
Research Article | DOI: https://doi.org/10.31579/2690-4861/898
1Forensic Psychiatric Center Mesdag, Helperlinie 2, 9722 AZ, Groningen, The Netherlands.
2Molde University College, Molde, Norway.
3Centre for Research & Education in Forensic Psychiatry, Oslo University Hospital, Norway.
*Corresponding Author: Jelle R. Lettinga, Forensic Psychiatric Center Mesdag, Helperlinie 2, 9722 AZ, Groningen, The Netherlands.
Citation: Jelle R. Lettinga, Herre W. Heetla, Frans A.J. Fluttert, (2025), Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry, International Journal of Clinical Case Reports and Reviews, 28(1); DOI:10.31579/2690-4861/898
Copyright: © 2025, Jelle R. Lettinga. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 June 2025 | Accepted: 16 July 2025 | Published: 24 July 2025
Keywords: single-case study; aggression management; clozapine treatment
Background
Aggression remains a significant challenge in forensic psychiatry, yet its treatment is insufficiently researched due to practical and ethical constraints. While atypical antipsychotics are commonly used to treat aggression, clozapine has demonstrated enhanced efficacy in managing aggression across various psychiatric disorders. However, studies focusing on clozapine's effectiveness in forensic populations are limited.
Objectives
This research employs a retrospective multiple single-case design to investigate the impact of clozapine on aggression, testing the hypothesis that clozapine would reduce both impulsive and psychotic aggression.
Materials and Methods
Seven patients with severe aggression were studied. Clozapine treatment commenced at 12.5 mg, gradually increasing to 300 mg over two to four weeks, with individualized adjustments based on blood levels, therapeutic effects, and side effects. The first prescription date marked the start of treatment. Measurements were conducted at least two weeks prior to initiating clozapine treatment and continued for a minimum of eight weeks thereafter, extending up to 16 weeks or until patient transfer. Aggression levels were assessed using the Brøset Violence Checklist [BVC] risk assessment instrument. BVC scores were pooled and averaged weekly.
Results
Results indicated a positive response to clozapine in four out of five patients with psychotic aggression, while those with impulsive aggression did not show similar improvements.
Conclusion
The findings from this study suggest that clozapine may be a promising treatment option for managing aggression in forensic psychiatric populations, particularly for those exhibiting severe impulsive and psychotic aggression.
Inpatient aggression represents a significant challenge within mental health care facilities, leading to feelings of unsafety and fear among staff and patients, along with increased resort to coercive measures [1-5]. Defined as intentional behaviors aimed at causing harm or injury to another person or object, aggression can be categorized into impulsive, psychotic, and predatory types [6-9]. Both psychotic and impulsive aggression are hypothesized to emerge from excessive reactivity to perceived threats, driven by inadequate top-down inhibitory control from the frontal cortex over the impulsive drives of the limbic system and amygdala [10].
If a common biological pathway exists for psychotic and impulsive aggression, this suggests that treatment may need to address aggression as an isolated symptom rather than solely as a function of specific psychiatric diagnoses. Challenges in ascertaining the prevalence of inpatient aggression in forensic settings stem from variability in definitions and methodologies [11], yet there is evidence that coercion in response to aggression is widespread [12].
While antipsychotics are frequently employed to mitigate aggression, their effects are often modest [13]. Clozapine, however, has demonstrated superior efficacy compared to other antipsychotics in managing aggression across various psychiatric disorders [14,15]. It is widely accepted that clozapine’s anti-aggressive properties are distinct from its antipsychotic effects, particularly in patients with schizophrenia, where it is recommended for those exhibiting persistent violence [16,17].
Studies have observed that clozapine’s anti-aggressive effects exceed its antipsychotic effects [18]. This finding has been confirmed in large clinical trials, which have also demonstrated the superior efficacy of clozapine in reducing aggression [19]. Furthermore, evidence suggests that the anti-aggressive properties of clozapine cannot be attributed solely to sedation [20-22] and may instead represent a primary pharmacological effect.
Furthermore, clozapine has proven effective in managing aggression across multiple diagnostic groups, including borderline personality disorder, autism spectrum disorders, intellectual disability, bipolar disorder, and dementia [23-30].
Despite its potential effectiveness, studies exploring the impact of clozapine on aggression within forensic mental health settings are scarce [20,31-33)]. Noteworthy findings include a retrospective analysis indicating significant reductions in aggression in treatment-refractory patients not diagnosed with schizophrenia [34], as well as studies demonstrating clozapine’s efficacy in forensic populations, such as patients with antisocial personality disorder [35] and court-ordered individuals [20]. Additionally, clozapine has shown a clinical and scientific significant reduction in violent re-offenses in patients with schizophrenia compared to olanzapine [36].
In conclusion, although clozapine is recognized as an effective yet underutilized treatment for aggression [37], there exists a significant gap in research regarding its effects on inpatient aggression, particularly in forensic settings where such behaviors are prevalent. Therefore, this study aims to study the effect of clozapine in treating impulsive and/or psychotic transdiagnostic aggression.
2. Material and Methods
2.1. Design
This study employed a retrospective multiple single-case pre-post design, utilizing an intention-to-treat approach.
2.2. Subjects and Setting
The study population comprises male patients residing in a high-security forensic psychiatric hospital in the Netherlands, which has 260 high-security beds. Inclusion criteria were: patients admitted between July 2018 and July 2019 who were treated with clozapine for psychotic or impulsive aggression. Aggression classification was performed by the treating psychiatrists (JL or HH). Eligibility for clozapine treatment required patients to have exhibited insufficient responses to at least two different antipsychotic medications at appropriate doses, in accordance with Dutch clozapine and TRIPP guidelines [38,39].
2.3. Procedure and Data Collection
Aggression levels were assessed using the Brøset Violence Checklist (BVC), a risk assessment tool comprising six items: Confused, Irritable, Boisterous, Physically threatening, Verbally threatening, and Attacking objects [40]. Each item was scored for presence or absence of the assessed item, with the BVC score reflecting the likelihood of aggressive behavior. Applying the BVC allows to assess risk before facing actual aggressive behaviors, which is a core aim in forensic treatment.
Measurements were conducted at least two weeks prior to initiating clozapine treatment and continued for a minimum of eight weeks thereafter, extending up to 16 weeks or until patient transfer. BVC scores were pooled and averaged weekly [40]. Clozapine treatment commenced at 12.5 mg, gradually increasing to 300 mg over two to four weeks, with individualized adjustments based on blood levels, therapeutic effects, and side effects [38,39]. The first prescription date marked the start of treatment. Concurrent medications, including other antipsychotics, were permitted, and medication adherence was monitored through blood levels and direct observation by the nursing staff. Table 2 shows the clozapine maximum dose and corresponding blood levels. Medical records were reviewed by the treating psychiatrist or psychologist to extract patient data, with participants assigned study numbers and analyzed within five-year age categories (e.g., 21-25).
2.4. Analysis
Based on clinical experience, the anti-aggressive effects of clozapine typically manifest within one week, which informed the decision to include data scores in the analyses only after this one-week threshold. Data analysis utilized simulation modeling analyses (SMA) as described by Borckardt and Nash [41]. Weekly mean BVC scores were calculated for each patient before and after clozapine treatment, provided sufficient measurements were available for both periods. A bootstrap sample of 5,000 cases per patient was generated to simulate a database of 5,000 measurements. The Pearson's r effect size for each case was compared with the simulated distribution of autocorrelations. This level change test evaluated the extent of BVC score alterations before and after clozapine initiation, controlling for score autocorrelation. A one-sample binomial test was conducted to assess whether the proportion of patients showing reduced BVC scores after clozapine treatment significantly differed from chance (50%), with p-values indicating treatment success. Clozapine treatment was defined dichotomously (yes or no), despite variations in prescribed dosages.
2.5. Ethics
The study protocol received approval from the local medical ethics committee and was conducted in accordance with Dutch and European legislation.
The study included seven patients (see Subjects and Settings), of whom one was not classified as exhibiting psychotic symptoms (see Table 1: Patient Characteristics). Among the participants, two patients (C and F) displayed impulsive aggression, while five demonstrated psychotic aggression [9]. All patients had been convicted of aggressive crimes. In Table 2, the maximum clozapine doses and corresponding blood levels for each patient are presented: Dose in mg/day and blood level in nanogram per milliliter. The overall results can be found in Table 3 "BVC Results". It is important to note that these results reflect the clinical findings from the BVC assessments conducted prior to the bootstrap analyses, and they include additional information regarding relevant co-medications.
The final and core analysis involved the bootstrap analysis, graphically represented in Figure 1 (Simulation BVC Results). The red line marks the start of the clozapine treatment, the black line reflects the BVC measures and the grey horizontal line the mean of BVC scores. The level change test indicated that all but one patient (F) experienced a reduction in aggression, with patients A and B showing significant decreases. Although not statistically significant, the visual data in Figure 1 suggest that patients D and E also exhibited reductions in assessed aggression, while patient F showed an increase. Patient G displayed neither statistical nor visual changes in assessed aggression.
| Patient | age | main DSM-5 classifications | subtype of aggression | crime category |
| A | 41-45 | schizophrenia, antisocial personality disorder | psychotic | Assault |
| B | 46-50 | schizophrenia, antisocial personality disorder | psychotic | severe assault |
| C | 21-25 | autism spectrum disorder | impulsive | severe assault |
| D | 36-40 | autism spectrum disorder, psychotic disorder, antisocial personality disorder | psychotic | Attempting manslaughter |
| E | 26-30 | schizophrenia, antisocial personality disorder | psychotic | severe assault |
| F | 31-35 | autism spectrum disorder, schizophrenia spectrum disorder | impulsive | Life threatening violence |
| G | 41-45 | schizophrenia, autism spectrum disorder | psychotic | severe assault |
Table 1: Patient characteristics.
| Patient | maximum dose [mg/day] | maximum blood level nanogram/ml |
| A | 800 | 314 |
| B | 900 | 664 |
| C | 300 | 591 |
| D | 300 | 282 |
| E | 300 | 248 |
| F | 450 | 396 |
| G | 600 | 400 |
Table 2: clozapine maximum dose and corresponding blood levels.
| Patient | Number of BVC scores | BVC average before clozapine | BVC average after clozapine | Relevant co-medication |
| A | n=31 | 883(N=17) | 159(N=14) | flupenthixole 200mg/4 weeks intramuscular |
| B | n=18 | 625(N=4) | 195(N=14) | bromperidole 200mg/4 weeks intramuscular |
| C | n=10 | 625(N=4) | 195(N=6) | risperidone 100 mg/4 weeks intramuscular |
| D | n=10 | 1,006(N=3) | 314(N=7) | paliperidone 50mg/4 weeks intramuscular |
| E | n=6 | 341(N=3) | 025(N=3) | paliperidone 150 mg/3 weeks |
| F | n=21 | 509(N=15) | 446(N=6) | olanzapine 20 mg dd, slowly tapered off, stop after 16 days |
| G | n=16 | 479(N=2) | 279(N=14) | haloperidol 5 mg daily |
Table 3: BVC results and co-medication
| Patients main symptom | Weekly averaged BVC Scores |
Graphic result | Level change R |
Patiënt A psychotic
|
n = 31 |  | R -0,654
P= 0,006*
|
Patiënt B psychotic
|
n = 18 |  | R -,515
P= 0,050* |
Patiënt C impulsive |
n = 10 |  | R -0,028
P= 0,909 |
Patiënt D psychotic |
n = 10 |  | R -,526
P= 0,323 |
Patiënt E psychotic |
n = 6 | 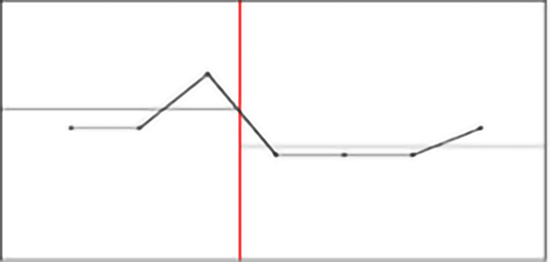 | R -0,708 P= 0,069 |
Patiënt F impulsive |
n = 21 |  | R 0,149 P= 0,575 |
Patiënt G psychotic |
n = 16 |  | R -,319 P= 0,281 |
Figure 1: BVC Results
Note: SMA and Test Level Change in BVC before and after start of clozapine.
* P<0>
This study evaluated the efficacy of clozapine in reducing predicted aggression within a small cohort of involuntarily admitted patients at a high-security forensic psychiatric hospital in the Netherlands. Data were analyzed on a single-case basis. The findings suggest that clozapine was associated with a decreased likelihood of aggression, as indicated by the Brøset Violence Checklist (BVC), specifically in patients with a history of psychotic aggression, except for one patient who exhibited no change. Conversely, this effect was not observed in patients diagnosed with impulsive aggression.
The efficacy of clozapine on aggression has been documented in other forensic contexts, aligning with existing literature that supports its effectiveness in managing psychotic aggression [22]. Most of the evidence, including data from randomized controlled trials, supports the use of clozapine as a maintenance treatment for persistent aggressive behavior in patients with schizophrenia. Moreover, it is suggested that the anti-aggressive effects of clozapine may operate independently of its antipsychotic properties, such as the treatment of hallucinations and delusions [23, 24] and the treatment of patients with personality disorders and severe aggression [25]. However, it is noteworthy that this study found no reduction in aggression among the two patients with impulsive aggression, particularly since both were diagnosed with autism spectrum disorder, a condition in which clozapine is known to be effective against aggression.
This multiple single-case study demonstrates the feasibility of assessing the effects of an intervention in a small, often challenging-to-study patient population. Furthermore, it highlights the potential for meaningful statistical analysis at the individual level, which is particularly valuable in forensic psychiatry and other specialized research domains with limited sample sizes.
In future research, this methodology may facilitate the identification of patient subgroups that respond favorably to specific interventions, such as clozapine for aggression. Moreover, it could help guide clinical decisions regarding the continuation or discontinuation of clozapine treatment based on individual patient responses.
The amygdala is crucial for threat perception and has been found to be hyperactive in cases of impulsive aggression [10,45]. It is modulated by several prefrontal brain regions, including the prefrontal cortex (PFC), dorsolateral prefrontal cortex (DLPFC), orbitofrontal cortex (OFC), and ventromedial prefrontal cortex (VMPFC) [43]. Neuroimaging studies indicate impaired connectivity between the PFC and amygdala in individuals exhibiting impulsive aggression [45,47,48].
In healthy individuals with psychopathic traits, the impulsive-antisocial dimension has been positively correlated with presynaptic dopamine release capacity in the nucleus accumbens (NAcc) and NAcc activity during monetary reward anticipation. This suggests that excessive NAcc function may underlie impulsive aggression, a component of impulsive antisociality [49]. Deep brain stimulation of the NAcc has been shown to substantially reduce aggression in patients with various conditions, including Tourette syndrome, obsessive-compulsive disorder, autism, cerebral palsy, encephalitis, and epilepsy [50,51].
The current hypothesis regarding neurotransmitter involvement in impulsive and psychotic aggression suggests an imbalance between dopamine and serotonin. Specifically, serotonin levels appear decreased in the prefrontal cortex, while dopamine levels are elevated [10,46]. Antagonism of the 5-HT2A receptor has been found to enhance OFC-amygdala connectivity [52]. Clozapine is a potent antagonist of the 5-HT2A, 2B, and 2C receptors with a relatively weak D2 dopamine blockade. It has been shown to increase dopamine release in the prefrontal cortex [53,54]. This release in the prefrontal cortex may locally decrease dopamine release in the mesolimbic system [54,55]. These effects on dopamine and serotonin may enhance the frontal cortex's regulatory control over the NAcc, thereby reducing aggression.
Additionally, the glutamatergic system has been proposed as a potential target for aggression treatment [56]. Clozapine has been shown to increase NMDA receptor-mediated glutamate output [57], and in treatment-resistant schizophrenia, it has been found to restore glutamatergic neuron function [58]. These findings are pertinent as glutamatergic enhancement can exacerbate aggression, and a glutamatergic/GABAergic imbalance can contribute to ‘hyperactivity in subcortical limbic regions [10]. The glutamatergic effect of clozapine is notable compared to other antipsychotics.
Strengths, limitations and Weaknesses
There is skepticism regarding the utility of randomized trials in clinical practice, particularly in forensic psychiatry, where informed consent can be challenging to obtain and coercion is often employed in cases of severe aggression [59]. One advantage of single-case studies is their feasibility in demonstrating clinical relevance, particularly for difficult-to-study cases. However, to generalize findings, a larger number of N = 1 studies are required, especially since the impulsive aggression cases in this study did not align with the expected outcomes in the literature.
The study described has limitations that could impact the validity and generalizability of its findings. The retrospective design relying on existing records may lack completeness or detail. This could introduce bias. A major issue regarding real world studies is placebo effect. Since it is not feasible to prescribe placebo in real world studies is is impossible to measure the size of placebo effect. The multiple single-case pre-post design may not provide sufficient power to detect statistically significant changes, particularly due to the small number of cases or variability in individual responses to treatment. Since the study does not describe randomization, the sample could be subject to selection bias. The characteristics of patients who received clozapine may differ from those who did not, confounding the outcomes. Individualized adjustments to clozapine dosage may lead to variability in treatment exposure, complicating the assessment of dosage effects on aggression levels. The reliance on medical records for data extraction may lead to incomplete or biased information, depending on the rigor and consistency of data entry in the clinical setting. Overall, while the study may provide important insights, these limitations should be considered when interpreting its results and implications for clinical practice.
The weakness of the study is its aiming to approximate real-world conditions; however, it did not yield real-world results. Factors beyond pharmacological treatments that could influence aggression were not included in the analysis. The allowance of other antipsychotics could confound the effects of clozapine, making it difficult to isolate its specific impact on aggression. Additionally, the BVC is primarily a predictive tool for aggression rather than a direct measure, making it suitable for clinical use but less optimal for research purposes. Although this study extensively measured clozapine's effects on predicted aggression, improvements in other psychiatric conditions were not evaluated. Clozapine has been shown to reduce aggression independent of psychosis, but this study could not quantify such effects.
The outcome of the study primarily reflected estimated aggression through BVC scores. We acknowledge that the most accurate measure of aggression would involve direct observation of aggressive incidents; however, during the study window, no such incidents occurred. Thus, the use of BVC as a recognized predictive instrument represents the next best option to gauge clozapine's anti-aggressive effects.
The findings from this study suggest that clozapine may be a promising treatment option for managing aggression in forensic psychiatric populations, particularly for those exhibiting severe impulsive and psychotic aggression. Despite the limited sample size and the retrospective nature of the design, the trend towards reduced aggression levels, as measured by the Brøset Violence Checklist (BVC), indicates that clozapine could be an effective intervention for patients with significant behavioral challenges.
Further research with larger, controlled studies is warranted to validate these findings and to explore the specific mechanisms through which clozapine exerts its effects on aggression.
Jelle R. Lettinga: Conceptualization, Writing – original draft. Cecilia Karr: Methodology, Formal analysis, Investigation, Data curation, Visualization. Herre W. Heetla: Conceptualization, Investigation, Writing – review & editing. Frans A.J. Fluttert: Resources, Data curation, Writing - review & editing, Supervision
The author confirms that the data (transcriptions of the interviews) supporting the findings of this study, these are available by request to main author.
The authors have declared that there are no conflicts of interest in relation to the subject of this study.
We thank Dr. Marinus Spreen for his advice on the design and statistical analysis. And we thank Cecilia Karr for performing the statistical analysis.
We thank Forensic Psychiatric Center Mesdag for the final financial contribution leading to this publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
