
Case Report | DOI: https://doi.org/10.31579/2690-4861/691
1 Department of Pediatrics, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China.
2 senior Department of Pediatrics, The Seventh Medical Center of PLA General Hospital, Beijing, China.
3 Department of Neonatology, Children’s Hospital of Chongqing Medical University, Chongqing, China.
*Corresponding Author: I. Bon, senior Department of Pediatrics, The Seventh Medical Center of PLA General Hospital, Beijing, China.
Citation: Li Wang, Lian Duan, Liuming Hang, Gang Liu, Lu Peng, et al, (2025), Facial Injury Caused by Punctiform Impact from High Pressure Gas, International Journal of Clinical Case Reports and Reviews, 23(4); DOI:10.31579/2690-4861/691
Copyright: © 2025, I. Bon. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2025 | Accepted: 12 February 2025 | Published: 21 February 2025
Keywords: high pressure; redness; facial injury; malocclusion
This case report is about a 12-year-old boy, his face, mouth and nose was damaged by gases from a high pressure gas gun (which can eject compressed gases with a pressure of 6-10 kpa from an air compression pump). Redness and swollen with small area of ulceration in the right cheek was earliest observed. Rapid deterioration from broken skin to extensive nose damage.
With the advent of high pressure compressed air in industrial work, the risk of associated pneumatic injuries from its improper use is becoming evident. These injuries usually happen through careless use and practical jokes, although rare but can be fatal. Previous reports are mainly about colorectal injury by compressed air passing through the anus, direct impact of high-pressure compressed air on human face is an unusual emergency presentation [1-5]. This report describes the case of facial injury caused by punctiform impact from high pressure gas.
Case Report
The face, mouth and nose of a boy aged 12 was damaged by gases from a high-pressure gas gun (which can eject compressed gases with a pressure of 6-10 kpa from an air compression pump). Redness and swollen with small area of ulceration in the right cheek was earliest observed. During the subsequent week, the skin ulceration and necrosis was progressively aggravated, and the nose and throat were gradually affected. The child was transferred to our hospital on the 12th day after injury to prevent further aggravation of facial ulceration.
Physical examinations at hospital admission found a 5 cm × 8 cm ulcer with parotid fistula in the right cheek and a 3 cm × 7 cm ulcer in the right preauricular area. A large number of necrotic tissues and purulent secretions were observed on the ulcer (Figure 1). The normal shape of nose disappeared with necrosis from biliteral nasal wings to nasal root. Nasal dorsum cartilage and nasal wing cartilage were necrosis and deficiency, with necrosis of anterior nasal septum cartilage and partial deficiency of the nasal columella. The bony structures of anterior segment of inferior nasal concha, nasal septum and turbinate were visible (Figure 2). The oral cavity was malodorous and the gingiva was dark-colored. The gingival laceration was present from upper right 5th to 7th teeth with bone exposure and a large number of secretions. The upper left first tooth was completely detached. The upper left 2th to 6th teeth suffered from mobility of grade II or III. The dentition was irregular with malocclusion. Slight mobility was present from the upper left 6th tooth to the left upper maxillary joint. The mucous membrane of the hard palate was dark black; A 2 cm × 1.5 cm perforation was present at the junction of soft palate and hard palate. Part of the soft palate was ulcerated (Figure 3). Cranial CT scanning was urgently performed and showed that necrosis was not diffused within the sinus and skull.

Figure 1: Right facial wounds

Figure 2: Nasal wounds

Figure 3: Injuries in the mouth
After continuous facial debridement for a week after hospital admission, the pediatric patient's condition was stabilized without continuous expansion of festered wound surface, and the child could be fed through a nasogastric tube. During the next 9 months, the necrotic part of the maxilla along the nasal and facial midline and necrotic tissues on the face detached gradually, scarring healing of the facial wounds was achieved (Figure 4). Reconstructive procedure was started after the stabilization of
the wound surface. Firstly, surgical repair was performed but failed to close the parotid fistula, which was gradually healed after 6 times of local radiotherapy. Bone deficiencies along the nasal and facial midline including the cover of the palate, alveolar processes and superior teeth were repaired with prostheses after CT three dimensional reconstructions (Figure 5). The total nasal reconstruction was performed by staging operations using expanded forehead flaps.

Figure 4: Scarring healing of the facial wounds was achieved, the soft palate disappeared with the oral cavity connected with outside space via opened nasal cavity.
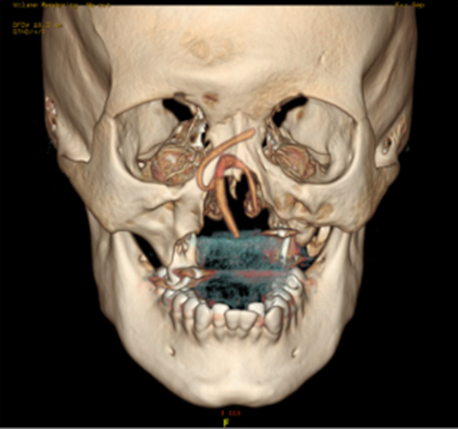
Figure 5: CT three dimensional reconstructions
Injuries caused by high-pressure gas is an unusual emergency presentation. Its clinical manifestation and pathological changes are different from those caused by traditional shock wave, direct punctiform impact on the skins from high-pressure gas produce impact forces far greater than the traditional strength of blast injuries [6-11]. There have been sporadic reports of pneumatic injury, most of which focus on pneumatic colon injury. At present, literatures about direct punctiform blast from high pressure gases on the skins of face or other parts were rare, and chronic persistent necrosis after injuries described in this case were also not reported previously.
In the course of treating this child with high-pressure compressed air blast injury, we found that his facial injury was different from that caused by other shock waves and blast injuries: he presented a concentric circle ulceration centered on the impact point, and the development of the injury was lagging behind, which was easily neglected in the early stage. The characteristics of this case were concluded as follows: firstly, late onset of symptoms: the facial skin tissues remained structurally intact during the initial stage after direct blast from the high-pressure gas, and the ulceration and necrosis occurred gradually. So, the skin redness, swollen and ulceration appeared in the early stage of disease were ignored, causing delay of related treatments. Secondly, rapid deterioration: there was only an interval of one week from skin rupture to large area necrosis of the nose. Such rapid aggravations of skin injuries without underlying diseases were rarely reported. Finally, slow healing: The facial and nasal damage achieved scarring healing more than half a year. The injuries of nasal bone and maxillary bone became basically stable after a longer time due to the osteolytic necroses.
In this case, we found that compared to the traditional shock wave, the impacted forces by high-pressure gases is greater and the duration is longer, the injury of skin will be worse.
The direct high-pressure gas blast injury is a kind of closed laceration with concussion injury. In this type of injury, the skin lesions appear relatively late, but the wound deteriorates more rapidly and more seriously with a longer healing time. Since these conditions are rarely observed in clinical practice and easily to be ignored, they may lead to serious consequences. In later stage of treatments, enhancing wound care to promote wound healing is the key point for successful treatments.
None of the authors have conflicts of interest to disclose.
None of the authors have financial relationships relevant to this article to disclose.
LW, LD, and ZF wrote the report. LW, LP and YS searched the literature and analysed the results. ZF, LD, LH and GL cared for the patient. LD provided the images. All authors critically revised the report. Written consent for publication was obtained from the patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
