
Research Article | DOI: https://doi.org/10.31579/2766-2314/098
1 ICMR-Vector Control Research Centre Field Unit, Near hati line, Koraput, Odisha, India.
2 ICMR-Vector Control Research Centre, Medical Complex, Indira Nagar, Puducherry, India.
*Corresponding Author: A. N. Shriram, ICMR-Vector Control Research Centre, Medical Complex, Indira Nagar, Puducherry, India.
Citation: Dilip K. Panigrahi, A. N. Shriram, Mustafa Baig, B. Vijaya Kumar, Ashwani Kumar, (2023), Exploring Barriers of Adherence to Artemisinin- Based Combination Therapy (Act) With One Day Primaquine Treatment for Plasmodium Falciparum Malaria and Compliance to Vector Control Among Marginalized Tribal Communities in East Central India, J, Biotechnology and Bioprocessing, 4(2); DOI:10.31579/2766-2314/098
Copyright: © 2023, A. N. Shriram. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 March 2023 | Accepted: 04 April 2023 | Published: 14 April 2023
Keywords: malaria; ACT; adherence; LLIN; IRS; traditional medicine; primaquine; tribes; resistance
Background: Artemisinin Based Combination Therapy (ACT) compounds, have been observed to produce rapid therapeutic response, introduced over the past few years against chloroquine resistant Plasmodium falciparum. In India, malaria treatment by Accredited Social Health Activists (ASHAs) in remote and tribal villages has expanded the use of ACTs for the management of uncomplicated malaria. To maximize its effectiveness, patients’ adherence to the treatment regimen is central. Measures should therefore be taken to ensure and monitor the use of ACT to avoid the emergence of resistance/treatment failure. The present study assessed the level of adherence to ACT treatment, including the respondents’ compliance to vector control interventions.
Methods: The research team visited the houses of pre-diagnosed P. falciparum infected malaria patients, treated by the Community Health Centers with ACT plus primaquine, on the 4th day post treatment. Adherence to the drug regimen was observed on the spot and the patients were interviewed using a semi-structured questionnaire on malaria and their compliance to the ongoing vector control intervention. Rapid diagnostic tests and peripheral blood smear collection were conducted to ascertain whether the patient was cleared of parasitemia post treatment.
Results: 76.5% of the patients were found adhering to the drug regimen. Over 80% of the respondents informed mosquito that bite was one of the causes of malaria and felt it is a serious disease. Only 0.7% of the respondents preferred traditional to ACT medicines for malaria treatment. Lack of space, damaged nets, and use of mosquito repellents were the major reasons of the non-usage of Insecticide-Treated Nets (ITNs). Only 1.6% of the respondents had permitted for indoor residual spray (IRS) in all rooms of their houses. 27.3% of the respondents had permitted spraying their houses partially.
Conclusion: Too many tablets was the major reason for non-adherence to the ACT regimen. Strengthening information, education, and communication/behaviour change communication could enhance drug adherence, improving LLIN use rate, and acceptance to IRS. One of the important take away from the current study was the paradigm shift in preference to ACT from traditional medicines for malaria treatment.
Plasmodium falciparum contributes 97% of the malaria incidence globally. Control of malaria relies on vector-control interventions such as Insecticide-Treated Nets (ITNs) and indoor residual spray (IRS) of insecticides, and antimalarial drugs due to nonavailability of an effective vaccine [1]. India recorded 50.7% (n=338,494 cases) of the malaria cases in the South-East Asia region (n= 667916 cases) and 46% of them are due to P. falciparum during 2019 [2]. The emergence of resistance and subsequent treatment failure against Plasmodium falciparum infection, has limited the use of Chloroquine (CQ) which was used as the first-line treatment for malaria in developing countries. Factors like incorrect dosing, non-compliance with the duration of the dosing regimen, poor drug quality, and drug interaction could have been contributing factors to chloroquine treatment failures [3]. A new group of antimalarials, the Artemisinin Based Combination Therapy (ACT) compounds, have been observed to produce a rapid therapeutic response was introduced during the past eleven years against CQ resistant Plasmodium falciparum [4]. The World Health Organization (WHO) currently recommends six ACTs: artemether-lumefantrine (AL), artesunate-amodiaquine (AS-AQ), artesunate-mefloquine (AS-MQ), artesunate-pyronaridine (AS-PND), artesunate-sulfadoxine/pyrimethamine (AS-SP), and dihydro-artemisinin-piperaquine (DHA-PPQ) [5]. The role of the artemisinin compound is to reduce the parasite load rapidly during the first days of treatment while the role of the partner drug is to eliminate any remaining parasites. [6]. In line with WHO recommendations, nearly all high-burden South East Asian countries including India have moved from chloroquine to ACTs as the first-line treatment of uncomplicated P.falciparum malaria. For the first-line treatment of falciparum malaria, by 2012, 79 out of 88 endemic countries adopted ACT [7] and is proven to be cost effective for malaria treatment [8].
WHO acknowledges the fact that rational use of antimalarial medicines is critical; it suggests that resistance to the ACTs could have a negative impact on national malaria control programmes [9]. Thus, incomplete elimination of parasites exposes the patient to recurrent malaria attacks increasing mortality and health care costs [10]. At the community level, it leads to the development of parasite resistance, precipitating malaria morbidity and mortality [10]. Poor adherence to anti-malaria medications could play a role in the future development of drug resistance. As such, identifying ways to improve anti-malarial compliance will help mitigate drug resistance [11].
However, there is a wide variation among the estimates of treatment adherence [12, 13]. It varies from 1.5% to 100
Study area
The study was carried out in 2 malarias endemic CHCs (Bandhugaon and Narayanpatna) of Koraput district, Odisha State, India. Malaria data for the past 5 years is furnished in table 1.

Table 1: CHC wise malaria data (API) of Koraput district, Odisha State.
Koraput district (18o13’ and 19o10’N and 82o5’ and 83o13’E) is situated in the southern part of Odisha, bordered by states of Andhra Pradesh on the eastern side and Chhattisgarh on the Western side. The district spans an area of 8807sq km (Figure 1). Many rivulets crisscross the valley and joins the larger rivers, Bansadhara and Kolab. The district has 2028 revenue villages and is inhabited by about 1.4 million population, of which 50% are constituted by the local tribes. The district is home to 13 tribes among them Kondhs, Ghadavas and Parajas are primitive. These tribes reside in huts in small hamlets / clusters located on hilltops and foothills. The literacy rate is 35.72%. The majority of the villagers are agricultural labourers and marginal farmers. During summer, villagers go to the forest and collect forest products, that include timber, firewood, bamboo, kendu leaf, sal leaf, Mohul flowers/fruit, etc. During rainy and winter seasons most of them work as agricultural labourers away from their homes on a daily wage. Lack of basic infrastructure (communication, transport, roads and paths) makes it difficult to reach village in quicktime. (Source: District hand book, Koraput, 2009), Among the 14 CHCs of Koraput district, Narayanapatna and Bandhugaon CHCs were severely affected by malaria, that was contributing >60% of the P. falciparum cases (Figure 2), over past several decades (Source: CDMO Office, Koraput). Therefore, we thought it worthwhile to conductthe study in these two Community Health Centre (CHCs).
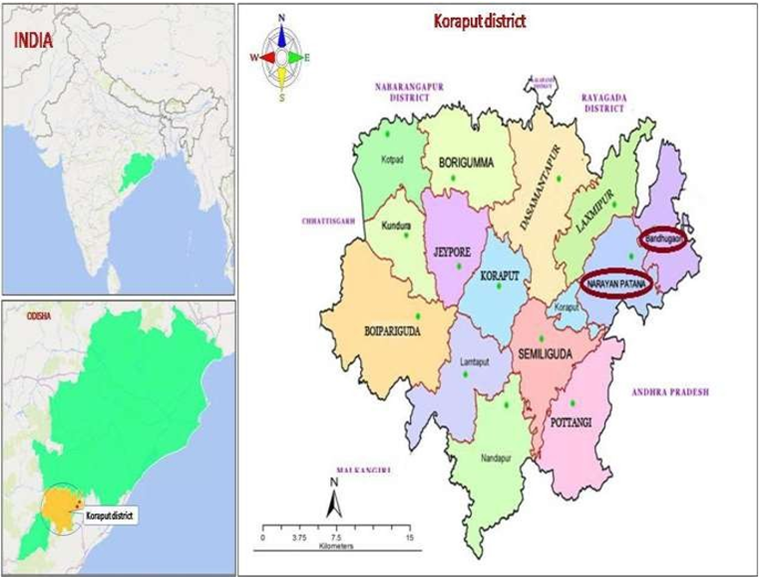
Figure 1: Map showing study area.
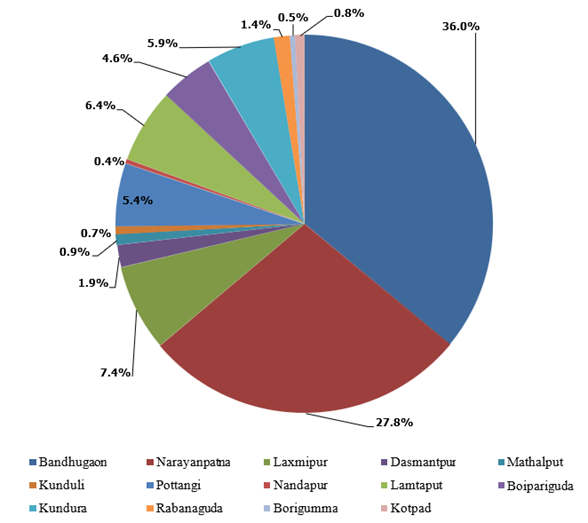
Figure 2: Percentage of API in different CHCs of Koraput district in 2020. (Source: CDMO Office, Koraput)
Narayanpatna CHC spans an area of about 726 sq. km with a population of 53015, of which 85.1% are tribes. There are 13 sub-centres (210 revenue villages) in this CHC. The distance between CHC and different villages ranges from 1-35 kms. Bandhugaon CHC is in contiguous to Andhra Pradesh in the east and Chhattisgarh to the western side spanning an area of 425 sq. km. The CHC comprises of 10 sub-centres (SCs) (166 villages) with a population of 68,698 predominantly constituted by several tribal communities (77%), the majority being Kondh (Table 2).

Table 2: Demographic details of the study CHCs.
Field survey
Malaria patients who were diagnosed and treated for P. falciparum infection with ACT (Artesunate with sulfadoxine and pyrimethamine) plus primaquine in these CHCs from January’22 toDecember’22 was eligible for the study. It was expected that; the patients would have consumed all the tablets present in the blister packets as per the instructions given by the health facility within 3 days. On the fourth day of post treatment, research team visited the patients’ home and interviewed them using a semi-structured interview questionnaire which was designed for a face-to-face interview with the patient in the local language i.e., Odiya. Caregiver or head of the family was interviewed if the patient was below 17 years of age. Written informed consent was obtained for interviewing the participants. A written copy of the information was provided to the participants.
For considering the level of adherence (like following the drug consumption instructions by the drug supplier, elimination of parasites after treatment), the patients were sub-grouped into the following four categories
Arrangements were made to treat him/her again to eliminate parasites from his/her blood for the patients who were found positive by RDT or microscopic testing. Patients who were found to have taken any treatment from traditional healers for malaria in addition to the treatment given by the CHC were also recorded. ITNs usage behaviour, maintenance practice and their perception on IRS were recorded by interviewing the head or any adult member of the 377 holdings from 115 randomly selected villages. Other information regarding demographic characteristics, socio-economic status, educational background, and geographical location of the patients were captured in a pre-designed data capture format.
The following information was collected from falciparum infected patients.
Patients who were positive either after adhering to the drug schedule or not adhered, were again advised to take treatment from their respective ASHAs were having advised to contact the concerned CHC for retreatment.
In total 400 falciparum infected malaria patients were included to estimate adherence to treatment. The sample size was determined with the assumption of percentage of treatment adherence is 50%, 5% of absolute precision and 95% confidence interval.
Where, n is the sample size
The patients’ household was included to estimate the compliance to vector control intervention measures in the community.
Statistical analysis was carried out using logistic regression analysis to find out the risk factors of non-adherence to medicines and p-value less than 0.05 was considered to be significant. All statistical analysis was done by STATA 14.2 (Texas, USA).
Overall, 400 patients (218-Males and 182-Females) from 377 holdings were interviewed in 115 villages from both CHCs. 1653 members were present in 377 human dwelling. Out of the 400patients interviewed, 232 (58.0percentage) patients were below 17 years of age. These 232 patients were present in 214 houses and the head of these houses were considered as caregivers and interviewed.
The age categories of the patients are furnished in table 3. Most of the surveyed houses (76.4%) were found to be made of mud walls with tiled roof/thatched roofs followed by reinforced cement concrete (RCC) buildings (19.1%), and cement walls with tiled roof/thatched roofs (4.5%).

Table 3: Age distribution of participants.
Details of Caregivers
The mean age (SD) of the caregivers was found to be 34.50 (6.01), ranging from 22 to 55 years. The majority of the caregivers (119;54.3%) were found to be looking after 2 children who were below 17 years of age (Table 4). Out of 219 caregivers 97.6% were ST followed by SC. (1.4%) and general (0.9%).
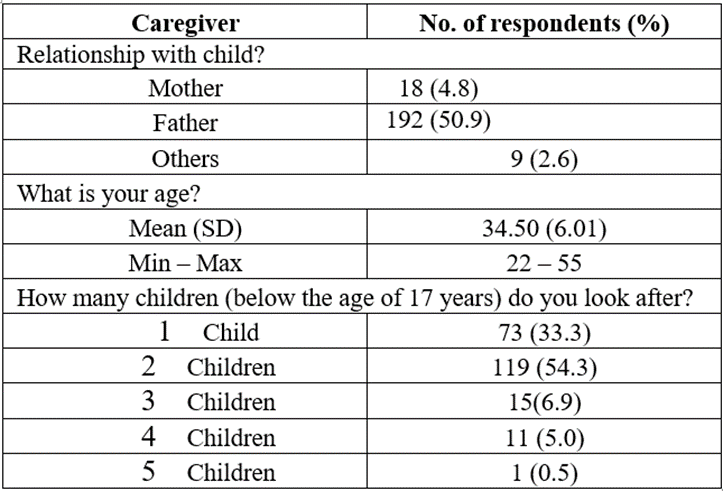
Table 4: Details of caregivers interviewed.
Respondents’ knowledge on malaria
Responding to the question “how do people get malaria”, 308 (81.7%) respondents out of 377 told, it was due to mosquito bites combined with other causes like unclean water/ stale food and bad air, while 61 (16.2%) respondents told it was solely due to mosquito bite, 59 (1.3%) respondents told was of unclean water and only 3 (0.8%) respondents told they had no idea. On their practice of using traditional medicines given by local healers (Disharis), only 3 (0.7%)persons said that they had used traditional medicine but subsequently they had also taken Government supply medicines from CHC and got cured. Only one patient said that he was not cured even after using antimalarials supplied by CHC. (Table 5).

Table 5: Respondents knowledge and practices on malaria
Treatment seeking behavior
All of 377 respondents said that they had asked the drug dispenser about drug schedule and 371 (98.4) persons out of them told that the drug dispenser had explained them as how to consume the medicines by showing them the blister pack. The other 6 respondents said that the drug dispenser had told them verbally, how to consume the tablets (Table 6).

Table 6: Treatment seeking behavior of the patients/caregivers
Adherence to ACT and PQ treatment
Out of the 400 patients surveyed 306 (76.5%) patients had adhered to the drug schedule. This was confirmed by the team by showing them the blister packets and asking them how they have consumed the tablets. Even 42 members showed the empty blister packets present with them.
Out of 94 non-adhered patients, 27 (28.7%) including caregivers of 10 patients below 17 years of age could not tell any reason, why they have not adhered to the drug schedule. Whereas, 2 (2.1%) patients told it was due to the bad taste of the tablets, 1(1.1%) patient said that it was because of the bigger size of the tablets, while 64 (68.1%) told it was because of a greater number of tablets (Table 7). When asked about the experience of any adverse effects of the drugs, out of 400 patients, 37 patients said that they had experienced vomiting, headache, and weakness after consuming the drugs.

Table 7: Response on “causes of non-adherence to 3 days ACT and PQ treatment”
When the research team asked the patients, possible reasons for non-consumption of the tablets by the villagers, 338 (89.6%) respondents said that they had no idea about this while 36 (9.5%) respondents said that this was due to a greater number of tablets, 1 (0.3%) respondent felt it was due to of adverse effects of the medicine, 1 (0.3%) respondent told, it was because of the size of the tablets and 1 (0.3%) respondent told it happened just because of negligence.
Compliance to vector control intervention measures
Insecticide Treated Net (ITNs)
ITN’s were distributed twice in this area (2017 and 2020). The survey showed that a total of 989 LLINs were distributed to cover 1653 members of the surveyed 377 holdings (1.7 persons per net).
It was observed that 120 (31.8%) holdings had not used the net during the previous night of the surveyed day, whereas 257 (68.2%) holdings were using at least one of their received nets. When asked “why they are not using all of their received nets”, 120 respondents could not give any answer (negligence). Twenty-six respondents told they have lack of space in their house to tie all of the received nets. Twenty-one respondents told some of their nets were damaged. Twelve respondents told they have washed the nets and are wet now. Nine respondents told they use mosquito repellents. Six respondents told they do not use it because of hot climatic conditions. One respondent said that he lost his net (Table 8).

While asking about the general habit of using LLINs, all of 377 respondents told that they do not use the LLINs regularly 191 (56.7%) respondents told they do not use the nets in hot/cold climates, 56 (16.6%) respondent did not answer anything (negligence) while 36 (10.7%) respondents told that their nets were damaged, 28 (8.3%) respondents told they use repellent/fan to avoid mosquito bites, 22 (6.5%) respondents told lack of space in their house to tie the nets, 3 (0.9%) respondents told the received nets are insufficient for their family while 1 (0.3%) respondent told he had experienced itching while using the net (Table 9).

Table 9: Response of the respondents on irregular use of LLIN.
Washing practices of LLINs
Out of 377 respondents, 370 (98.1%) told that they wash their LLINs in streams/ponds while 7 (1.9%) respondents told, they wash the LLINs in their home/near bore well. None of the holding members said that they washed their nets with warm or hot water. Only 15 respondents said that they dry their LLINs under shade after washing (Table 10).
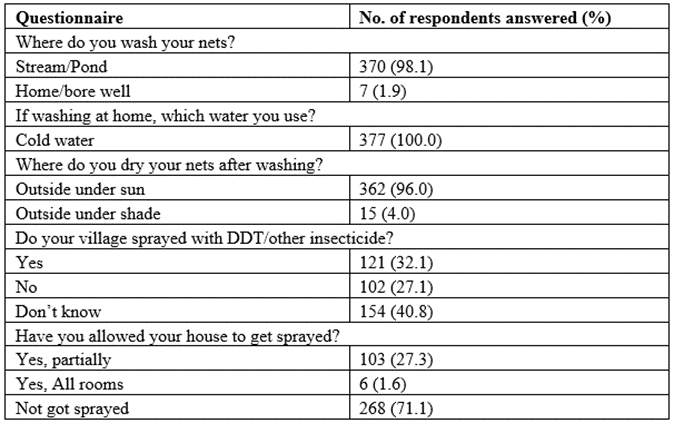
Table 10: Response of the respondents on washing practices of LLINs and IRS in their villages
Compliance to Indoor Residual Spraying
When asked “whether your village has been sprayed with DDT”, 102 (27.1%) heads of holdings answered “no” while 154 (40.8%) respondents said that they did not know whether their village had been sprayed or not, while 121 (32.1) respondents told, they knew when their village had been sprayed. Out of 121 participants who knew about the visit of the IRS spraying team to their village, only 6 (1.6%) told that they had allowed spraying in all rooms of their respective house, 103 (27.3%) allowed the spray team to partially spray in their house (leaving Puja room, Kitchen room, and food grain storage room) (Table 11).
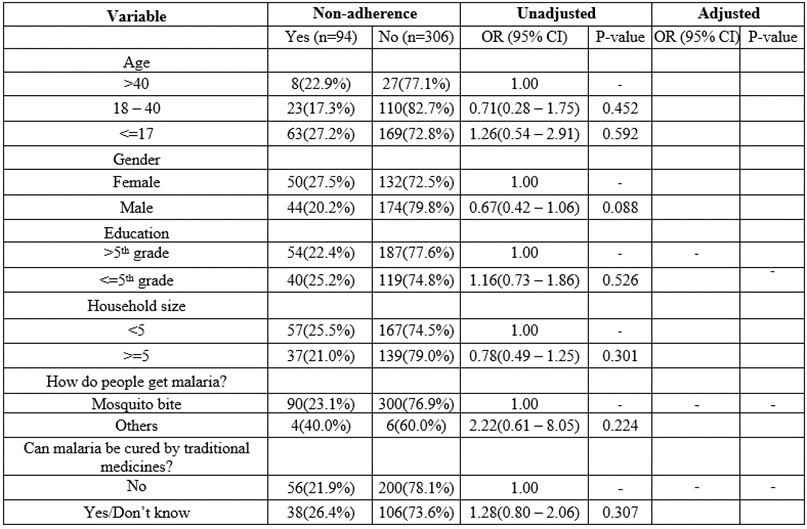
Table 11: Univariate logistic regression model for non-adherence of ACT
Level of adherence
Level of adherence showed that 306 patients are adhered to drug schedule and found negative for malaria parasite in microscopy and RDT and 94 patients are certainly non-adhered, if showing any remaining tablets.
Factors associated with non-adherence to 3 days malaria treatment
The statistical analysis using logistic regression analysis to find out the risk factors of non-adherence to medicines indicate that factors like age, education, knowledge on malaria could not be attributed to adherence to drug schedule. Only experience of discomfort (P=<0 xss=removed>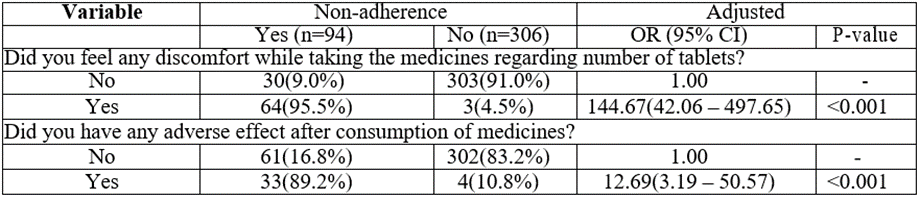
Table 12: Multiple logistic regression model for non-adherence of ACT
The present study was conducted to assess the level of adherence to 3 days treatment of ACT+PQ for P. falciparum infection. Kristin Banek et al. (2014) in his critical review on the subject, suggests that ACT adherence levels varied substantially between the study populations and comparison between studies was challenging due to differences in study design, definitions, and methods used to measure adherence [12]. A similar study conducted in the Amazon region of Brazil to know the level of adherence for P. vivax treatment had reported 86.4% of the patients adhered and 9.6% of the patients were in “certainly non-adhered category that showed the remaining tablets after completion of drug schedule regimen [24]. The present study showed 76.5% of patients adhered to the instructions while 23.5% showed the remaining tablets. Those patients who have not shown the remaining tablets had followed the 3 days drug schedule as per instructions. In Ghana, 36.6% of the patients were observed to have adhered to the treatment instructions. Surprisingly, >90% of the respondents had agreed that ACTs they consumed had bad taste and felt unpleasant [11]. While we observed, a miniscule proportion (2.1%) of the respondent’s experienced discomfort while consuming the ACTs in terms of unpleasant taste. This implies that with a robust and sustained IEC campaign, the perception of this miniscule proportionof individuals could be altered, paving way for completed compliance. This would pave way for elimination of malaria in the region and also prevent development of resistance to ACTs.
Alexandria et.al. (2015) documented reported 57.3

Figure 3: Treatment seeking behaviour of the participants
Non-adherence to malaria treatment would be participate in development of drug resistance. Non-adherence to ACT was primarily due to negligence of patients as after one or two days after consuming the medicines they were relieved from fever. The tribal patients preferred ACT over the traditional medicines for malaria treatment. In spite of the awareness that mosquito bites cause malaria, not using the LLINs poor maintenance and non-acceptance of IRS are most likely reasons for persistence of malaria in this area. People should be educated about the implications of poor adherence to ACT and at the same time they should be educated about the wastage of Government resources by not using the LLINs and non-acceptance to the IRS. Therefore, a robust information, education, and communication (IEC)/ behaviour change communication (BCC) mechanism shouldbe in place such a mechanism not only could enhance the compliance to ACT but also facilitate in decreasing the malaria cases coupled by creating awareness on LLIN use and IRS acceptance. For the future, further in-depth studies on individual factors and barriers associated with non-adherence to ACT are needed, to make informed policy choices and improve the drug delivery system for effective malaria treatment which would hasten the process and elimination of malaria.
ACT - Artemisinin-based combination therapy
ASHAs - Accredited Social Health Activists
CHC - Community Health Centre
ITNs - Insecticide treated nets
IRS - Indoor residual spraying
CQ - Chloroquine
PQ - Primaquine
WHO - World Health Organization
AL - Artemether-lumefantrine
AS-AQ - Artesunate-amodiaquine
AS-MQ - Artesunate-mefloquine
AS-PND - Artesunate-pyronaridine
AS-SP - Artesunate-sulfadoxine/pyrimethamine
PQ - primaquine
DHA-PPQ - Dihydroartemisinin-piperaquine
NCVBDC - National Centre for Vector Borne Disease Control
ASHA - Accredited Social Health Activists
ICMR-VCRC - Indian Council of Medical Research-Vector Control Research Centre
CDMO - Chief District Medical Officer
RDT - Rapid Diagnostic test
IHEC - Institutional Human Ethical Committee
RCC - Reinforced Cement Concrete
SD - Standard Deviation
SCs - Sub-centres
DDT - Dichlorodiphenyltrichloroethane
VBDTS - Vector Borne Disease Technical Supervisor
LT - Laboratory technician
IEC - Information, Education, and Communication
BCC - Behaviour change communication
Ethics approval and consent to participate:
Ethical permission for the research was sought and granted by the Institutional Human Ethical Committee (IHEC), ICMR-VCRC, Pondicherry. (IHEC-0421/N/N). Consent from all of the participants of this study was obtained at the time of survey.
All the authors involved in the study have given their consent to publish the manuscript.
Relevant data was obtained from the CHCs are available within the manuscript in the form of primary tables and graphs. Data is available on reasonable request to ICMR-VCRC.
The authors declare that they have no competing interests
This study was supported by internal funds of the ICMR-Vector Control Research Centre, Pondicherry, India.
DKP, ANS, AK Conceptualized the study design. DKP, MMB supervised the conduct of study. DKP & VK performed the curation of data and statistical analysis. DKP & ANS drafted and edited the original manuscript; AK critically reviewed the manuscript. All authors read and approved the final version of the manuscript.
The authors would like to thank Vector borne disease technical supervisors (VBDTS) Mr. Prakash Chandra Jena & Mr. Santosh Kumar Behera and laboratory technicians (LT) Mr. Rohiteswa Jena & Mr. Surendra Nath Choudhury of Bandhugaon and Narayanpatna CHCs respectively for providing malaria patients’ data and locating their houses in the villages.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
