
case report | DOI: https://doi.org/10.31579/2692-9392/141
1Department of Pathology the Ohio State University Wexner Medical Center, Columbus, OH Doan Hall.
2Vice Chair and Director, Anatomic Pathology, Department of Pathology Director, Digital Pathology Shared Resource the Ohio State University Wexner Medical Center, Columbus, OH.
*Corresponding Author: Nada Shaker, Department of Pathology the Ohio State University Wexner Medical Center, Columbus, OH Doan Hall.
Citation: Nada Shaker, and Anil Parwani, (2022) Extramammary Paget’s Disease Arising in the Scrotum of an Elderly Male. J. Archives of Medical Case Reports and Case Study, 6(3); DOI: 10.31579/2692-9392/141
Copyright: © 2022 Nada Shaker, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 August 2022 | Accepted: 25 August 2022 | Published: 09 September 2022
Keywords: extramammary paget’s disease; angiolymphatic
Extramammary Paget’s disease (EMPD) is a rare form of primary or secondary intraepithelial adenocarcinoma typically presenting within the fifth through seventh decades of life. Though cases of EMPD localized to the scrotum are typically not associated with underlying malignancy, evaluation of dermal and angiolymphatic invasion in conjunction with pertinent laboratory investigations, e.g., serum CEA, is essential to rule out malignancy and metastatic disease. We present a case of EMPD in an elderly male that presented with a history of a longstanding asymptomatic scrotal lesion that was ultimately managed with excision and skin grafting.
Extramammary Paget’s disease (EMPD) of the scrotum is a rare occurrence, most often presenting during the 6th or 7th decade of life. Local recurrence is common in EMPD, with approximately 22% of cases demonstrating resurgence in the penoscrotal area. 1 We discuss a clinical presentation of a case of EMPD in a patient initially presented with a pruritic, non-healing erythematous scrotal lesion of the scrotum for more than five years.
Case Presentation:
A 76-year-old male with a past medical history of atrial fibrillation, colitis, postoperative hypothyroidism, and aortic stenosis with prior admittance due to hematuria and other lower urinary tract symptoms presented to our center for evaluation of a scrotal lesion. He denied any ongoing hematuria, dysuria, frequency, difficulty urinating, chills, fatigue, fever, abdominal pain, or additional skin lesions. The patient described the lesion as an asymptomatic “red spot,” present for at least 5 years, which became pruritic 1 year before his presentation. At the onset of pruritis, the patient was treated with antifungal creams by his primary care provider yielding no improvement in symptoms. Dermatology referral and subsequent biopsy of the lesion resulted in pathologic findings which prompted a urological consult.
A physical exam revealed a scaly and erythematous left lateral anterior scrotal lesion (3.2cm x 2.0 cm). Figure 1. Testes were bilaterally descended and without masses or nodules. No groin lymphadenopathy was noticed. A left hemi-scrotum excision with scrotoplasty and a split-thickness skin graft was performed. Intraoperative consultation confirmed that the margins were appropriate. On gross examination, the specimen was consistent with a geographical portion of tan, hair-bearing skin that measured 7.3 x 5.5 x 1.1 cm. The epidermal surface featured a tan-white, mottled lesion measuring 3.2 x 2.3 x 1.1 cm. Sections cut through the lesion revealed tan-white, rubbery tissue 0.1 cm in maximum thickness and 0.9 cm from the deep margin, from which a focus of orange discoloration measuring 0.2 cm in thickness was also noted. Microscopy revealed large pale cells with enlarged hyperchromatic nuclei arranged in nests and single cells throughout all layers of the epidermis. Nuclei were pleomorphic with basophilic nucleoli. These atypical cells were confined to the epidermis, with no signs of invasion into the dermis. The epidermis was acanthus with foci of parakeratosis. The dermis appeared edematous with lymphoplasmacytic infiltrates. Figure 2. Ancillary testing was positive for CK7, CEA, and Mucicarmine staining with negativity to S-100 staining. Figure 3, 4.

Figure 1: Physical examination of the scrotum: A 3.2 x 2.0 cm non-healing erythematous scrotal lesion.
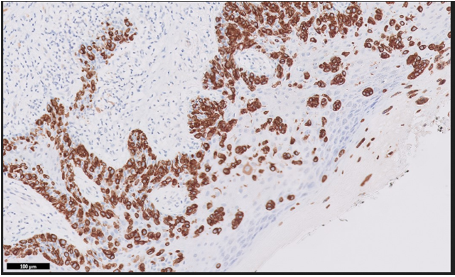
Figure 2: Pathological findings: The tumor is composed of malignant cells in the epidermis with local glandular differentiation nests, (hematoxylin and eosin, original magnification x50).

Figure 3: Immunohistochemical staining for ck7 (original magnification x100): The tumor cells are positive for CK7

Figure 4: Immunohistochemical staining for CEA (original magnification x100): The tumor cells are positive for CEA
Extramammary Paget’s Disease (EMPD) arises from the glandular differentiation of carcinomatous cells within the epidermis. The most common sites of EMPD in women are the labia majora and perianal region [2,3]. Men most commonly develop the disease in the scrotum or perianal region [3]. Several reports described rare cases in the genitourinary tract [4,5,6]. EMPD has an insidious onset, characteristically manifesting as a scaly, erythematous plaque, which may evolve into a nodule or ulcerate. Localized pruritus most commonly accompanies the area surrounding this lesion, though some have described the lesion to be painful rather than pruritic [2]. The pathogenesis of EMPD is still unclear, with current categorizations relegated to primary or secondary disease [7]. Primary disease, representing most cases of EMPD, results from an in-situ neoplasm originating from the intraepidermal sweat duct. Secondary EMPD develops in association with an underlying carcinoma (bladder, cervix, prostate, urethra, or rectum) with epidermotropic metastases [2]. Treatment for EMPD, regardless of location, is generally with wide surgical excision and appropriate margins [8,9].
Microscopically, both Paget Disease and EMPD are characterized by an intraepidermal expansion of atypical large cells with large nuclei [10]. These cells characteristically have a pale vacuolated cytoplasm and vesicular nuclei. The epidermis itself is typically hyperkeratotic with parakeratosis and acanthosis. Paget cells contain much-polysaccharides that stain positive for PAS, mucicarmine, and alcian blue. CEA and CK7 immunohistochemistry stains are positive in EMPD, which is typically negative for CK20, S-100, and Melan-A [1].
Differential diagnosis of EMPD includes melanoma, which may be distinguished from EMPD by positive staining for Melan-A and S-100 and negativity for CEA [1]. In addition, the revolution of digital pathology made disease diagnosis more efficient, and the advancement of AI became more applicable [11,12,13]. Pagetoid dyskeratosis, an incidental pathological finding appearing in several skin conditions, may be differentiated from EMPD by its absence of cell atypia along with negative staining for mucopolysaccharide and CEA [14]. EMPD lesions may bear a similar appearance to those of Bowen’s disease, which stains negative for CEA and S-100. CK7 staining is variable in Bowen’s disease, with most cases staining negatively, though two cases of CK7 positive Bowen’s disease have been reported [1].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
