
Case Report | DOI: https://doi.org/10.31579/2641-0419/266
1 Clinical cardiology specialist, Echocardiographist, Cardio-oncologist. Echocardiography department. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, CDMX. Fax number: None.
2 Clinical cardiology specialist, Echocardiographist. Echocardiography department. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, CDMX. Fax number: None.
3 Clinical cardiology specialist, Echocardiographist. Echocardiography department. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, CDMX. Fax number: None.
4 Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, CDMX. Fax number: None.
5 Clinical cardiology specialist, Echocardiographist. Cardiology division. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga 15, Belisario Domínguez Secc 16, Tlalpan, 14080 Ciudad de México, CDMX. Fax number: None.
*Corresponding Author: Zuilma Y. Vásquez-Ortiz MD, PhD. Echocardiography Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Vasco de Quiroga #15, Tlalpan, Mexico city. PC 14349.
Citation: Vásquez-Ortiz Zuilma Yurith, Fernández-Campos Beatriz A, Aceves-Velázquez Eduardo D, Ramírez-Cervantes Rolando D, Oseguera-Moguel, Jorge (2022). Extensive Intravascular Leiomyomatosis with Cardiac Involvement, Clinicopathological and Imaging Characteristics: A Case Report. J. Clinical Cardiology and Cardiovascular Interventions, 5(7); Doi:10.31579/2641-0419/266
Copyright: © 2022 Zuilma Y. Vásquez-Ortiz, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 April 2022 | Accepted: 17 May 2022 | Published: 01 June 2022
Keywords: intravascular leiomyomatosis; uterine myomatosis; heart failure; echocardiography
Intracardiac masses are a rare differential diagnosis in patients who present heart failure symptoms, these are classified by many authors as neoplastic or non-neoplastic, dependent or not on the heart chambers. Being able to differentiate and classify intracardiac masses is very important because treatment and prognosis depend on it. Intravascular leiomyomatosis is one of the rarest tumors, characterized by direct overgrowth of a uterine leiomyoma through adjacent veins with an unusual growth pattern. To date, less than 300 cases have been reported, with proliferation to the heart chambers being even rarer. We present the case of a female who presented to the emergency department due to dyspnea and palpitations, during his approach, a mass from the inferior vena cava was found causing intermittent tricuspid obstruction. Later it was documented as coming directly from the uterus, diagnosing intravascular leiomyoma by pathology.
Intravascular leiomyoma is a very rare benign neoplasia which depending on its extension can be asymptomatic until causing heart failure symptoms or pulmonary hypertension, the first imaging study indicated in heart failure symptoms is the transthoracic echocardiogram. The differential diagnosis of intracardiac masses must always be considered, although they are rare, their timely detection can lead to a better evolution of the patient.
Intravascular leiomyoma (IVL) is a rare benign neoplasia described first by Birsh-Hirshfeld in 1896 [1]. It´s characterized by the histological proliferation of benign smooth muscle cells through vascular structures without invasion of other tissues. Generally, IVL affects premenopausal and multiparous women, with symptoms depending on the site of origin (intrauterine venules or the myometrium) and the extent of invasion. There are no specific clinical manifestations of IVL, symptoms depend on the extension and size of the tumor, it can range from pelvic pain, abnormal uterine bleeding to infertility. If there is invasion to the cardiac cavities, it can cause fatigue, palpitations, chest pain, dyspnea, ascites, abdominal pain and hepatomegaly, syncope and even sudden death. [2,3] IVL has a serpentine appearance, proliferates throughout the venous system, but doesn´t invade it. Usually grows in the iliac veins or the inferior vena cava although there are very few reported cases with direct extension to the right atrium and causing symptoms of acute heart failure. [3,4]
A 51-year-old woman presented to the emergency department with progressive dyspnea of 2 weeks' duration progressing to rest (New York Heart Association Functional Class IV), palpitations, general state attack and lower limb edema. Five years ago, she was diagnosed with uterine myomatosis, morbid obesity, and mixed dyslipidemia. Transthoracic and transesophageal echocardiograms on admission showed a heterogeneous mass in the right atrium of large dimensions and regular borders, that emerged from the inferior vena cava, without adherence to the interatrial septum or other neighboring structures. This mass protruded into the right ventricle in each cardiac cycle, conditioning intermittent obstruction and tricuspid stenosis with a mean gradient of 8mmHg (Figure 1).

Once it was observed that the tumor came from the inferior vena cava, an abdominal contrast computed tomography (CT) was performed. CT showed a tumor originated in the uterus, adjacent to the anterior and lower left wall. The lesion was observed with 3.7 centimeters thick, tubular, and hypodense course, following a posterior and cephalic path, decreasing in caliber in the distal portion. The extension was observed starting through the left ovarian vein to the ipsilateral renal vein, which continued its course through the inferior vena cava showing filling defects until it falls into the right atrium. (Figure 2).

Faced with sudden hemodynamic deterioration, it was decided to undertake emergency surgery jointly by a multidisciplinary surgical team. An open resection of the right atrial tumor was performed in a single surgical time together with total abdominal hysterectomy and bilateral salpingo-oophorectomy to reduce tumor recurrence. Microscopic analysis demonstrated a uterine lesion with intertwined muscle bundles of spindle cells, homogeneous size, with oval nuclei with positive immunohistochemistry for smooth muscle markers (desmin and smooth muscle actin) and estrogens and progesterone, concluding leiomyoma, without evidence of malignancy. (Figure 3)
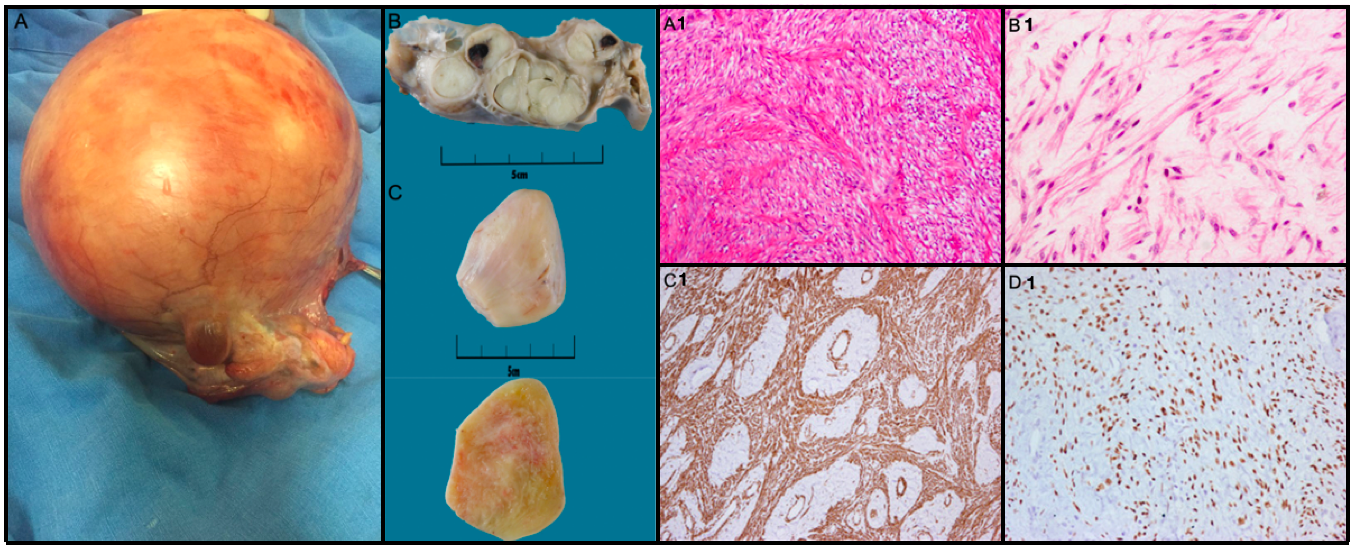
A1) Hematoxylin and eosin staining of uterine lesion with spindle-shaped cells and homogeneous size. B1) Hematoxylin and eosin staining showing abundant extracellular stroma and spindle cells, no cellular irregularities or nuclear pleomorphisms. C1) Immunohistochemical staining is positive for smooth muscle markers. D1) Intracavitary tumor is positive immunohistochemical staining for estrogen receptors.
IVL occur mainly in caucasian premenopausal women with an average age of 40 years (between 20 and 70 years) with history of uterine leiomyomatosis [1,5,6]. Less than 300 cases of IVL have been reported in the literature and only 10% have had repercussions with the
characteristics of our patient. [4,7] The specific etiology of IVL is not clear, and there are two theories to explain the existence of this neoplasia: One theory is that the leiomyomas originate from the uterine vein wall growing through the vessels. Another theory is the invasion projections of uterine fibroids into blood vessels [8] and they have been associated with high levels of estrogens. Intravascular extension can occur concomitantly with uterine leiomyomas or occur even years after hysterectomy [5]. IVL macroscopically has a serpentine appearance and can range in size from a few centimeters to half a meter or more. Is a benign tumor by histology; however, it can invade surrounding tissues and have a high rate of recurrence. Can grow along the veins or lymphatic vessels and in addition to the vena cava, these tumors can extend into the hepatic and renal veins or can even reach the pulmonary arteries [1,2]. The main differential diagnosis to consider is atrial myxoma. Is the most common benign primary tumor, reaching up to 70-80% of all. Most are found in the left atrium and originate from the interatrial septum. [7,8]
The echocardiogram is considered the first-line imaging modality for the evaluation of intracardiac masses, can provide real-time information, helps to characterize them and the hemodynamic repercussion they cause. IVL appear as a mobile solid myxomatoid mass and long intravascular serpentine. [4] It is visualized emerging through the inferior vena cava and limited to the right cavities without invading them. The most common location is the right atrium and depending on its length, can be as a floating mass or can protruding through the tricuspid valve into the right ventricle, even across pulmonary arteries. [2,4,5]
The Cardiac computed tomography (CCT) can provide additional information about the location and size, the invasion of intracardiac structures and the secondary effects on the cardiac anatomy. IVL are seen
as low-density tumors with a “snakelike” image, with mild heterogeneous enhancement and don´t generate invasion of contiguous structures. It can also be used to assess the origin and extension of the IVL, can be found as filling defects in the veins and thickening of the vessels. [2,8,9] Can also be found incidentally on abdominal CT taken for another reason, with no apparent impact on adjacent organs. To assess tumor spread Guotao Ma, et al. classified the IVL into 4 stages: Stage I, tumors penetrate towards the uterine venous wall, but is limited to the pelvic cavity; Stage II, tumors has extended into the abdominal cavity, but had not overtaken the renal vein; Stage III, tumors overtake the renal vein and inferior vena cava, and even penetrate into the right atrium, but had not reached the pulmonary arteries; Stage IV, tumors overtake the pulmonary arteries and/or lung metastases were observed. [9]
Histologically the intravascular tumor, which often has a lobulated contour, resembles a typical uterine leiomyoma, findings include endothelium-covered of uniform spindle-shaped smooth muscle proliferations within the vascular lumen with neoplastic cells that show minimal atypia and a low mitotic index (2, 4). Some reports have found estrogen and progesterone receptors in the extracted pieces, although they are not consistent, they are associated with a better prognosis. The cytogenetic study has revealed an abnormal karyotype with 45,XX,der(14)t(12;14)(q15;q24) in different studies, however its etiology remains unknown to date. [2,10]
The complete surgical resection of the tumor and its intravascular implants is the only current effective treatment. The extension of the surgery depends on the extension of the IVL, can be done in one or two times depending on the surgical risk of the patient. In patients who are not candidates for surgery or if the entire tumor will not be removed, hormonal therapy with antiestrogens can be used with variable results. [2,9,10] Due to the rareness of the pathology, the recurrence rate is not exactly known, which can reach up to 30-40%. This due to micro or macroscopic remnants after surgery or new growth. For this reason, follow-up imaging studies are suggested every 3 to 6 months, because recurrence can be faster and fatal than the primary tumor. [2]
Intracardiac tumors are a rare differential diagnosis that we must not forget in a patient with heart failure. The correct and appropriate diagnosis can influence the prognosis and survival of the patient. IVL should be considered when a right atrium mass is found and does not depend on the walls of the myocardium. Especially in patients between the fourth and fifth decades of life and history of hysterectomy, myomectomy or concomitant uterine leiomyomas. Evaluation by echocardiography is essential to determine the origin and extension of intracardiac tumors as well as the hemodynamic repercussion caused. High-resolution CT or MRI can be used to determine the origin and extent. Each imaging modality can provide different information about the lesion and is complemented by others. The complete removal of the tumor has shown excellent results together with a close follow-up to monitor recurrences and to be able to offer timely medical or surgical treatment. The factor that most influences this type of pathology is timely detection. Having a high level of suspicion and performing multimodality cardiovascular imaging protocols early has a positive impact on the prognosis of patients.
The authors declare no conflict of interest.
No grants, contracts, and other forms of financial support were required.
The authors have no disclosures to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
