
Research article | DOI: https://doi.org/DOI:10.31579/2690-4861/247
D Amico Foundation for Renal Disease Research, Milan, Italy, Retired from Nephrology and Dialysis Unit, Azienda Ospedaliera Ospedale San Carlo Borromeo, Milan, Italy.
*Corresponding Author: Claudio Bazzi
Citation: C Bazzi. (2022). Factors affecting long-term remission in patients with FSGS and NS. International Journal of Clinical Case Reports and Reviews. 11(5)
Copyright: © 2022 Claudio Bazzi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 30 July 2022 | Accepted: 05 August 2022 | Published: 16 September 2022
Keywords: high blood pressure ; Nephrotic Syndrome; Cyclophosphamide
In FSGS with Nephrotic Syndrome (NS) 23 patients (61%) of 38 with functional outcome are in remission with very long follow up (from 60 to 331 months) after treatment with Steroids alone or in combination with Cyclophosphamide.
It would be interesting to assess whether in 11 patients with follow up from 5 to 27.6 years some parameters are associated with less severe disease favouring very long term remission.
Three parameters were considered [age<vs≥35 yrs, normal or high blood pressure (BP0 and BP1 ) baseline 24hP <vs≥ 6.5] to verify whether they assess lower disease severity favouring remission.
Age≥ vs <35 yrs and BP1 va BP0 are characterized by very significant differences of age, baseline and last eGFR, TID score and AH score. The patients with baseline 24hP < vs ≥6.5) were significantly different only for proteinuric parameters (TUP/C, IgG/C, Alb/C, α1m/C).
In all remission patients the last value of 24hP is not significantly different according to the considered parameters and is independent from the baseline values eGFR and TUP/C and duration of follow up
In the last years several studies evaluated which is the most favourable prognostic factor for long-term stable renal function and remission of proteinuria in Focal Segmental Glomerulosclerosis (FSGS) with nephrotic syndrome (NS) (1-15). In observational studies proteinuric biomarkers based on high molecular weight proteins excretion such as IgG and α2-macroglobulin showed a high predictive value for remission in patients treated with steroids and Cyclophosphamide. The functional outcomes in all patients treated with Steroids alone or in combination with Cyclophosphamide include remission, persistent NS (PNS) with normal renal function (NRF) or chronic renal failure (CRF), and progression to ESRD. The interesting aim of this study is to assess if the very long follow up of patients with remission (159±77, 60-331) may be dependent on clinical, functional, histologic and proteinuric markers associated with less severe disease favouring a very long follow up of remission
The patients cohort included in the study was not selected. The patients attending the Nephrology and Dialysis Unit of San Carlo Borromeo Hospital, Milan, Italy, between January 1992 and April 2006 with renal biopsy diagnosis of Focal Segmental Glomerulosclerosis (FSGS) were 46; at baseline 6 patients have persistent non-nephrotic proteinuria (<3>
Proteinuria was measured in 24 hour urine collection and second morning urine sample by the Coomassie blue method (modified with sodium-dodecyl-sulphate) and expressed as 24/hour proteinuria and protein creatinine/ratio (mg urinary protein/g urinary creatinine). Serum and urinary creatinine were measured enzymatically and expressed in mg/dL. Serum albumin and IgG and urinary IgG, α2-macroglobulin (α2m), Albumin and α1-microglobulin (α1m) were measured by immunonephelometry; urinary proteins were expressed as urinary protein/creatinine ratio (IgG/C, α2m/C, Alb/C, α1m/C). Estimated glomerular filtration rate (eGFR) was measured by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula (16). Three types of renal lesion that are markers of disease severity in any type of GN were evaluated: percentage of glomeruli with global glomerulosclerosis (GGS%); extent of tubulo-interstitial damage (TID) evaluated semi-quantitatively by a score: tubular atrophy, interstitial fibrosis and inflammatory cell infiltration graded 0, 1 or 2 if absent, focal or diffuse (TID global score: 0-6) and extent of Arteriolar Hyalinosis (AH) evaluated semiquantitatively by a score: 0, 1, 2, 3 if absent, focal, diffuse, diffuse with lumen reduction, respectively (AH global score 0-4).
Continuous variables are expressed as means±SD. Categorical variables are expressed as the number of patients (%). The differences of mean were determined by t-test; categorical variables by the chi-square test. All statistical analyses were performed using Stata 15.1 (StataCorp LP, TX, USA). Two-sided p<0>
In 38 patients with NS and functional outcome 23 patients (61%) developed remission: the remission patients with age <35 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed p =0.04), p =0.001) p=0.017); p =0.18); xss=removed xss=removed p=0.85); p=0.0001), p=0.04), p=0.0002) p=0.006) p=0.001); xss=removed>
In the 23 patients with remission the follow up is rather long (from 60 to 331 months); it would be interesting to assess whether the patients with very long follow (27.6 years) were characterized by clinical, functional, histologic and proteinuric markers less severe than in patients with lower follow up. The last value of 24hP is not significantly different according to the baseline markers of severity of disease (age, normal or high blood pressure, baseline 24hP) (Table 3). Thus no one factor has been identified as associated with the duration of follow up. Few patients after remission show recurrence of NS that was still responsive to the first treatment. It may be suggested that the patients characterized by markers associated with more severe disease (age, blood pressure, baseline 24hP) should be treated with higher dosage and longer duration of the treatment that developed the first remission.

Table 1.Clinical, functional, histologic and proteinuric parameters in patients with Focal Segmental Glomerulosclerosis (FSGS) with different outcome.
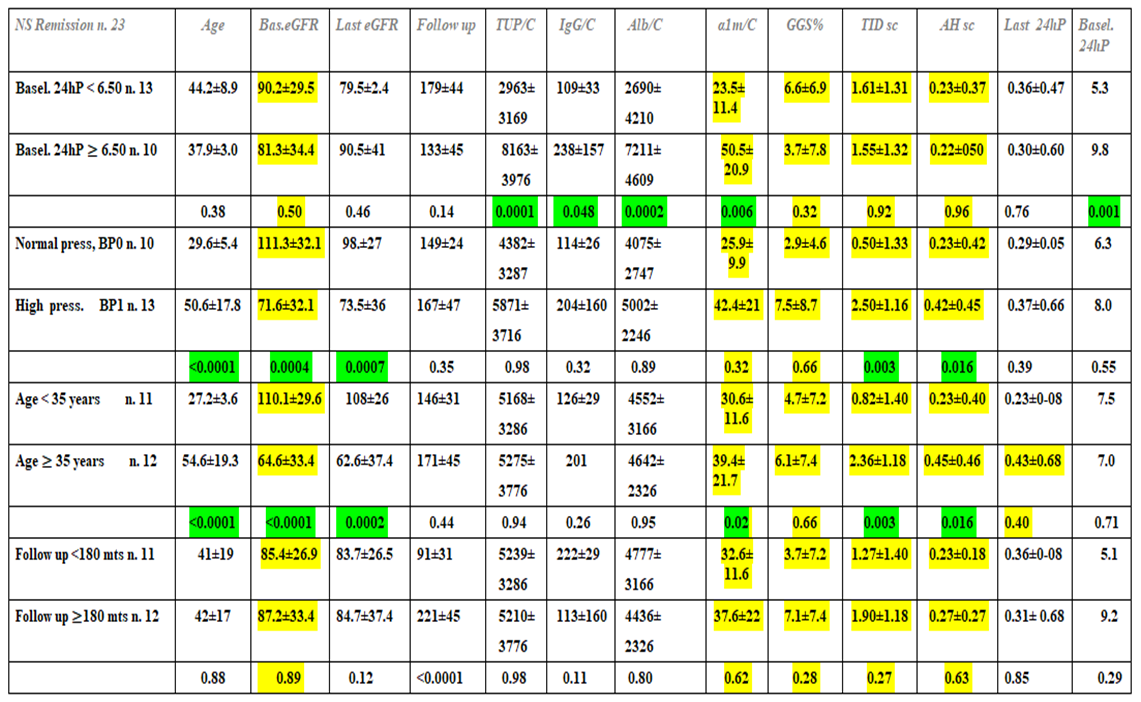
Table 2. Clinical, functional, histologic and proteimuric parameters in remission patients according to basel. 24hP, normal or high blood pressure (BP0 and BP1), age
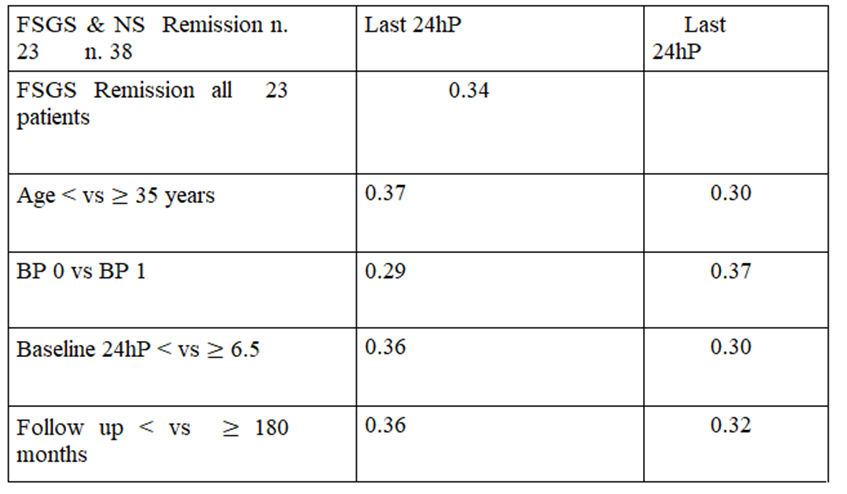
Table 3. Last value of 24hP in all 23 remission patients, in patients with age
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
