3 times more likely to reach 6 antenatal care contacts than those with no complaints (12% against 3.1%).
History of a deceased newborn: Women who have lost children tend to better follow antenatal care.
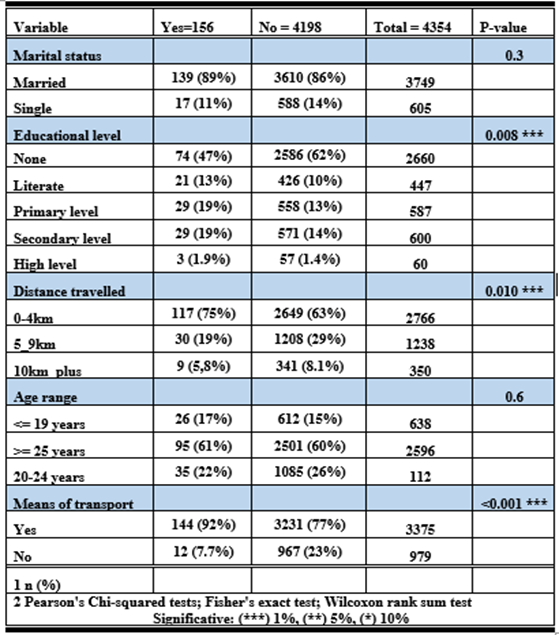
Table 1:Results of individual association between reaching at least 6 antenatal care contacts and independent variables
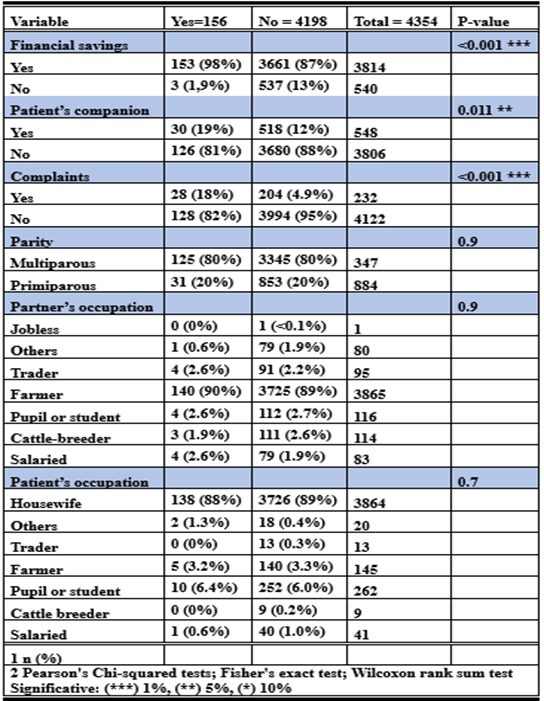
Table 2: Results of the individual association between reaching at least 6 antenatal care contacts and independent variables (continued)
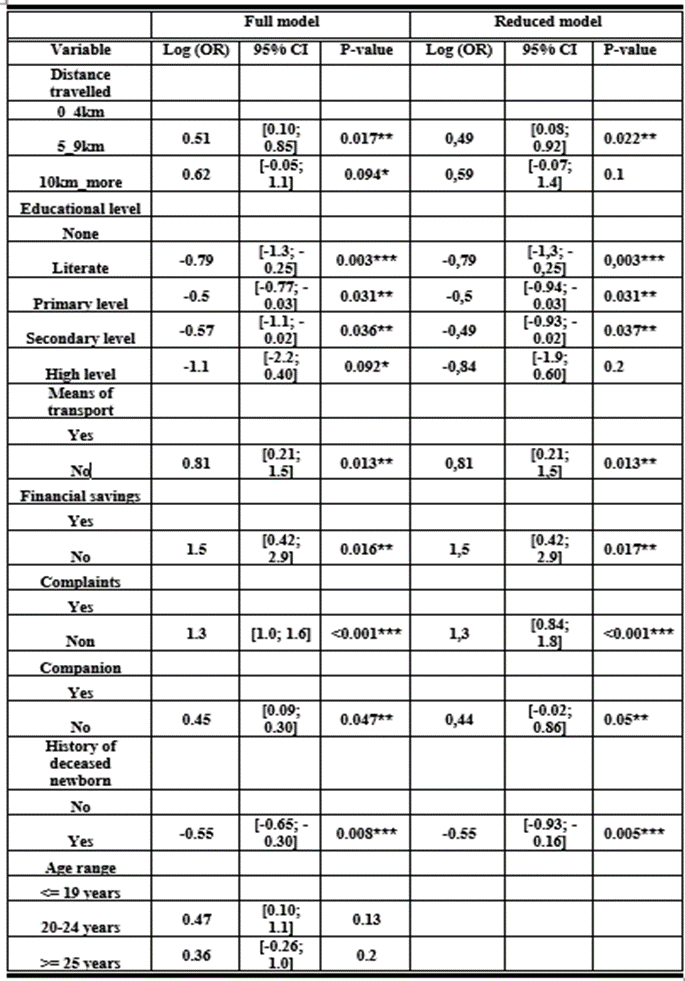
Table 3: Results of logistic regression between independent model variables and reaching at least 6 antenatal care contacts
NB: (*) significant at the threshold of 10%, (**) at the threshold of 5% et (***) at the threshold of 1%.
The distance travelled has a positive and significant influence on reaching 6 antenatal care contacts. The positive signs in both models mean that women who are at 0-4km away from the health facility are more likely to reach at least 6 antenatal care contacts than those who are at 5-9km and more than 10km away from the health facility. This may be due to poor road conditions. In low- and middle-income countries, poor roads and means of transport hamper access to antenatal care services [5]. Given women's multiple household chores, they lack some time to travel long distances for their antenatal care [6]. Furthermore, a study carried out in rural Burkina Faso showed that living at less than 5 km away from a health facility was positively associated with the use of antenatal care [7]. The distance to health facilities, which required uncomfortable travel on poor road networks, was identified as an obstacle [8].
Educational level: being literate is significantly associated (OR=-0.79; P=0.003) with reaching 6 antenatal care contacts. This could be explained by the fact that those who are literate are more likely to understand the importance of ANC, regardless of the language in which the counselling is given, than those who have no education at all. The translation of the counselling is often not obvious enough for the woman to understand exactly what the health worker is saying. The results corroborate those of a study conducted in Uganda, which indicated that girls with a low level of education have more difficulty in accessing prenatal care [9]. Studies in Guinea and India have shown that a woman's education influences her use of antenatal care [7, 10, 11].
Means of transport: having a means of transport has a significant influence on reaching at least 6 contacts (OR=0.81; P=0.013). This could be explained by the fact that the means of transport facilitate access to the health facility in a short time, so that they could return for their daily tasks. Indeed, in Uganda, transport is perceived as preventing some pregnant women from going to antenatal care [12]. Moreover, the lack of transport has an influence on antenatal care [13].
Financial savings: It has a positive and significant influence at a threshold of 5% (OR=1.5; P=0.016) on reaching the 6 antenatal care contacts. This could be explained by the fact that, despite free care in health facilities, other costs may arise from consultations, such as the cost of drugs, syringes and gloves in the event of stock-outs in health facilities' pharmaceutical depots. In addition, there are indirect costs such as the cost of transport, food and so on. Studies carried out in Kenya have shown that poverty is an obstacle to the use of MNCH services. Another study conducted in Guinea showed that women from the richest wealth quintile were more likely to use antenatal care. [13, 14].
Complaints: They have a positive and significant influence at a threshold of 1% on reaching 6 antenatal care contacts (OR=1.3; P<0>
Patient’s companion: the fact of being accompanied has a positive and significant influence at a threshold of 5% on reaching 6 antenatal care contacts in Toma district (OR=0.45; P=0.047). This result could be explained by the fact that in the provinces, women seek their husband’s or mother-in-law’s approval before coming for antenatal care. The study carried out in Uganda has showed that the lack of the husband ‘support, including difficulties in encouraging her to go for antenatal care, is an obstacle to the use of antenatal care [12]. Furthermore, women do not still have the power to decide for themselves about their care during pregnancy [11]. In some hierarchical societies, the decision to use antenatal care requires the authorization of the tribal elders, of the husband, the mother-in-law or eldest member of the family [5]. Furthermore, low autonomy and lack of the husband’ support have a negative impact on the overall use, timeline and frequency of antenatal care [15].
History of deceased newborn: This has an influence on reaching at least 6 antenatal care contacts (OR=-0.55; p 0.008). In fact, women who did not have an history of a deceased newborn were 55% less likely to achieve 6 antenatal care contacts than those who did. This could be explained by the fact that the shock of losing a newborn leads them to take care of their pregnancies so as not to go through the same experiences of losing their children.
This work has certain limitations. It resides in the data on the antenatal care form. The tablet may discharge, break down, etc. and the health worker would be using the register at this time. Which means that not all consultations are recorded in the maternity REC, this implies that there are women who will perhaps have at least 6 antenatal care contacts who will not be counted in the number of women having had at least 6 antenatal care contacts because was not recorded in the REC-maternity.
Antenatal care in Burkina Faso is of paramount importance although continuity of care is a major public health issue. This study has provided some basic findings enabling to understand the prevalence of 6 antenatal care contacts within Toma health district. The prevalence of reaching at least 6 antenatal care contacts is low. The factors significantly associated with reaching at least 6 antenatal care contacts within district are: the distance travelled, the educational level either primary, secondary or higher, literacy, presence of complaints, financial savings, patient’s companion, history of deceased newborn, having a means of transport.
The studies involving human participants were reviewed and approved by the authorization of the ethics committee. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Kain DP and Zamané H prepared the manuscript, Ouattara A collected the data, Zongo A and Kiemtoré S. analyzed the data, Ouédraogo A and Thiéba/Bonané B provided a useful review of this manuscript. All authors contributed to the article and approved the submitted version.
The authors would like to thank all patients for their consent obtained. The authors also thank all the staff who contributed to the care of the patients.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
