
Review Article | DOI: https://doi.org/10.31579/2688-7517/008
Mother Theresa College of pharmacy, India.
*Corresponding Author: Thadakala Kiran, Mother Theresa College of pharmacy, India
Citation: Thadakala Kiran (2019). External evidence against using less-than complete abstinence as a primary outcome in addiction. Addiction Research and Adolescent Behaviour 2(2): Doi: 10.31579/2688-7517/008
Copyright: © 2019 Thadakala Kiran. This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 May 2019 | Accepted: 31 May 2021 | Published: 16 June 2019
Keywords: addiction; vivitrol; substance abuse
“Addiction” is a complex neurobiological process of hedonic dysregulation. It is characterized in humans by compulsive use of substances, loss of control over the quantity consumed, and continued use despite the harm caused by the substance. Addicted individuals are prone to relapse that appears to be related to reexposure to the addicting substances, substance-related cues, and psychosocial stressors [1]. In this process, initial impulsivity is replaced by compulsivity [1]. The traditional method of treatment for addiction in the United States involves twenty-eight days of residential treatment. The follow-up recommendations by treatment centers generally amount to participation in twelve-step meetings. There is little financial incentive for rigorous follow-up in this model and the recovery rates following such treatments are unknown. Even if very generous definitions of success are applied, recovery rates remain low. However, for physicians, well-documented recovery rates following their initial residential treatment experience are high. Additionally, there is a movement in the field of addiction medicine to employ “Medication Assisted Treatment” (MAT). For example, its advocates recommend the use of medications such as naltrexone (Vivitrol®).The proponents of these medications, however, use curious outcome measures, rather than complete abstinence, to demonstrate their efficacy. This paper reviews and utilizes the neurobiology of addiction to compare and contrast the outcomes in different populations. It also reviews the outcome data on Vivitrol in particular. We believe that a clear understanding of the neurobiology of addiction is essential to understanding and correcting the vast outcome differences in various patient groups.
The neurobiology of addiction is complex. Acute effects of substances of abuse include intoxication and dependence. These phenomena are well understood. What is complex and comparatively poorly understood is what happens over the course of time in an addicted brain and why so many people relapse. A brief review the brain’s reward system is in order to gain an understanding of the phenomenon of relapse.
The human reward system which is primarily located in the older, less evolved, “reptilian brain”, was designed to ensure survival. Based on evolutionary biology, the brain’s primary mandate is survival and propagation of the species. The reward system is evolutionarily ancient but is exceedingly important to the organism to fulfill this mandate. Pleasurable activities ensure survival of the organism and the propagation of the species. Such reward systems involve dopamine (and other chemicals derived from tyrosine). They are present in even very primitive organisms across many phyla. These include phyla such as Nematoda, Platyhelminthes, and Mollusca [2]. The centerpiece of this reward system in humans is the dopamine release in the nucleus accumbens (NAc). This release occurs as a result of the exposure to the addicting drugs and other pleasurable activities, such as food and sex.
Substances of addiction primarily recruit this reward system to make the organism initially feel good. As substance ingestion continues, dysphoria and negative emotional consequences ensue, resulting in severe psychosocial disruption [3,4]. Substances, then, are consumed out of the biological necessity created by chemical and structural adaptations in the reward system. The system increasingly becomes dysregulated, and out-of-control manifestations occur. The neural adaptation from chronic drug-taking dampens the perception of the reward (pleasure) and markedly increases craving and locomotion of the animal. This behavior is magnified with decreasing higher cortical/prefrontal brakes to stop this downward spiral.
Hypothalamic Pituitary Axis (HPA) is activated by stress. This system is intimately involved in the development of addiction. Genetic factors influence the initial drug taking drive [5]. Chemicals generated in the hedonic systems of the brain may be initially deficient in a genetically susceptible host brain. Genetically susceptible individuals perhaps feel dysphoria even before using substances of abuse. Initially, these substances temporarily normalize the system; however, the vicious cycle of the downward spiral begins, further dysregulating the hedonic systems.
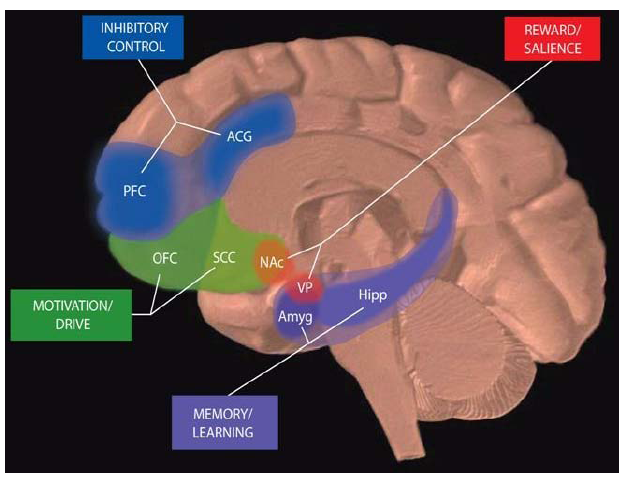
The areas of the brain involved in the reward system (Figure 1) includes Nucleus Accumbens (NAc), Ventral Pallidum or Ventral Tegmental Area (VP), Amygdala (Amyg), Hippocampus (Hipp), Subcallosal Cortex (SCC), Orbitofrontal Cortex (OFC), Prefrontal Cortex(PFC), and the Anterior Cingulate Gyrus (ACG). These reward pathways are present in rats, mice, and primates. Since no animal model of “addiction” per se has been reported, it is not possible to diagnose “addiction” in animals. The well recognized diagnostic criteria for addiction in humans include 1) Compulsion to use the substance 2) Loss of control over the quantity consumed 3) Continued use despite the harm caused by the substance. Obviously, it is not possible to fulfill all these criteria of “addiction” in laboratory animals. We can, however, study comparable traits that suggest addiction, such as alcohol preference in laboratory animals. Some these traits suggest comparable relapse behaviors is humans.
There is compelling evidence for the role of dopamine in a mesocorticolimbic reward system [6,7]. In addition to dopamine, many chemicals have been involved in the acute reinforcing/rewarding effects of addictive drugs. They include opioid peptides, gamma-aminobutyric acid (GABA) and endocannabinoids [1]. Dopamine is activated by cocaine, amphetamine and nicotine in the NAc. Cocaine and amphetamines are well-known sympathomimetics, and the role of dopamine with these two abusable drugs is easy to understand. But even in drugs of abuse that activate the system of opioid peptides, endocannabinoids, and GABA, mesolimbic dopamine release is important to produce the reinforcing effects of these drugs [8]. For example, animals placed in a lever pressing operant conditioning paradigm eventually will readily self-administer reward- producing drugs to include cocaine, heroin, and amphetamines. In time “addictive behaviors” will develop and include drug- taking at the exclusion of food and water. Animals will receive electric shocks to receive the drug. The animals will die due to exhaustion and hunger in pursuit of the drug [9,10].
The amygdala determines if the experience is pleasurable or painful and whether it may be repeated or avoided. The hippocampus records the memories of euphoria such as where, when, and with whom it occurred [6]. It is possible in laboratory animals, therefore, to have cue-dependent delivery of addicting substances. The frontal cortex coordinates the information and decides whether to engage in a behavior of drug taking. Frontal regions of the brain can act as a brake to the compulsive drug taking that is induced by the release of dopamine in the nucleus accumbens. In chronic drug administration such as cocaine, it has been shown that these drugs damage the prefrontal cortex, thereby removing the brake that would suppress compulsive drug taking [11]. In fact, neuroimaging studies such fMRI, and FDG PET has revealed an emerging pattern of generalized PFC dysfunction in drug-addicted individuals. This results in weakened “prefrontal brakes” to prevent relapse [12].
The pathway from the ventral tegmental area (VTA) to the nucleus accumbens determines how rewarding the activity is. Despite their targets, many drugs of abuse share the same final pathway of dopamine release in the nucleus accumbens and dopamine mimicking signals. Cocaine blocks the transporter protein on the cells to the ventral tegmental area neuronal circuits. This results in excess dopamine in the nucleus accumbens. Opioids suppress neurons that are normally responsible for dampening dopamine-producing neurons that project on to the nucleus accumbens. Opioid peptides can also act directly on the nucleus accumbens by releasing dopamine [13]. As the drug use progresses, high concentrations of dopamine in the nucleus accumbens increases production of cyclic adenosine monophosphate (cAMP), cAMP in turn activates the cyclic AMP response element binding protein (CREB). CREB down-regulates the reward pathways. The endogenous opioid peptide dynorphin is activated by CREB. Dynorphin shuts down the production of dopamine by pathways that go back from NAc to the ventral tegmental area. Release of dynorphin produces a net reduction in dopamine and acute tolerance to the drug ensues. This causes the drug addict to increase the dose and the frequency of drug use but despite that the drug produces a less euphoric effect [6]. CREB is a short-lived transcription factor, and the production of CREB stops after a few days of discontinuation of addicting substance. The production of CREB, decreases in a few days after drug use declines thereby causing a decrease in tolerance and a corresponding increase in the drug sensitivity. This produces the phenomena of craving [14,15]. This craving is intimately related to the now strengthened pathways between the amygdala, hippocampus, and nucleus accumbens. These strengthened pathways result in cravings that are triggered by mere memories of places, sounds, smells, and tastes associated with previous drug exposure, this mechanism is called cue-induced relapse. Even without the cues, memories of previous drug use can create a phenomenon of craving. These pathways are mediated by glutamate. Furthermore, dopamine release in nucleus accumbens sensitizes VTA and NAc for days [6]. The pathways between the prefrontal cortex and NAc are weakened with repeated drug use. Animal studies and limited human imaging studies suggest cocaine users display impairments in executive functioning. The evidence from the imaging studies pointed to the dysregulation in the medial and ventromedial prefrontal cortex, areas activated during performance and inhibition tasks. Additionally, cocaine abusers were deficient in other areas of executive functioning to include updating and shifting of mental sets and decision-making. These changes were marked by alterations in prefrontal activation [16]. This results in the removal of “brakes” that are normally present and compulsive drug use sets in.
CREB alone does not last in the brain long enough to cause a relapse. There is another molecule Delta-FosB, a transcription factor, which is produced in the NAc [17]. It may be responsible for relapse in addicted individuals. Animal studies suggest that, in response to chronic drug abuse, Delta-FosB concentrations rise in nucleus accumbens and the extended limbic system, and possibly in the prefrontal cortex. The transcription factor Delta-FosB is exceedingly stable and can remain in the NAc for weeks after a bout of drug use. The presence of Delta-FosB causes sensitization to the effects of the drug and makes animals highly prone to relapse. It is interesting to note that the other rewarding stimuli such as intravenous sucrose load or an excessive wheel turning in animals also produces Delta-FosB. This may be the mechanism responsible for the transfer of addictions in humans. After weeks of discontinued drug use, the Delta-FosB concentrations go down; however, sensitization to the effect of the drug and a tendency to relapse persists for months if not years. This may be due to structural changes that occur in the spiny neuron dendrites by the production of more sprouts. The structural change or plasticity that occurs after chronic drug use has been attributed to elevated concentrations of nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF). This occurs primarily in the in nucleus accumbens as a result of the release of Delta-FosB [16]. It is unknown when these dendritic arborizations reverse if ever. These plastic changes in the brain of an addict set the stage for a full-blown relapse when an addicting substance is introduced into this system. The potent opposing force for relapse seems to be the “brakes” applied to the craving for a substance by the frontal lobe executive systems. Thus, contingency contracting with the threat of severe consequence is a powerful motivator to prevent the use of an addicting substance in the first place. Interestingly, genetic or viral overexpression of Delta JunD antagonizes Delta FosB [18]. In the future a better understanding of the JunD system may lead us to develop novel treatment modalities for addiction.
Glutamate pathways are activated by increasing concentrations of dopamine in NAc from VTA neurons. As a result, pleasurable memories of drug-seeking experiences are laid down in the amygdala after the hippocampus assigns a high degree of salience to such behaviors [19]. In studies based on observations of drug addicts, it is apparent that stress is a potent inducer of relapse [20]. Chronic drug use produces plastic changes in hypothalamic-pituitary-adrenal (HPA) axis and corticotropin-releasing factor (CRF). Even in the acute drug withdrawal state, there is increased activity of CRF in the HPA and the extended limbic system. This in turn causes the release of dynorphin that in turn dampens the release of dopamine in the nucleus accumbens from VTA neurons. Antagonists to CRF have been shown to reduce excessive drug self-administration in animals. This particular HPA axis and CRF pathway have been termed as an “anti-reward pathway” [21]. Interestingly, chronic stress causes dopamine release in the nucleus accumbens; this sensitizes the reward system causing the subject to relapse. There have been studies where chronic stress has been shown to reduce the number of dopamine receptors [22], this may lead to anhedonia. There are studies that suggest that the sensitization can persist after the stress has been abated.
Understanding what causes a relapse in a subject who has remained abstinent for a period is the Holy Grail in addiction treatment. Subjects report high motivation to stay abstinent when they are interviewed in treatment. However, the relapse rates remain high. While addiction cannot be diagnosed in animals, there are certain behavioral traits in the laboratory animals such as mice, rats, and sub-human primates that guide us in that direction. Understanding the biological basis of relapse is very important in treating addicts. Laboratories use the “reinstatement model” to study factors that underlie relapse induced by exposure to self-administered drug abuse and stressors [9]. In studies, reinstatement typically refers to the resumption of extinguished lever pressing behavior after noncontingent exposure to the drug or non-drug stimuli. In cue-induced reinstatement, the resumption of drug-seeking occurs after exposure to the drug cues following extinction of the lever-pressing behavior. In the reinstatement model, the animals are trained to self-administer drugs by pressing a lever for intravenous drug infusion in an operant conditioning chamber. Eventually, the drug reinforced behavior is extinguished by substituting the drug solutions with saline or by disconnecting the infusion pump. The re-exposure to the drug results in the reemergence of addictive behaviors. The key to the primary conclusions in this paper is the research reported on priming induced drug reinstatement.
Numerous studies have reported heroin and cocaine-induced reinstatement [23]. The priming effect was also reported in alcohol and nicotine trained rats. Agents from the same pharmacological class self-administered drugs reliably reinstate heroin and cocaine. Several studies, however, also demonstrated “cross reinstatement with drugs that are from different classes than the self-administered drug” [24]. The role of several other neurotransmitter systems in reinstatement induced by cocaine and heroin priming is noted. These include 5-hydroxytryptamine, corticosterone, CRF, GABA, noradrenaline, acetylcholine and endocannabinoids. Even a small amount of a drug can induce relapse behavior in animals. A review of both animal and human research suggested that the resumption of drug taking remained problematic even when drugs were unavailable for extended periods or when the individual was successful in discontinuing use. Three powerful triggers for relapse include reexposure to drugs, drug-related stimuli, and stressors [25]. This research suggests that even a small amount of reexposure to the drug can produce a relapse and resumption to uncontrolled craving and drug use.
If addiction to substances lends itself elegantly to the simple outcome concept of complete abstinence from substances, why are there apparent complex methodological challenges in determining “success rate” following traditional 28 days of treatment? Perhaps it is because of the low clinical reliability inherent in self-report “follow up” interviews of these patients. Calling a patient on the phone to ascertain if they have remained sober since treatment is a recipe for an inaccurate data set. The question then becomes: why not include state of the art tissue sample monitoring such as hair, nails and urine for demonstration of substances as a sign of treatment failure or a relapse.
The DATOS study was designed to examine treatment outcomes for drug addicts. The large $27 million dollar MATCH study was designed to ascertain the effects of treatment on alcoholism. These studies have inherent flaws in their outcome measures [26,27]. This lack of research rigor makes finding the recovery rates of complete abstinence in these studies exceedingly difficult due to the problem of inadequate random tissue sample monitoring after treatment.
The DATOS study sponsored by NIDA analyzed results over a one and five-year time frame. The DATOS study incorporated four different outpatient treatment models: 1) methadone maintenance 2) long-term residential treatment 3) outpatient drug-free treatment 4) short-term inpatient treatment. They attempted to measure success by looking at the drop in the number of weekly cocaine users, the number of weekly marijuana users, decline in heavy drinking, changes in unemployment status, suicidal ideation, and illegal activity. Unfortunately, their data did not include complete abstinence as an outcome measure. Also, none of these studies included frequent and random tissue sample (urine, hair, and nails) monitoring to determine complete abstinence.
Miller, the principle investigator, led an eight-year, $27 million MATCH study, sponsored by NIAAA. Miller et al. [28] reviewed the MATCH, VA, and seven other studies and found a 25% rate of success over the course of one year. In these studies, abstinence is often based on self-report and occasional tissue monitoring. Furthermore, it only included alcohol. Unfortunately, self-report is a highly suspect measure, as denial and rationalization are hallmarks of addiction. Even this modest outcome percentage is vigorously challenged by Fishbain et al [29,30]. These studies as well as the recent development of Medication Assisted Treatment (MAT) proponents use other curious outcome measures instead of complete abstinence as outlined above [31].
Vivitrol is approved for the treatment of opioid and alcohol addiction. The outcome measure for opioid addiction was based on an “Opioid-Free Urine Response Profile”. The methodology required that urine opioid screens were performed weekly during Part A of Study ALK21-013 [32]. Therefore, each patient had 20 occasions to submit a urine sample during weeks 5 to 24. Urine samples were collected under direct observation by study site personnel. A patient with 20 opioid-free urine samples was scored with a frequency of 100%. A patient with 19 opioid-free urine samples would have a frequency of 95%, etc. For each treatment group, the response profile was generated by calculating the cumulative percent of patients at each observed value of the rate of opioid-free drug tests (≥ 0%, ≥ 5%, ≥ 10%, ≥ 15%… ≥ 95%, = 100%). The Vivitrol, website rated efficacy according to the following criteria: 1) had significantly more days of complete abstinence 2) stayed in treatment longer 3) reported less craving 4) were less likely to relapse to physical dependence. For use in alcohol addiction, Vivitrol’s efficacy is based on outcome measures of “event rate of heavy drinking” defined as the number of heavy drinking days per month based on > 4 drinks for women and > 5 drinks for men. The Vivitrol website equates a successful outcome measure as having “had significantly fewer heavy drinking days.” [33]. These studies for Vivitrol are short term studies, twenty weeks for opioids and six months for alcohol. There is not a single long-term Vivitrol® study that demonstrates success when complete abstinence is used as a gauge of recovery. These outcome measures with Vivitrol® are similar to outcomes in chronic disease models such as hypertension and diabetes. In doing so, they attempt to draw equivalency between addiction and other chronic diseases such as diabetes, and hypertension [34]. While these outcome measures are reasonable in a chronic disease model, we advocate that the primary outcome for addiction be total abstinence from addictive substances. The underlying neurobiology of the disease of addiction points to complete abstinence as a prerequisite for recovery. An addiction-prone central nervous system due to previous exposure to substances of addiction quickly reverts to a very dysregulated, dysfunctional, and dyshedonic state. This results in complete loss of control over the drug taking, with devastating psychological and social consequences to the addict. All outcome measures that are less-than-complete abstinence are not logical based on current understanding of the neurobiology and the clinical presentation of the disease of addiction. The other two medications utilized by MAT advocates are methadone and buprenorphine. These substances are reinforcing and agonists. We feel that the use of these substances in addicted populations is simply the reintroduction of a reinforcing drug and hence not addressed in this paper.
We believe that there is no problem in having other outcome measures in addiction as proposed by Tiffany et al. They suggest using the following five primary outcome measures: 1) change in self-efficacy 2) psychosocial functioning 3) network support/social support 4) craving 5) quality of life [35]. We, however, believe that these must be secondary outcome measures. While it is laudable to reduce the adverse impact of the disease of addiction on the patient and society, the very nature of the neurobiology of this disease mandates that we have to use complete abstinence as a primary outcome measure.
The European College of Neuropsychopharmacology consensus meeting was convened to develop guidelines for the investigation of treatment efficacy in substance use disorders. A publication by Van Den Brink et al. [36] discusses various outcome measures. They concluded improved methodology of potential treatments for substance addiction should assess outcome measures that include full recovery (cure) or drug use stabilization and harm reduction (care).
Additionally, complicating the interpretation of general outpatient success rates, are the methods often utilized by for-profit treatment centers to gather such information. Miller et al. [37] offer eight general points in their tongue-in-cheek article on how to have a high success rate in treatment: 1) choose only good prognosis cases to evaluate 2) keep follow-up periods as short as possible 3) avoid control and comparison groups 4) choose measures carefully 5) focus only on alcohol outcomes 6) use liberal definitions of success 7) rely solely upon self-report and 8) always declare victory regardless of the findings. The obvious conclusion is the lack of reliable data from for-profit treatment centers and the need to review their claims with healthy skepticism.
The recovery rates of addiction with traditional 28 to30-day treatment are so low that there has been a flurry of articles in the lay press. Even the headlines of these articles are illuminating. They include “The 30-day Myth” in the LA times, and in the Washington Post,” We’re addicted to rehab, It doesn’t even work.” [38,39].
In contrast, physicians in the USA enjoy a high success rate. Following residential treatment physicians enter into very rigorous monitoring programs coupled with contingency contracting and loss of licensure if a chemical relapse occurs. The monitoring includes attending a prescribed number of 12-Step meetings as well as random and frequent tissue sample analysis of urine, blood, and nails. State of the art analysis of tissue sample monitoring is the key to the success of the program. Urine samples have been the preferred specimen type for drug screening due to its low cost, the moderate window of detection, and the vast array of drugs detectable in urine. Advances in toxicology testing have progressed quickly, and now many drugs of abuse can also be tested for by using specimen types such as hair, nail, blood, and oral fluids. Often referred to as specialty tests, drug screens using hair and nail specimens have the greatest window of detection, typically three months and longer. These tests cover the common drugs of abuse and drug classes including expanded amphetamines, opiates, benzodiazepines, as well as many popular stimulants and prescriptions. Blood tests have been more limited but recently have gained more acceptances with the introduction of Phosphatidylethanol (PEth) testing. PEth is formed in the in the presence of ethanol and is widely viewed as the new marker for ethanol abuse. Oral fluid testing is catching up quickly in terms of lower costs and a vast number of drugs that can be detected. The collection process for hair, nail, blood, and oral fluids has a major advantage over urine collections. They each, by the nature of the specimen type, are collected in an “observed” method. This makes it difficult for the donor to adulterate their specimen. Urine collections may also be “observed” but are more difficult to coordinate and can be an uncomfortable experience for the donor.
State of the art tissue sample monitoring protocols has existed for physicians due to the significant public health risk if their relapse is not quickly recognized. These programs use random urine drug screenings, and in the first year perform up to fifty-two comprehensive and random urine drug screens in order to compensate for physicians who may misuse their knowledge of pharmacology in an attempt to evade detection of substances of abuse.
Additionally, hair analysis and nail analysis are sprinkled in with the urine monitoring to detect ultra-short acting substances such as fentanyl. The outcome data from these programs are carefully reviewed by the state medical boards whose mandate is to protect the public [40,41]. Recovery rates of complete abstinence from substances of addiction in physicians are at around 80%. This is remarkable given that this is a chronic disease and is very prone to relapse [42,43,44]. The data published is for five years, and complete abstinence from all substances of abuse is the outcome measured. These results suggest that monitoring is the key to increasing recovery rates.
Monitoring, however, is not recovery. Monitoring promotes recovery. Recovery and resultant psychic and spiritual changes occur with 12-Step programs. Contingency contracts with monitoring require participation in a 12-Step recovery program initially, but as the time passes, external controls are needed less and less, and the physicians develop internal psychological and spiritual coping mechanisms. These post-treatment monitoring effects were even seen in the MATCH study. One of the most interesting findings from Project MATCH was that even brief research contact over the telephone appeared to support abstinence. It is interesting that nearly all physician monitoring programs across the USA require 12-Step meeting attendance. None mandate the use of Vivitrol. Furthermore, all discourage the use of other MATs such as buprenorphine and methadone.
It is ethically problematic to have high success rates in a certain group of population such as physicians but underutilize these modalities in the general population. We are using less than optimum outcome measures as a barometer of recovery from addictive substances. Just as physicians are subjected to the strict monitoring program, the same principles of monitoring could be utilized for patients entering traditional 28-day treatment programs. The threat of suspension or revocation of a medical license and loss of livelihood and prestige is the deterrent for the physician. We suggest considering the use of similar contingency contracting in other employed patients who enter traditional 28-day treatment programs. After discharge, that patient’s ongoing job security may be tied to having a negative random tissue sample monitoring screen for a period of two to five years. In order for that to happen, a paradigm shift in the treatment industry has to occur. Emphasis needs to be placed on long-term monitoring with mandated attendance at meetings and reliable random tissue sample monitoring. If the disease of addiction has progressed to the point that patients have “nothing to lose”, then perhaps harm reduction strategies as secondary measures could be utilized as the next best thing. However, they should not be used as the primary outcome measure in addictions.
Chronic disease models such as hypertension and diabetes have been proposed for addiction, and we find this clinically problematic [34]. These diseases share a common theme with addictive diseases in that they are chronic, relapsing and fatal. However, the similarity stops there. Failure to take medications for high blood pressure or diabetes for a few days does not cause a dramatic progression of either disease. However, reexposure to even small amounts of addicting substances sets a devastating cascade of relapse and associated behaviors. In this instance, addiction resembles malignancies rather than chronic diseases such as diabetes and hypertension. As in oncology, it may be appropriate to call a return to substance use the “recurrence” of the disease state.
Conclusions
The push by the past head of NIAAA, Enoch Gordis that “treatment works” may have resulted in trying to find secondary outcomes in order to demonstrate that the treatment is effective. Furthermore, expensive medications developed by financially motivated pharmaceutical companies create an underlying bias of developing outcome measures that are short of complete abstinence, but nonetheless superficially appear reasonable for FDA approval of these medications. The existence and further maintenance of expensive budgets of NIAAA and NIDA may also have created another bias to accept less than complete abstinence as a reasonable model of recovery [30]. On the surface, it may seem acceptable and humane to have harm reduction strategies as outcome measures in addiction. In doing so, however, we are doing a disservice to the patients. These outcomes have been taken straight out of models of chronic diseases, such as diabetes and hypertension. Indeed, substance use disorders are chronic conditions; however, because of the very nature of addiction, the similarity ends quickly between chronic diseases and substance use disorder. The neurobiology of addiction is complex, and the priming model described above suggests that even a minimal reexposure to the substance after long periods of abstinence or extinction can induce a full-blown relapse. This relapse is different than the other chronic diseases such as diabetes and hypertension because the simple act of taking a small amount of a drug can induce a profound and ongoing dysfunction due to priming of the central nervous system. Therefore, once reexposure to an addictive substance occurs, unfortunately, the disease quickly begins to escalate and progress.
One of the diagnostic criteria of addiction is a loss of control over the quantity consumed. If subjects, when exposed to reinforcing substances, can control their disease and not deteriorate in a full-blown relapse, they will not qualify for the diagnosis of addiction in the first place. This is a prima facie evidence against using less-than complete abstinence as a primary outcome in addiction. Complete abstinence from all reinforcing substances needs to be the primary goal in substance use disorder treatment. The intramuscular long-acting opioid antagonist in clinical studies must have failed to demonstrate sustained abstinence from alcohol or opioids. Otherwise, why would you choose convoluted outcome measures used by pharmaceutical industry to demonstrate the efficacy of these drugs in the first place? The expense associated with intramuscular naltrexone (Vivitrol®) is in excess of $15000 per annum. This cost does not justify its use. We believe that the contingency contracting model utilized by physicians is underutilized in addiction treatment in the general population. The barriers to utilization of this model include a lack of reimbursement for longer-term monitoring and the culture in the treatment industry, which is weighted towards the initial treatment phase rather than the aftercare. Educating the employers to be the stakeholders in their employees’ recovery, and adequate reimbursement by insurance companies will begin to change the current paradigm. It is ethically problematic that physicians have a substantially higher success rate in addiction treatment in the USA than the general population. Clinicians have to redouble their efforts to level the playing field for our non-physician patient population.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
