
Research Article | DOI: https://doi.org/10.31579/2641-0419/405
1Department of Psychiatry, Royal Brisbane and Women’s Hospital, Brisbane, QLD, Australia
2Department of Cardiology, Blacktown Hospital, Sydney, NSW, Australia
3Western Sydney University, Sydney, NSW, Australia
4University of Queensland, QLD, Australia
*Corresponding Author: Maxwell Qu, Department of Psychiatry, Royal Brisbane and Women’s Hospital, Brisbane, QLD, Australia.
Citation: Maxwell Qu, Iman Awan, Shaun Khanna, Anjalee Amarasekea, Aditya Bhat, et al, (2024), Exploring the Association between Anxiety and Atrial Fibrillation using two Quantitative Psychometric Tools: A Systematic Review and Meta-Analysis, J Clinical Cardiology and Cardiovascular Interventions, 7(12); DOI: 10.31579/2641-0419/405
Copyright: © 2024, Maxwell Qu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 August 2024 | Accepted: 18 October 2024 | Published: 29 October 2024
Keywords: atrial fibrillation; anxiety disorder; anxiety screening; state-trait anxiety inventory; stai-state; stai-trait; zung’s self-rating anxiety scale; zung’s sas
Background: Anxiety is widely prevalent, exhibiting higher rates among individuals with chronic health conditions, notably cardiovascular diseases such as atrial fibrillation (AF). Studies have shown interventions targeting anxiety can improve AF outcomes, while AF management can reduce anxiety levels. This study explores the association between AF and anxiety by comparing anxiety levels in AF populations with healthy controls.
Materials and Methods: A systematic review adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) principles was conducted to identify relevant studies through medical databases and grey literature sources. Various psychometric tools, including the Spielberger State-Trait Anxiety Inventory (STAI) and Zung's Self-Rating Anxiety Scale (SAS) were considered for assessing anxiety severity. Meta-analysis was performed using a random-effects model to analyse continuous variables, with the overall effect size quantified as the standardized mean difference (SMD).
Results: 5 study samples (327 AF patients for STAI-State, 171 AF patients for STAI-Trait) and 3 study samples (209 AF patients) using Zung's SAS were included in the meta-analysis, along with 3 respective control samples. Compared to control groups, AF patients exhibited significantly higher scores for STAI-State (SMD 1.13; CI: 0.57-1.69, p<0.01, I²=81%), STAI-Trait (SMD 0.54; CI: 0.09-0.99, p=0.02, I²=67%), and Zung's SAS (SMD 1.85; CI: 1.58-2.13, p<0.01, I²=22%).
Conclusions: AF patients demonstrated elevated levels of anxiety, as indicated by higher STAI and Zung's SAS scores compared to controls. These findings suggest an association between AF and anxiety. The study highlights the importance of addressing mental health disorders in AF patients and vice versa.
Anxiety is a common complaint in clinical practice, with around 26% of the Australian population receiving a lifetime diagnosis of an anxiety disorder (1). The prevalence of anxiety-related conditions in the Australian population has shown an increase from 11.2% in 2014-2015 to 13.1% in 2017-2018 (2).
Atrial fibrillation (AF), the most prevalent arrhythmia, affects 1-2% of the general population and has a higher occurrence among individuals over the age of 80 (3). Research indicates a higher prevalence of anxiety disorders in patients with AF compared to the general population, suggesting a possible association between the two (4). Coumel's triangle is a conceptual framework that outlines three factors linking anxiety and AF. These include the arrhythmogenic substrate (structural heart disease), the trigger factor (e.g., hyperactive HPA axis and increased catecholamine release), and the modulation factor (autonomic nervous system). Anxiety affects all three components (5).
Anxiety symptoms can influence a patient's self-perception and perception of the world through an overactive autonomic nervous system, leading to physiological manifestations of the sympathetic response and affecting the arrhythmogenic substrate (6). Interventions targeting anxiety symptoms such as mindfulness, interoceptive exposure therapy, or exposure-based have shown to decrease AF occurrence, supporting the hypothesis that anxiety fosters AF persistence (7, 8, 9). Conversely, AF palpitations can mimic or exacerbate anxiety symptoms, and studies have reported an improvement in anxiety following interventions for AF (10). Thus, a bidirectional or causative pathway between AF and anxiety may exist.
Understanding the connection between anxiety disorders and AF has significant implications for both mental and cardiac health. This insight can inform clinical strategies unhindered by traditional approaches, which often separate mental and physical health. This study aims to examine the association between anxiety disorders and AF, with the hypothesis that anxiety not only fosters AF persistence, but that AF also aggravates anxiety, emphasising a bidirectional or causative link between these two conditions.
2.1 Search Strategy and Selection for Peer-Reviewed and Grey Literature
The review followed the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines (11) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (12). The review protocol was registered on PROSPERO (registration number CRD42021281133).
A comprehensive search was conducted in major medical databases (CINAHL, PubMed, Ovid Medline, EMBASE, Web of Science, SCOPUS, ProQuest, Science Direct, and Cochrane Central Register of Controlled Trials) from 2000 to May 2022. Grey literature searches were performed using Google Scholar, WHO International Clinical Trials Registry Platform, and ClinicalTrials.gov. Search terms, including free-text and Medical Subject Heading (MeSH) terms, were used to identify English studies reporting standardised measures for anxiety symptoms and AF. Detailed search terms and strategies are presented in ‘Table 1’.
| Concept 1 | Concept 2 | Concept 3 | ||
| “Atrial Fibrillation”, “AF”, “NOT atrial flutter”, “Arrhythmia” | “Anxiety”, “Anxiety Symptoms”, “Anxiety Disorders” | “Anxiety Questionnaires”, “Anxiety Psychometrics”, “Anxiety Scoring Systems”, “Anxiety Scales”, “Anxiety State Score”, “Anxiety Trait Score”, “State-Trait Anxiety Inventory”, “Spielberger State-Trait Anxiety Score”, “STAI”, “Zung Self-Rating Anxiety”, “Zung SAS”, “SAS”, “Anxiety Sensitivity Index”, “ASI”, “HADS-A”, “HAM-A”, “GAD-7”, “GADQ”, “Generalized Anxiety Disorder Assessment”, “HADS-A”, “BAI”, “Beck Anxiety Inventory”. | ||
Table 1. A table showing three key concepts and the search terms used for each. For each concept, various search strategies were employed. All three concepts used the AND operator to link them to focus the search, and in the search terms for Concept 3, the OR operator was employed to broaden the search.
2.2 Definition and Psychometric Tools for Anxiety Disorders
Anxiety disorders were defined based on diagnostic criteria from DSM-IV to DSM-5-TR (13) or clinically significant anxiety scores measured by validated psychometric instruments. Symptoms falling below these diagnostic thresholds will not be considered indicative of an "anxiety disorder." Various psychometric tools considered to assess anxiety symptoms included the Hamilton Anxiety Scale (HAM-A), Spielberger State-Trait Anxiety Inventory (STAI), Zung's Self-Rating Anxiety Scale (SAS), Depression Anxiety Stress Scale (DASS), and Generalised Anxiety Disorder rating scale (GAD-7) (14).
2.3 Inclusion and Exclusion Criteria
Studies that measured anxiety in patients with AF using diagnostic criteria from DSM-IV to DSM-5-TR or standardised scoring systems were included in the analysis for the period between January 2000 and May 2022. Studies without quantitative data, involving paediatric samples, published only as abstracts without full articles, or relying on non-specific psychometric measures (e.g., SF-36) were excluded. Also, studies involving participants with overt depressive symptoms were excluded due to the established association between depression and cardiovascular conditions (15, 16).
2.4 Data Extraction and Quality Assessment
Retrieved records were analysed, considering data such as author, publication year, references, study design, participant characteristics, age, and outcome measures. Only completed studies with available results were included. Data were collected using a predefined template in Microsoft Excel. Discrepancies were resolved through discussions before finalising the literature summary table. The quality of the final literature was evaluated using the critical appraisal tools provided by the Joanna Briggs Institute (JBI) (17) to appraise the data and identify studies with bias or confounding factors for further exclusion.
2.5 Statistical Analyses
The meta-analysis incorporated studies that provided means and standard deviations for anxiety measures. Methodological differences and study design were considered. The statistical analysis included reporting quantitative indices, sample size, mean, confidence interval (CI), and standard deviation (SD). Due to a greater number of intervention groups than controls, the control samples were reused with adjusted sample sizes to prevent conflation of statistical results. This correction was achieved by dividing the control sample size by the number of repeated observations required to match the corresponding intervention groups.
Heterogeneity within studies was assessed using the I2 statistic. Random-effects models and standardised mean difference (SMD) were used to estimate the overall effect size. Publication bias was evaluated using funnel plot asymmetry (Egger's test) (18). A significance level of p < 0>
3.1 AF Population Search Results
Based on the literature search, a total of 478 studies were identified for the AF population. After screening based on title and abstract, 447 articles were considered, and 48 studies underwent full-text assessment. 13 studies remained for further consideration for a meta-analysis after applying exclusion criteria. A PRISMA flow diagram depicting the study selection process and reasons for exclusion can be found in 'Figure 1'.
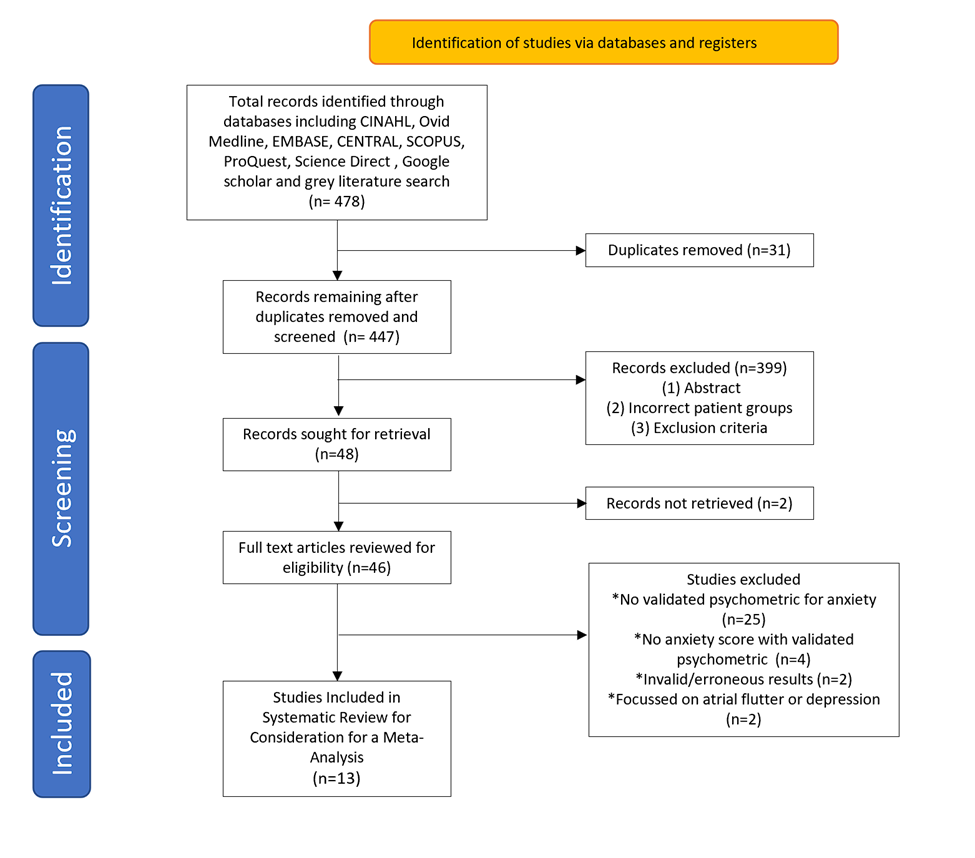
Figure 1: PRISMA flow chart detailing the identification and screening of records for the systematic review and meta-analysis, including reasons for exclusion.

Figure 2: Forest Plot for the meta-analysis of the STAI-State Scores with the AF populations demonstrating statistically significant higher scores compared to the controls.
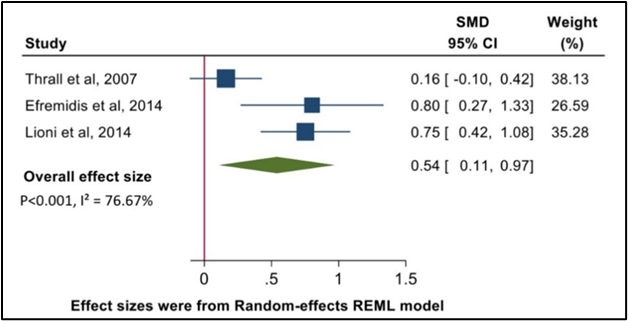
Figure 3: Forest Plot for the meta-analysis of the STAI-Trait Scores with the AF populations demonstrating statistically significant higher scores compared to the controls.
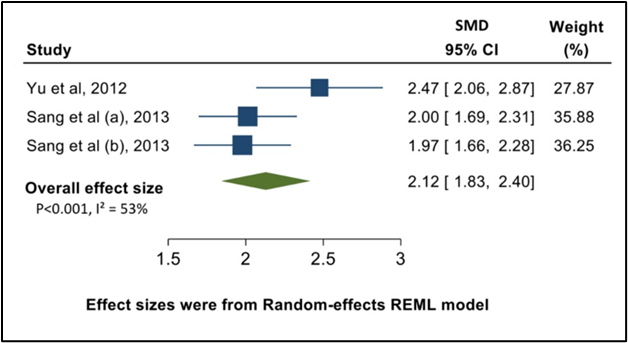
Figure 4: Forest Plot for the meta-analysis of Zung's SAS with the AF populations demonstrating statistically significant higher scores compared to the controls.
‘Sang et al (a)’ refers to the meta-analysis of the AF group that received cardiac ablation treatment, and ‘Sang et al (b)’ refers to the AF group that received antiarrhythmic drugs (AAD) treatment.
The 13 studies were assessed for their suitability for inclusion in the meta-analysis. To ensure meaningful statistical analysis, it was necessary to have at least 3 study samples per anxiety measurement tool. Consequently, 6 studies using anxiety scoring systems with fewer than two additional samples using the same tool were excluded. The 7 remaining studies, which employed the STAI-State and Trait and Zung’s SAS measuring tools, underwent further quality appraisal.
3.2 Control (non-AF) Population Search Results
The control samples in the 7 AF studies had either invalid data or potential confounders such as hypertension, other arrhythmias, and depression. External studies utilising STAI and Zung’s SAS scoring systems were therefore necessary to obtain corresponding control samples to conduct a meta-analysis (11).
The same methodology and databases used in the AF population search were applied to identify suitable control populations. The search terms “without AF”, “healthy” and “normal” were used instead of “AF” to screen for studies without AF or significant co-morbidities. Specific search terms for “STAI”, “Zung’s SAS” and similar were also utilised to acquire studies with compatible quantitative data. Identical inclusion and exclusion criteria applied to the AF population search results were used in the screening process for the control studies.
For the control population, the initial search within peer-reviewed journals using terms like "healthy," "STAI," and "Zung's SAS" yielded 636 and 211 results, respectively. However, these studies were excluded due to various reasons, including irrelevance, unavailability, absence of relevant scores, or inclusion of patients with depression. A subsequent search on Google Scholar and grey literature produced limited relevant results, with only two studies meeting the inclusion criteria. These two studies provided the mean STAI and Zung’s SAS scores respectively for the control group.
Quality Appraisal and Characteristics of the Study Cohort
The 7 AF and 2 control studies underwent quality assessment using the JBI tool to determine their suitability for the meta-analysis. Various critical appraisal tools were considered to guide the selection for the meta-analysis.
As the control studies were external to the AF studies, the Checklist for Cohort Studies (19) was deemed unsuitable, and the Checklist for Analytical Cross-Sectional Studies (20) was employed instead. This checklist was modified to include the appraisal of both the AF and control groups. The quality appraisal tool consisted of 8 questions to assess the studies and evaluate potential bias and threats to validity. Both authors reached a consensus in completing this process, and an additional column was included to provide an overall impression.
The results of the quality appraisal can be found in ‘Table 2’. Each study was assigned a score of '1' if it met the quality requirement or '0' if it did not. The total score was calculated as the sum of these factors. Studies with a total score below '3' were considered of poor quality and excluded from the meta-analysis. Scores of '4' indicated fair quality, '5' indicated good quality, and '6' or above indicated excellent quality. No studies from either the AF or control groups were excluded based on this process.
| Quality appraisal study table | Inclusion criteria clearly defined in the sample? | Were the study subjects and the setting described in detail? | Was the exposure measured in a valid and reliable way? | Was the control measured in a valid and reliable way? | Were objective, standard criteria used for measurement of the condition? | Were confounding factors identified? | Were strategies to deal with confounding factors stated? | Were the outcomes measured in a valid and reliable way? | Overall rating | Quality assessment |
| Efremidis et al | 1 | 0 | 1 | N/A | 1 | 0 | 0 | 1 | 4/7 | Fair |
| Thrall et al | 1 | 1 | 0 | N/A | 1 | 1 | 0 | 1 | 5/7 | Good |
| Kupper et al | 1 | 1 | 0 | N/A | 1 | 0 | 0 | 1 | 4/7 | Fair |
| Lioni et al | 1 | 1 | 1 | N/A | 1 | 0 | 0 | 1 | 5/7 | Good |
| Jeon et al | 1 | 1 | 1 | N/A | 1 | 1 | 0 | 1 | 6/7 | Excellent |
| Yu et al | 1 | 1 | 1 | N/A | 1 | 1 | 0 | 1 | 6/7 | Excellent |
| Sang et al | 1 | 1 | 1 | N/A | 1 | 1 | 0 | 1 | 6/7 | Excellent |
Donzuso et al (STAI control) | 1 | 1 | N/A | 1 | 1 | 1 | 0 | 1 | 6/7 | Excellent |
Dunstan et al (SAS control) | 1 | 1 | N/A | 1 | 1 | 0 | 0 | 1 | 5/7 | Good |
Table 2. Use of the Modified Joanna Briggs Institute Critical Appraisal tools for use in Analytical Cross-Sectional Studies (JBI tool) to assess the quality of included studies.
3.3 Included Studies in the Meta-Analysis
The meta-analysis included 11 study samples from the AF group and 3 study samples from the control group. Detailed information about the included studies, such as study design, sample size, demographics, anxiety scoring systems used, mean anxiety scores, confounding factors, and limitations, can be found in ‘Table 3’
| First Author, Year, Country, Type of Journal | Study Design | AF Subjects (n) | Age | Gender (% Male) | Anxiety Scoring System | Mean Anxiety Score | Adjusted Factors | Summary of Results | Limitations |
Kupper, 2013 (21) Netherlands Peer-Reviewed | Prospective cohort
Treatment Trial | 21 | 68±9.4 | 61.2 | STAI-State | 37.5 | Age, sex | AF patients experienced significantly higher levels of anxiety than matched persons from the general population. | Measured paroxysmal and persistent AF – reliability and validity of results reduces. Small Sample Size. High attrition rate, although not relevant for this review. |
Efremidis, 2014 (22) Greece Peer-Reviewed | Prospective cohort
Treatment Trial | 16 | 56.9±9.7
| 68.8
| STAI-State | 49.9 | Age, sex, BMI, diabetes, hypertension | Baseline STAI-Trait was associated with AF recurrence. Measures of anxiety were higher in those with AF recurrence compared to those without. Furthermore, there was a significant improvement in QoL, anxiety, and depression after left atrial ablation. | Small Sample Size. Poor generalisability – only paroxysmal AF included.
|
| STAI-Trait | 41.9 | ||||||||
Lioni, 2014 (23) Greece Peer-Reviewed | Retrospective cohort | 54 | 56.4±12.5
| 59.3
| STAI-State | 45.53 | Ischaemic Heart Disease risk factors | Higher STAI-state and -trait scores were seen in patients who suffered AF comparing to those with SVTs. | Small Sample Size. Poor generalisability – only paroxysmal AF included. Risk of confounding – AF population had high percentage of males. |
| STAI-Trait | 42.18 | ||||||||
Jeon, 2014 (28) (Non-Type D)
| Prospective cohort | 163 | 55.9±12.0 | 80.4 | STAI-State | 39.9 | Age, Sex, Partner, Education, BMI, cardiac and medical co-morbidities, Echocardiogram results, depression | The mean baseline scores on the STAI-State were significantly higher in the Type D personality group compared to the non- Type D personality group. | Small Sample Size with Type-D personality.
Poor generalisability – only paroxysmal AF included. |
Jeon, 2014 (28) (Type D) South Korea Peer-reviewed | 73 | 55.6±11.9 | 82.2 | STAI-State | 48.9 | ||||
Thrall, 2007 (53) UK Peer-reviewed | Retrospective cohort | 101 | 66.3±11.0
| 61.4 | STAI-Trait | 37.4 | Age, sex, Ethnicity, Occupation | AF patients displayed higher levels of trait-anxiety (p < 0> | Retrospective study design with self-assessment questionnaires – recall bias.
Risk of confounding – female patients were older than males.
Poor generalisability – only paroxysmal AF included. |
Yu, 2012 (26)
China Peer-reviewed | Prospective cohort
Treatment Trial | 43 | 58.3±7.3 | 67 | Zung’s SAS | 49.76 | Not mentioned
| CPVA (Circumferential vein ablation) can ameliorate anxiety and depression, which may contribute to improvement of quality of life in patients with paroxysmal AF in comparison with pharmacological treatment. Anxiety and depression increase the recurrence risk of AF after CPVA. | Sampling Bias – participants chose their treatment method.
Small Sample Size.
Poor generalisability – only paroxysmal AF included. Risk of confounding - analyses of the data did not adjust for factors. |
Sang, 2013(10) (Ablation Group) | Prospective cohort
Treatment Trial | 82 | 55.9±6.1 | 67 | Zung’s SAS | 48.6
| Not mentioned
| Catheter ablation was effective in reducing symptoms of depression and anxiety and improving QoL, and it was superior to AAD therapy. | Sampling bias – non-randomised assignment of patients. Small Sample size. Poor generalisability – only paroxysmal AF included. Risk of confounding - analyses of the data did not adjust for factors. |
Sang, 2013(10) (AAD Group)
China Peer-reviewed | 84 | 57.2±5.4 | 69 | Zung’s SAS | 47.7 | ||||
| Control Populations | Exclusion Criteria | Limitations | |||||||
Donzuso, 2014 (27)
Italy Peer-reviewed | Cross-sectional | *121 | 38.7±15.1 | 33 | STAI-State | 35.73 | Not mentioned
|
| Risk of confounding - analyses of the data did not adjust for factors. |
| STAI-Trait | 34.1 | ||||||||
| Dunstan, 2020 (28) | Cross-sectional | *178 | **N/A | **N/A | Zung’s SAS | 32.2 | Not mentioned
|
| Response bias - 2 similar self-report assessments were provided; PHQ-9 and Zung’s SAS risking inflation (or deflation) of responses. |
Table 3. Details of the studies, extracting relevant data and determining the limitations and risk of bias.
| AF Populations | ||||
| Anxiety Scoring System | Total Number of Participants | Total Percentage Male | Mean Age | Mean Anxiety Score |
| STAI-State | 327 | 75.52 | 56.74 | 43.17 |
| STAI-Trait | 171 | 45.25 | 62.29 | 39.3 |
| Zung’s SAS | 209 | 67.80 | 45.41 | 48.4 |
| Control Populations | ||||
| STAI-State | 121* | 33* | 38.7* | 35.73 |
| STAI-Trait | 121* | 33* | 38.7* | 34.1 |
| Zung’s SAS | 178 | **N/A | **N/A | 32.2 |
Table 4. Comparison of the patient demographics and mean anxiety score between the AF and control populations. It provides an overall comparison of patient demographics between the AF and control populations, specifically reporting the number of subjects, mean anxiety scores, age, and gender.
*Both the STAI-State and STAI-Trait scores in the control group were obtained from the same study.
** No information regarding age or gender was explicitly specified for this sample.
The control STAI-State group had a higher proportion of males and was older compared to the AF population. The AF STAI-Trait group had a more balanced gender proportion but exhibited a higher age discrepancy compared to the control STAI-Trait group. Limited demographic information was available for the control Zung's SAS group.
Clinically significant anxiety was determined based on the respective cut-off scores of the anxiety scales used. Scores above 40 for both the STAI-State and STAI-Trait inventories indicate probable significant anxiety (29). For Zung's SAS, a raw cut-off score of 36 is generally used in the clinical setting, but for research purposes, it is recommended to use a higher cut-off score of 40 to reduce the chance of false positives and negatives (28).
3.4 Meta-Analysis Results
In the meta-analyses, patients with AF had significantly higher anxiety scores in STAI-State (SMD 1.13; CI: 0.57-1.69, p<0 I²=81%), p=0.02, I²=67%), I²=22%)>
No significant publication bias was found for STAI-State (p-value=0.46) and STAI-Trait (p-value=0.28) with symmetric funnel plots in ‘Figures 5 and 6’, but indications of small study effects and publication bias were observed for Zung's SAS (p-value=0.04) in ‘Figure 7’.
| Anxiety Scoring System | Number of Study Samples | Number of AF Patients | Number of Control Patients | Overall Effect Size (SMD) | 95% CI | p | I2 |
| STAI-State | 5 | 327 | 121 | 1.13 | 0.57-1.69 | <0> | 81 |
| STAI-Trait | 3 | 171 | 121 | 0.54 | 0.09-0.99 | 0.02 | 67 |
| Zung’s SAS | 3 | 209 | 178 | 1.85 | 1.58-2.13 | <0> | 22 |
Table 5. Comparison of the Meta-analysis of the Anxiety scoring systems.
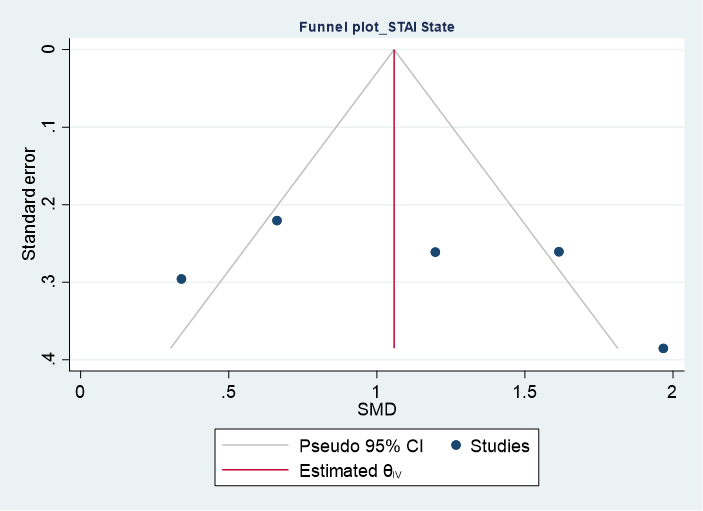
Figure 5. Funnel Plot for STAI-State Scores demonstrating no small study effects and a reduced risk of publication bias. Egger’s Test p-value = 0.46 (not significant).
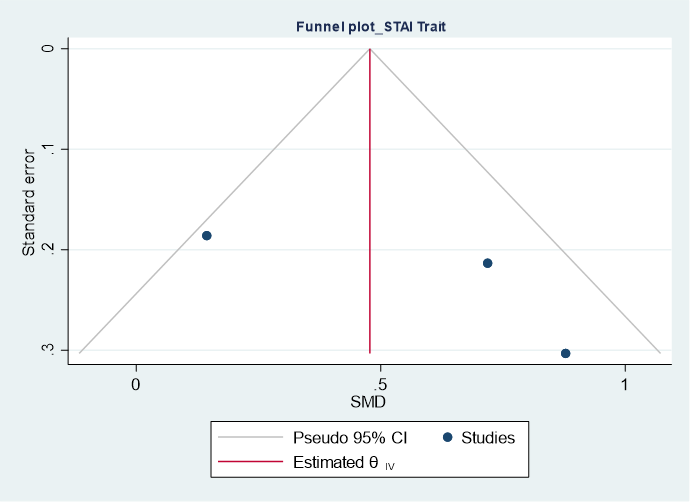
Figure 6. Funnel Plot for STAI-Trait Scores demonstrating no small study effects and a reduced risk of publication bias. Egger’s Test p-value = 0.28 (not significant).
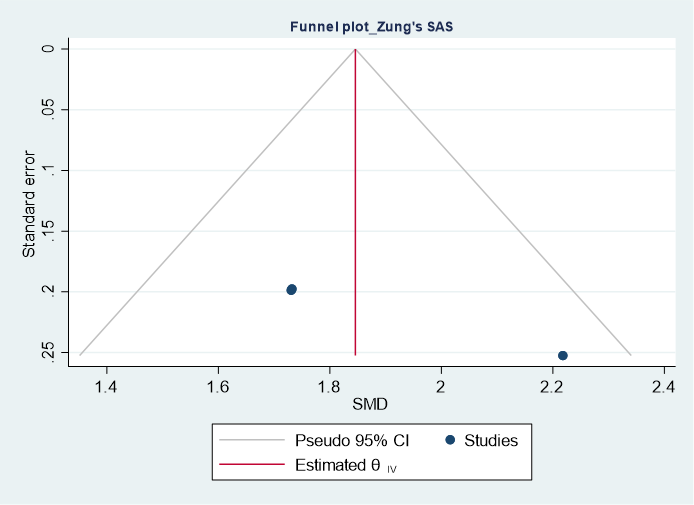
Figure 7. Funnel plot for Zung's SAS demonstrating presence of small study effects and an increased risk of publication bias. Egger’s Test p-value = 0.04 (significant).
Heterogeneity was observed in STAI-State and STAI-Trait scores, while Zung's SAS showed lower heterogeneity. ‘Table 5’ provides a summary of the meta-analyses, including effect sizes (SMD) and heterogeneity.
This study supported an association between AF and anxiety by showing that patients with AF had significantly higher anxiety scores compared to healthy populations. These findings emphasise the need to screen for anxiety in AF patients and vice versa.
Furthermore, this study compared the effect sizes of STAI-State and STAI-Trait. The results showed that STAI-State had a larger effect size than STAI-Trait, suggesting that cross-sectional and transient anxiety may have a greater impact on AF than chronic and longitudinal anxiety. This finding aligns with previous studies that have linked anxiety symptoms to stressful life events, such as partner loss, which can transiently increase the risk of AF (30, 31, 32).
The meta-analysis does not establish a causal relationship between anxiety and AF but suggests an association between the two disorders. Supporting this association, a study on permanent AF found a high prevalence of anxiety symptoms compared to the general population (28).
Other studies have explored interventions such as yoga training, internet-based cognitive behavioural therapy (CBT), and pharmacological agents like dabigatran, all showing improvements in anxiety symptoms and quality of life in AF patients (9, 33, 34). Additional studies highlight anxiety as the primary emotional response to an AF diagnosis (35). Perceptions of AF as a chronic and unpredictable condition with serious consequences are associated with higher levels of negative emotions and anxiety scores (36). Another study observed elevated anxiety sensitivity during treatment anticipation, which decreased over the intervention period (37). These findings align with the larger impact of STAI-State compared to STAI-Trait and provide an alternative explanation for the observed association between anxiety and AF.
AF can manifest in different types, such as new-onset, paroxysmal, persistent, long-standing persistent, and permanent AF (38). However, there is limited research directly comparing the different types of AF and their association with anxiety.
One study found that patients with persistent AF experienced high levels of emotional discomfort, including anxiety symptoms (21). Another study suggested that the unpredictability and fear of new episodes in individuals with paroxysmal AF contributed to a poorer quality of life (39). Additionally, another study demonstrated that frequent arrhythmias were associated with an increased likelihood of developing anxiety due to recurrent somatic symptoms (40).
The diagnosis of new disorders is commonly linked to anxiety, and informing patients about their diagnosis can help alleviate anxiety symptoms (41). Illness perception, influenced by various biopsychosocial-cultural factors, plays a role in the development of anxiety (39). Therefore, culturally-informed psychoeducation tailored to the patient's needs is essential in addressing anxiety in AF patients (42).
The Temporal Relationship between Anxiety and AF
Although the meta-analysis doesn't directly investigate the direction of the relationship between AF and anxiety, some studies included in the analysis offer insights. They compare pre-intervention and post-intervention anxiety symptom scores in individuals with AF, allowing for an exploration of temporality from AF to anxiety (10, 22, 26).
The observed psychological improvement after interventions for AF suggests that the cardiac autonomic modifications caused by AF may contribute to the development or perpetuation of anxiety (43). Other studies indicate a bidirectional relationship, suggesting that anxiety can increase the risk of AF recurrence, while cardiac interventions can alleviate anxiety symptoms in patients with AF (26).
Furthermore, several studies have found that baseline preoperative anxiety levels are significant predictors of AF relapse following intervention. This suggests that anxiety could be a modifiable risk factor or trigger for AF (22, 44, 45).
If future studies support anxiety as a modifiable risk factor for AF, it could present the possibility of implementing first-line psychological or psychiatric interventions for managing AF with minimal resource expenditure and side effects, such as internet-based CBT (9).
Considering the high prevalence of anxiety disorders and AF in the general population, the concept of managing AF as a modifiable risk factor for anxiety symptoms has practical implications in the clinical setting (1, 3). While the typical treatment for anxiety disorders involves antidepressants and/or psychotherapy, there is still a high rate of treatment resistance after 5 years (46). Recognising AF as a modifiable risk factor for anxiety symptoms could lead to screening and treatment for AF in patients with anxiety symptoms that have not responded to first-line management.
Furthermore, providing increased surveillance and support for anxiety symptoms in patients with AF could be beneficial, considering the barriers to receiving mental health support. This includes addressing stigma, cultural factors, and lack of awareness or access to care. In line with a holistic healthcare approach, low-risk psychiatric medications such as Selective Serotonin Reuptake Inhibitors (SSRIs) could be considered as a prophylactic measure in AF patients. This may improve quality of life and potentially lead to remission of AF symptoms. While the efficacy of SSRIs in anxiety may not be optimal (with a number-needed-to-treat [NNT] of 1 in 5) (47), comparing it to the efficacy of antiarrhythmic drugs for preventing tachyarrhythmia recurrence (which often requires a higher NNT 1 in 7) suggests its potential utility (48). Moreover, improvements in mental well-being can enhance treatment adherence (49) and strengthen the therapeutic alliance (50), while also reducing the burden on caregivers, families, and healthcare systems.
Potential confounders such as age, sex, and co-morbidities (e.g., hypertension) in the meta-analysis should be considered, as these imbalances in these factors may introduce bias. Some studies did not account for co-morbidities, complicating the AF-anxiety relationship. The inclusion of different AF types, small sample sizes, clinical diversity, and non-randomised designs contribute to heterogeneity and reduce the generalisability of the findings. Additionally, the use of self-reported anxiety scales, absence of clinician-rated measures, and retrospective study designs affect the reliability and validity of anxiety assessments, introducing response bias and complicating the evaluation of psychiatric diagnoses.
In summary, the study highlights an association between anxiety and AF, showing higher anxiety scores in AF patients compared to non-AF individuals. However, limitations such as the absence of appropriate control groups, small sample sizes, and reliance on self-reported measures need to be considered in the interpretation of the findings. Further research is needed to explore interventions for reducing anxiety in AF patients and assess the impact of effective AF control on anxiety symptoms.
Nevertheless, the findings underscore the importance of considering both psychiatric and cardiac health concurrently. Clinicians should be attentive to the interplay between anxiety and AF, adopting a biopsychosocial approach to improve patient outcomes and develop comprehensive management strategies for individuals with either condition.
The lack of direct studies comparing AF and anxiety makes it challenging to differentiate between confounders, effect modifiers, and mediators in their association. This prompts the exploration of alternative pathways to explain the observed phenomena.
For example, the stimulation of 5-HT4 receptors has been found to reduce anxiety (51) but also has a proarrhythmic role that could contribute to the development of AF (52) his suggests that other factors within the biopsychosocial-cultural model may contribute to the relationship between AF and anxiety.
Prospective studies with larger sample sizes directly exploring the relationship between AF and anxiety are needed to provide valuable insights and determine causality. Such studies would offer more clarity on the multi-faceted nature of this relationship. Additionally, investigating specific types of AF in relation to anxiety and utilising subgroup data can help identify potential confounders and elucidate hypothesised mechanisms.
Advancements in this area can have significant implications for patient care. By providing comprehensive education to patients about the disease burden and potential outcomes, they can contribute to a more thorough informed consent process, alleviate negative emotional effects, strengthen mental health advocacy, and improve the overall quality of life for patients.
The meta-analysis lacked studies with compatible non-AF control groups, necessitating the use of external controls. Such studies can have disparate characteristics and lack randomisation, introducing bias and heterogeneity in the study. The generalisability of the findings may be impacted, and the use of terms like "healthy" or "normal" for control groups may have included individuals with AF, potentially contaminating the control group.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
