
Research Article | DOI: https://doi.org/10.31579/2692-9392/159
1Radiology Department, Düzen Laboratories, Remzi Oğuz Arık Mh. Atatürk Blv. No:237/39. 06680, Kavaklıdere-Ankara/Turkey.
2Cardiovascular Surgery Department, Başkent University Alanya Medical Research and Training Hospital Address: Saray Mah. Yunus Emre Cad. No:1, PK 07400 Alanya-Antalya/Turkey.
*Corresponding Author: Aykut Kadıoğlu, Radiology Department, Düzen Laboratories, Remzi Oğuz Arık Mh. Atatürk Blv. No:237/39. 06680, Kavaklıdere-Ankara/Turkey.
Citation: Aykut Kadıoğlu and Ali Baran Budak, (2023) Evaluatıng the Impact of Great Saphenous Veın Reflux Pattern on Clınıcal Severıty and Treatment Modalıty. Archives of Medical Case Reports and Case Study, 7(1); DOI:10.31579/2692-9392/159
Copyright: © 2023 Aykut Kadıoğlu, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 November 2022 | Accepted: 22 December 2022 | Published: 06 January 2023
Keywords: saphenous vein; venous insufficiency; ultrasound; reflux; sclerotherapy; radiofrequency ablation; cyanoacrylate
Objectives:
This research aimed to determine the impact of reflux patterns in patients with great saphenous vein (GSV) insufficiency on clinical severity and management.
Methods:
We evaluated 771 lower extremities of 452 patients having GSV insufficiency with Doppler Ultrasound. We characterized the reflux patterns like previously done in the literature: type 1, GSV reflux without the involvement of perimalleolar region or saphenofemoral junction (SFJ); type 2, GSV reflux involving perimalleolar region; type 3, GSV reflux involving SFJ; type 4, GSV reflux involving both perimalleolar region and SFJ. Then we conducted a study to evaluate the relationship between GSV reflux type and age, gender, venous clinical severity score (VCSS), clinical, etiological, anatomical and pathophysiological elements (CEAP), body mass index (BMI) and gave an effort to compare the groups by therapeutic strategies.
Results:
The mean age was 44±11 years. The male-to-female ratio was 0.49. The most commonly observed reflux pattern was type 3 (48%) in patients with GSV insufficiency and varicose veins. Patients with type 1 reflux were younger, had lower BMI, and had a better clinical situation (p=0.002). VCSS was associated with perimalleolar region involvement, as increased in type 2 reflux than type 1, and higher VCSS was related to SFJ involvement as defined in type 3 reflux. Type 4 reflux patients had the highest VCSS that means the most severe clinical presentation. Sclerotherapy was the most common treatment modality in type 1 reflux (p<0.001). Also, in type 2 and type 4 reflux, sclerotherapy was more preferred than type 3 (p<0.001). Type 4 reflux pattern required mostly radiofrequency ablation, compared with type 3 (28.2% vs 20.5%; p<0.05) after initial diagnosis. Cyanoacrylate glue embolization was the appropriate therapeutic option in only 3.2% of type 4 reflux patients, which was significantly lower than type 3.
Conclusion:
According to the reflux pattern classification system based on SFJ and malleolar region involvement as practiced in this study, we described a correlation between VCSS, CEAP, BMI, and the extent of venous insufficiency. This correlation with consideration of cosmetic reasons and vein diameter measurements can suggest further treatment modality.
Advances in knowledge:
We investigated a practical, clinically applicable, and widely accepted standard method for classifying GSV insufficiency. Mapping venous insufficiency with such a system is essential to determine the clinical severity and the most appropriate treatment modality.
Abbreviations (respectively):
CVI: Chronic venous insufficiency
GSV: Great saphenous vein
SSV: Small saphenous vein
US: Ultrasonography
RFA: Radiofrequency thermal ablation
CGE: Cyanoacrylate glue embolization
BMI: Body mass index
CEAP: Clinical, etiological, anatomical, and pathophysiological elements
VCSS: Venous clinical severity score
SFJ: Saphenofemoral junctiontab
Varicosis of the lower extremities is a common condition that presents various symptoms such as pain, heaviness, swelling, night cramps, itching, and numbness. Chronic venous insufficiency (CVI) is associated with a consequential socioeconomic cost due to its high prevalence, cost of investigation, and treatment [1-3]. It usually originates from the superficial venous system. Great saphenous vein (GSV) failure accounts for the majority (82.7%) of superficial venous insufficiencies. Differently, small saphenous vein (SSV) failure constitutes a limited (10.9%) part [4]. Superficial venous insufficiency usually shows segmental involvement and progression [5]. However, based on Ultrasonography (US) mapping, a standardized and commonly used anatomical classification for superficial venous insufficiency has not been available yet.
Venous insufficiency mapping is crucial to determine an accurate treatment plan. The treatment's primary purpose is to relieve the complaints of patients, and to prevent future complications and recurrences, as well. Treatment options for CVI are evolving day by day. The current main treatment methods are surgery, sclerotherapy, thermal and non-thermal techniques [6]. Surgical treatment of varicose veins has been superior to conservative treatment [7]. High ligation and stripping have been the standard method in CVI treatment for half of the century. Despite its success, associated postoperative morbidity and delay in return to daily life concluded the development of less-invasive techniques [8]. Radiofrequency segmental thermal ablation (RFA) with excellent results, low complication rates, and a faster return to work recommended as the first-line treatment over surgery and foam sclerotherapy by the European Society of Vascular Surgery [8]. Nevertheless, the necessity of infiltration of tumescent anesthesia and potential side effects such as bruising and neurological complications like paresthesia due to saphenous nerve damage provided non-thermal techniques. Cyanoacrylate glue embolization (CGE) has been one of the non-thermal techniques. Unless any region with insufficiency is treated, symptoms may persist and cause recurrent varicose veins in the long term [6-10]. Therefore, it is necessary to determine the pathological segment with venous insufficiency and choose the most convenient treatment option accordingly.
Applying a standardized mapping method in lower extremity venous system assessment with Doppler US can reveal a relationship between the types of GSV insufficiency and the treatment method for these specific types. There are some classification methods for GSV reflux in the literature. Some researchers divided reflux patterns into six groups by mapping the lower extremities of a female population. They described the GSV reflux patterns in separate groups as segmental and multi-segmental. The study described different types that can be combined practically, making these methods clinically less applicable [11]. So far, the classification systems created in some other investigations [4, 12] were also not widely accepted due to their detailed and complex typology that makes them difficult to use in routine. A practical and widely accepted clinical classification of venous insufficiency has not yet been established. As mentioned in some other studies [10], it is clear that there is a need for a widely accepted, clearly understandable, effective, and practical anatomical classification of reflux patterns.
This study aimed to assess the validity and effects on the clinical severity of a recently defined and easily applicable reflux classification system [10[ in patients with GSV insufficiency. Furthermore, we investigated the effect of reflux patterns on the preference of the treatment modality.
The data of 452 patients were assessed who applied to the Başkent University Alanya Hospital, cardiovascular surgery outpatient clinic, to complain of chronic venous disease between January 2018 and February 2021. This retrospective study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The ethics committee of Başkent University Faculty of Medicine approved the study, and informed consent was taken from all the patients. Age, gender, weight, height, body mass index (BMI), presence and duration of symptoms were recorded for each. We scored the clinical situation with clinical, etiological, anatomical, and pathophysiological elements (CEAP) classification. CEAP scoring was made by the revised version in 2020, as shown in Table 1 [13]. CEAP scores were defined as mild (C1-C2) CVI and severe (C3-C6) CVI. Moreover, the venous clinical severity score was assessed and recorded for each patient according to the revised method [14, 15], as shown in Table 2 (rVCSS). A total of 771 lower extremity examinations were performed with Doppler US. Then, insufficiency maps of the lower extremity venous systems were recorded. An experienced radiologist made all Doppler US examinations. All patients were examined with 9 MHz or 12 MHz linear multi-frequency transducers (S2000, Siemens) in the standing position. Conventionally, the reflux is called venous flow in the opposite direction, longer than 0.5 seconds after provocation (squeezing and releasing with or without the Valsalva) maneuvers (16). As previously described in the recent literature (10) to Doppler US findings, we classified GSV reflux patterns into four types, as illustrated in Figure 1. Type 1, primary GSV reflux with or without the involvement of some superficial branches; type 2, reflux involving the malleolar area with competent SFJ (saphenofemoral junction); type 3, reflux involving SFJ with the competent malleolar area; type 4, reflux involving both malleolar region and SFJ. We did not make the classification by considering below or above the knee. Then we investigated the association between the type of reflux and patients' age, presence of symptoms, duration of varices, BMI (weight and height), VCSS score, and CEAP classification.
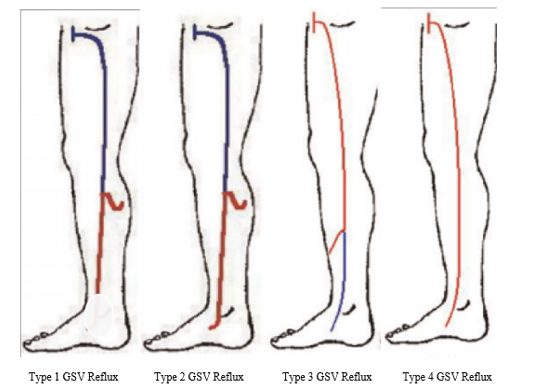
Figure 1: Diagram of Reflux Patterns
Illustrations from Engelhorn CA, Cassou MF, Engelhorn AL, Salles-Cunha SX. Does the number of pregnancies affect patterns of great saphenous vein reflux in women with varicose veins?. Phlebology. 2010;25(4):190-195. doi:10.1258/phleb.2009.009057).
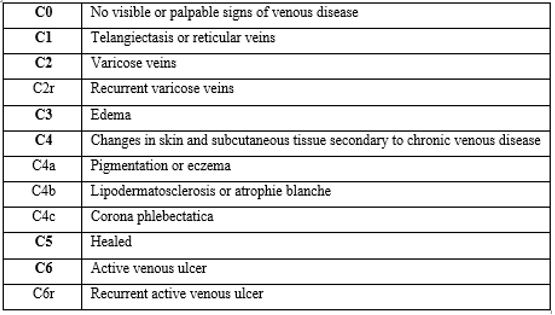
Table 1: CEAP (Clinical Manifestations, Etiology, Anatomic Distribution, Pathophysiology) Classification System and Reporting Standard, Revision 2020

Table 3: Clinical & demographical findings of patients based on the reflux patterns
Numerical data are presented as the mean±SD
* BMI: Body mass index
** VCSS: Venous clinical severity score
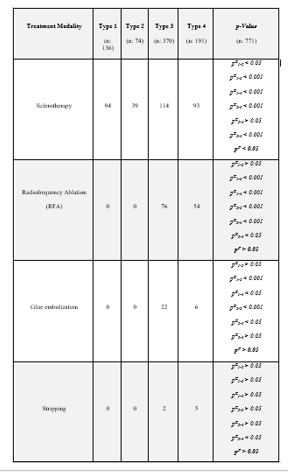
Table 4: Association of reflux patterns with treatment modalities
Patients with a history of superficial or deep venous thrombosis, reflux of femoral vein both above and below the knee, a history of lower extremity trauma, congenital vasculopathy, thrombophilia, severe systemic disease, pregnancy, breastfeeding, and the patients who underwent lower extremity surgical or percutaneous treatment in the last six months, were not included in the study. Primary varicosities with C2-C6 patients, SFJ incompetence, and GSV reflux lasting longer than 0.5 seconds on duplex scanning were evaluated for thermal and non-thermal therapeutic ablation methods.
ClosureFast RFA System (Medtronic, İstanbul, Turkey) was used for the thermal ablation of GSV. The 7 cm long therapeutic distal tip operates for 20 seconds per cycle. The generator automatically controls the power adjustment to maintain the temperature of the heating element at 120 0C. Radiofrequency energy transmission is automatically terminated 20 seconds after the procedure. If necessary, a second cycle can be started immediately after the first, and two or three cycles can be applied in large vessels. Tumescent anesthesia infiltration around GSV was applied to all patients who underwent thermal ablation. CGE of GSV was carried out with The VariClose Vein Sealing System (Biolas, Ankara, Turkey). The continuous drawback technique was applied to give 0.03 cc of polymer in every centimeter via an injection gun. Ablation therapy was started to be applied from the lowest region of reflux. In patients whose GSV diameter >15 mm, RF ablation was preferred over CG embolization (17). An experienced operator applied the treatment of all patients.
Statistical Analysis
SPSS software version 20.0 was used to make the statistical analysis. Mean and SD calculated for continuous variables, then frequencies and percentages were reported as descriptive statistics of categorical variables. We run the Chi-squared test to compare categorical variables, including age, CEAP, and the presence of symptoms associated with the reflux pattern, Fisher's exact test for multivariable analysis as well. Then, a two-sided Student t-test was performed to assess and compare the continuous variables. We used the one-way analysis of variance to define the significant difference between the means. A p-value less than 0.05 considered indicating the statistically significant difference. Then, a t-test was used for comparison. For an individual test, a p-value less than 0.009 considered significant.
In our study, 304 patients were females, and the male-to-female ratio was 0.49 (148:304). A total of 519 (67.3%) lower extremities belong to the females, and 252 limbs (32.7%) to the male patients. The mean age of the research group was 44.7±11.2 years. The mean weight was found 72.8±13.9 kg, and the mean BMI was 26.9±5.0 kg/m² in the study group.
Clinical examination revealed one or more symptoms of CVI in 719 lower extremities (93.3%). There were no symptoms in 52 lower limbs (6.7%). Overall, the average duration of chronic venous disease was 11.8±9.8 years. The CEAP classification in these lower extremities: 391 lower extremities were classified as mild from C1 to C2 (84.6%) and severe from C3 to C5 (15.2%) in 70 lower limbs. Only one lower extremity was described as C6 (0.22%). The mean VCSS in the whole study group was 3.7±2.9. The most common reflux pattern was type 3 (48%) during the initial diagnosis, followed by the type 4 pattern (24.8%).
We have presented clinical and demographical findings of the patients based on the reflux pattern in Table 3. Patients in the type 1 reflux group were the youngest (p<0>). The patients' age tended to increase with the superficial venous insufficiency involving perimalleolar region or SFJ compared to type 1; however, the age differences were not significant statistically according to the corrected p-values (compared to type 1 p=0.04, and p=0.03 for type 2 and 3, respectively). BMI showed a significant difference (p=0.008) between the groups, and the mean values increased with the advance of the reflux type. Patients with type 1 reflux had the lowest BMI (24.8±4.1 kg/m²). The comparative analysis based on BMI concluded that a statistically significant difference was existing among type 2 (27.1±4.4), type 3 (27.4±4.5), type 4 (27.6±4.4) patients, and type 1.
The group with the lowest VCSS was the patients with type 1 reflux pattern. While a significant increment in VCSS was detected in the type 3 pattern by the effect of SFJ involvement (p=0.006), it was determined that the mean VCSS was the highest in type 4 reflux (p=0.001). Compared with type 1 reflux, no statistically significant difference was observed in type 2 reflux (p=0.9). Similarly, patients with type 2 reflux had significantly lower VCSS when compared to patients with type 4 reflux pattern (p=0.005), while the mean VCSS was not significantly different from type 3 insufficiency (p=0.3). There was a significant correlation between the CEAP score and the reflux pattern of the patients included in the study (p=0.002). Usually, patients with type 1 and type 2 reflux patterns had mild CVI (95.1% and 96.8%, respectively). Only 4.9% and 3.2% of them were classified as severe CVI, respectively. Differently, 15.4% of type 3 reflux patients and 20.4% of type 4 patients were scored as C3-C6, meaning they had severe CVI. In type 1 reflux patients, the clinical situation was significantly milder than type 4 but not statistically different from type 2 or type 3 (p=0.004, p=0.040, p=0.501, respectively). Furthermore, the clinical condition of type 2 patients was significantly milder than type 4 patients (p=0.002).
Moreover, symptoms such as pain, burning, swelling, night cramps, itching, and numbness in the legs were present in 87% of patients with type 1 GSV insufficiency. Symptoms existed in 97% of those with type 2 insufficiency, 92% of those with type 3, and 95% of patients with type 4 failure. The symptomatic presentation was less likely in type 1 insufficiency when compared to type 2 and type 4 (p=0.03 and p=0.04, respectively). We observed the symptomatic admissions more frequently in type 2 insufficiency involving the perimalleolar region when compared to type 3 (p=0.05). However, after a statistical correction test was run, none of these differences were considered significant (p>0.06). There was no significant difference between the patient groups with type 3 and type 4 reflux patterns based on demographic and clinical parameters. However, there was a significant difference between gender and reflux patterns (p=0.004). On the other hand, we did not observe a statistically considerable relation between reflux types and gender distribution after further statistical analysis and correction tests. As a conclusion of this study, no relationship was found between the duration of varices and reflux patterns (p=0.950).
As presented in Table 4, sclerotherapy was the most common treatment modality in type 1 insufficiency. Also, in type 2 and type 4 reflux patients, sclerotherapy was more preferred than type 3. Neither RFA nor CGE of the saphenous vein was an option for type 1 and 2 patterns. RFA was mostly preferred in type 4 reflux, while CGE was more frequently preferred for type 3 patients. The number of surgical GSV high ligation and stripping was insufficient as numbers for statistical comparison.
GSV insufficiency constitutes the majority (83%) of superficial venous insufficiency in the lower extremities [4, 5, 10, 16]. That kind of venous failure involves the venous system segmentally [10-16]. It is crucial and decisive to map the segmental involvement with a standardized, understandable, and easily identifiable method in routine radiological practice. According to the recent literature data, the detailed effects of segmental involvement on clinical status have not been determined yet. In this study, we examined patients with GSV insufficiency by dividing them into the groups according to the involved segment, like Yılmaz et al. did [10]. According to our Doppler examination findings, the most common reflux pattern was type 3, in which SFJ is involved and the perimalleolar region spared. The statistical analysis displayed that the reflux pattern correlated with VSCC, CEAP score, and BMI. However, the reflux pattern showed no significant relationship with the mean age and duration of varicosis.
The patients with type 1 insufficiency were the youngest, the clinical status was the mildest, and the mean BMI was also the lowest in the study group. Therefore, we may describe type 1 reflux as the initial or early stage of GSV insufficiency. In other groups where the malleolar region and SFJ were involved (type 2, 3, and 4 reflux patterns), a significant increment existed in variables such as mean age, BMI, VCSS, and CEAP score when compared to type 1 patients. When the reflux type advanced, the severity of the clinical findings and the average BMI progressed. In brief, the clinical course was more severe in superficial venous insufficiency patients with the malleolar region (types 2 and 4) and particularly SFJ (types 3 and 4) pathology. Thus, to evaluate the effect of SFJ involvement on the clinical situation, type 1 and 2 groups were compared one on one, and type 1 and 3 groups. Accordingly, it was determined that in type 3, VCSS was significantly higher than type 2. Based on the VCSS parameter, no statistically significant difference was existing between types 1 and 2. The conclusion elucidates that SFJ failure is a crucial finding that indicates advanced GSV insufficiency. Since the clinical condition of patients with type 2 reflux pattern was significantly milder than type 3.
Varicosis is a venous circulation disease that can cause pain, heaviness, and night cramps in the legs. However, these symptoms are nonspecific and can frequently appear in individuals without venous insufficiency [16, 19]. The advance of the disease can not be predicted at the initial diagnosis. The presence, severity, and progression of the symptoms may be related to the degree of venous valve regurgitation. As the conclusion of some studies, a correlation was found between reflux and symptoms in the limbs [18, 19]. Some researchers defined that the clinical severity of the disease was more severe in advanced age than the younger individuals and defined the presence of reflux associated with increased CEAP score. However, reflux was not classified based on the segmental involvement, and since they did not compare reflux types with symptomatology, they could not reveal the cause of this correlation [18, 19]. In this study, we determined that patients of GSV insufficiency with the malleolar region and SFJ involvement were older and had higher CEAP scores than patients with type 1 reflux. Therefore, we consider that reflux with SFJ involvement may be an advanced form of chronic venous insufficiency, emerges at an advanced stage. So that, patients with type 3 and 4 had more severe symptoms, higher CEAP scores, and a more severe clinical course. This conclusion may suggest that patients of advanced age with severe venous insufficiency may have the regarding GSV pathology longer than expected. Furthermore, if all patients get appropriate treatment in the early stages, we can prevent the progression of the disease and then the emergence of severe clinical pictures. The origin of venous insufficiency has long been a controversial issue. To elucidate that the relationship between the severity of reflux and the prevalence should be disclosed firstly. Conventionally, it is considered reflux originates at the SFJ level and progresses in a retrograde course. However, some studies have stated that reflux may occur in a different segment and then advances in the retrograde or antegrade way [16-20]. This study revealed that venous insufficiency could occur without SFJ involvement in some cases (136 of 771 limbs, 17.6%). Moreover, our study displayed that the clinical course was milder in patients without SFJ involvement, so these conclusions support the antegrade reflux theory. Several studies investigated the relationship between the clinical severity of varices and reflux patterns. These studies focused on a crucial point of reflux (such as involvement of SFJ) rather than comparing reflux patterns with each other [20, 21]. According to some recent research, while SFJ reflux was associated with the most severe form of the disease, reflux in the proximal GSV segments without the involvement of SFJ was found to be associated with mild to moderate CVI. At the same time, they showed that obesity remarkably increased the incidence of severe CVI. Being female also advanced the frequency of severe diseases [19, 20, 21]. We classified C1-C2 as mild CVI and C3-C6 as severe in our study, based on our clinical experience and symptomatology. It has been mentioned in the literature that family history and BMI increased the incidence of venous insufficiency [20, 21]. Consistent with these literature data, we found a positive correlation between SFJ and malleolar region involvement and BMI. The outcomes reveal the effect of intra-abdominal pressure on venous insufficiency and a contributing risk factor for the severity of the disease. In the literature, several recent studies support the outcomes of our research.
Some researchers classified reflux into five types and ten subtypes according to the presence of varicose veins and saphenous vein insufficiency. The most common reflux type was venous insufficiency with SFJ involvement, similar to the pattern we classified as type 3 in terms of main characteristics. Another similarity with the conclusion of our study was that age and CEAP score correlated with the progression of reflux [12]. Some methods suggested for reflux classification have not been applied widely in routine Doppler US practice due to their complexity. Some systems, including reflux components without varicose veins and reflux in a branch of SFJ or several methods that categorize reflux as segmental and multi-segmental, were found incomprehensible [4, 11, 13]. Thus, these are not used commonly in routine Doppler US examinations. Besides, in some studies on this subject, the most common type of venous reflux was determined as the type with SFJ involvement. At the same time, some researchers found that the most common pattern was segmental reflux type without SFJ involvement [11, 20, 21].
Classification of GSV reflux patterns is essential for identifying different types of venous insufficiency and their therapeutic effects. Various treatment modalities, including surgical, thermal, and non-thermal endovenous treatments, are applicable for venous insufficiency. Surgery has been a longstanding treatment option for venous insufficiency that involves the stripping of GSV just below the popliteal level, including high ligation SFJ. Endovenous thermal ablation methods are the modern treatment modalities that have recently been presented as the first-line treatment of venous insufficiency. However, the endovenous treatment of GSV below a certain level distal to the knee is frequently not applicable due to possible damage to the saphenous nerve. Because the nerve and GSV are in close contact under the knee [9, 10, 21]. The segment below this level can be treated with foam sclerotherapy after thermal ablation of the proximal part. Endovenous non-thermal treatments do not cause nerve damage and can be offered as a safer option for GSV insufficiency above or below the knee [21]. Showing the segmental distribution of GSV with mapping increases the prospect of choosing the correct surgical and endovascular treatment option in patients. So, unnecessary or inadequate treatments and possible recurrence or complications can be avoided. The outcomes of endovascular or surgical treatment at an early stage when the perimalleolar region or SFJ is not involved (type 1) are not known on the long-term development of the disease process yet. Therefore, further studies investigating the issue and follow-up patients for a long time are needed.
Sclerotherapy has been used successfully as a treatment method for intradermal, subcutaneous, and perforator veins. The success of sclerotherapy leans on the diagnostic and procedural methodology that includes medical history, clinical and duplex ultrasound examinations. Duplex ultrasound shows the pattern, severity, localization of venous insufficiency and measures the vein diameters. Sclerotherapy is a widely used and effective modality to reduce the appearance of cosmetically disturbing telangiectasias in patients having milder clinical status. Therefore, the prominence of sclerotherapy as the most preferred treatment method in type 1 reflux patients in our study can be attributed to cosmetic reasons. Liquid sclerotherapy was chosen as a method for treating telangiectasis, spider veins, and reticular varices. We know from the previous studies that occlusion rate depends on the vein diameter [22] so, foam sclerotherapy was the method of treatment in varicose saphenous tributaries and large incompetent perforator veins, which is consistent with the literature [23]. Simultaneous application with thermal and non-thermal treatment techniques and its success as an alternative to phlebectomy may explain why it was preferred more often than type 3 in patients with type 2 and 4 patterns who suffer from incompetent tributary veins below the knee. Since ultrasound-guided foam sclerotherapy for ablation of GSV appears to be less successful (approximately 25%) than endothermal techniques, that was never preferred as a treatment method for the insufficiency [17]. RFA has a favorable side-effect profile in conjunction with a high rate of maintained GSV occlusion in the midterm [24] and late results [25] and has been verified by prospective studies with endovenous laser ablation (EVLA) and surgery [26]. Since the vein wall, not the lumen is the target, vein diameter has no longer be an issue for RFA because of the vasoconstrictive properties of tumescent anesthesia. These features could explain why 28.2% of the type 4 pattern patients underwent RFA after initial diagnosis. In 7 patients, due to the high tortuosity of GSV, traditional surgical techniques were performed. As expected, both thermal and non-thermal procedures and surgical methods were not used in type 1 and type 2 pattern patients due to the absence of reflux in the proximal GSV segment.
In this retrospective study, we made the statistical analysis considering the gender factor also. However, that was not included in a separate statistical significance evaluation due to the insufficient pregnancy and number of children data in the medical history of many female patients. If there were sufficient data in the patients' medical history, evaluating the relationship between smoking and chronic diseases and venous insufficiency would be a factor that would increase the value of this study. Furthermore, the higher number and variety of cases, particularly the higher number of subjects with specific segmental involvement, would increase the reliability of the statistical conclusions. In our study, grading of the segmental distribution was not confirmed by long-term clinical outcomes. More studies are needed to demonstrate the clinical value of the finding. In this study, we analyzed only the presence of symptoms, not the types of symptoms based on segmental distribution. The mentioned issues are among the limitations of our research, which we acknowledged.
In this research, we investigated the availability of the method that is practical and clinically applicable to categorize GSV insufficiency. Mapping venous insufficiency with Doppler US is essential to determine the most effective treatment modality. Besides, we assigned that GSV insufficiency with SFJ involvement (defined as type 3 and 4) had a more severe clinical presentation, and the reflux classification system correlated with the severity of the disease.
Conflict of interest disclosure
The authors declared no conflicts of interest.
Highlights
- Mapping venous insufficiency with Doppler US is essential to determine the appropriate treatment plan.
- SFJ involvement displays severe superficial venous disease and advanced venous insufficiency.
- There was an association between reflux type and clinical severity. As reflux type advances, VCSS and CEAP scores increase.
Footnote
Reporting Checklist: The authors have completed the MDAR reporting checklist.
On a separate form, the clinician will be asked to:
“For each leg, please check one box for each item (symptom and sign) that is listed below.”
Pain or other discomfort (i.e., aching, heaviness, fatigue, soreness, burning)
The clinician describes the four categories of leg pain or discomfort outlined below to the patient and asks the patient to choose, separately for each leg, the category that best describes the pain or discomfort the patient experiences.
None = 0: None
Mild = 1: Occasional pain or discomfort that does not restrict regular daily activities
Moderate = 2: Daily pain or discomfort that interferes with, but does not prevent, regular daily activities
Severe = 3: Daily pain or discomfort that limits most regular daily activities
Varicose Veins
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the patient's superficial veins. The standing position is used for varicose vein assessment. Veins must be ≥3 mm in diameter to qualify as "varicose veins."
None = 0: None
Mild = 1: Few, scattered varicosities that are confined to branch veins or clusters. Includes "corona
phlebectatica" (ankle flare), defined as >5 blue telangiectasias at the inner or sometimes the outer edge of the foot
Moderate = 2: Multiple varicosities that are confined to the calf or the thigh
Severe = 3: Multiple varicosities that involve both the calf and the thigh
Venous Edema
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the patient's pattern of leg edema. The clinician's examination may be supplemented by asking the patient about the extent of leg edema that is experienced.
None = 0: None
Mild = 1: Edema that is limited to the foot and ankle
Moderate = 2: Edema that extends above the ankle but below the knee
Severe = 3: Edema that extends to the knee or above
Skin Pigmentation
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the patient's skin pigmentation. Pigmentation refers to color changes of venous origin and not secondary to other chronic diseases.
None = 0: None, or focal pigmentation that is confined to the skin over varicose veins
Mild = 1: Pigmentation that is limited to the perimalleolar area
Moderate = 2: Diffuse pigmentation that involves the lower third of the calf
Severe = 3: Diffuse pigmentation that involves more than the lower third of the calf
Inflammation
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the patient's skin inflammation. Inflammation refers to erythema, cellulitis, venous eczema, or dermatitis rather than just recent pigmentation.
None = 0: None
Mild = 1: Inflammation that is limited to the perimalleolar area
Moderate = 2: Inflammation that involves the lower third of the calf
Severe = 3: Inflammation that involves more than the lower third of the calf
Induration
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the patient's skin induration. Induration refers to skin and subcutaneous changes such as chronic edema with fibrosis, hypodermitis, white atrophy, and lipodermatosclerosis.
None = 0: None
Mild = 1: Induration that is limited to the perimalleolar area
Moderate = 2: Induration that involves the lower third of the calf
Severe = 3: Induration that involves more than the lower third of the calf
Active Ulcer Number
The clinician examines the patient's legs and, separately for each leg, chooses the category that best describes the number of active ulcers.
None = 0: None
Mild = 1: 1 ulcer
Moderate = 2: 2 ulcers
Severe = 3: ≥3 ulcers
Active Ulcer Duration
If there is at least 1 active ulcer, the clinician describes the four categories of ulcer duration outlined below to the patient and asks the patient to choose, separately for each leg, the category that best describes the duration of the most prolonged unhealed ulcer.
None = 0: No active ulcers
Mild = 1: Ulceration present for <3>
Moderate = 2: Ulceration present for 3-12 mo
Severe = 3: Ulceration present for >12 mo
Active Ulcer Size
If there is at least 1 active ulcer, the clinician examines the patient's legs, and separately for each leg, chooses the category that best describes the size of the largest active ulcer.
None = 0: No active ulcer
Mild = 1: Ulcer <2>
Moderate = 2: Ulcer 2-6 cm in diameter
Severe = 3: Ulcer >6 cm in diameter
Use of Compression Therapy
Choose the level of compliance with medical compression therapy
None = 0: Not used
Mild = 1: Intermittent use
Moderate = 2: Wears stockings most days
Severe = 3: Full compliance: stockings
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
