
Research Article | DOI: https://doi.org/10.31579/2690-1919/492
1Department of Anesthesiology and Reanimation, Konya City Hospital, University of Health Science, Konya, Turkey.
2OUTCOMES RESEARCH Consortium®, Houston, Texas, USA. - Member of Consortium.
3Department of Anesthesiology and Reanimation, Yeditepe University Kosuyolu Hospital, Istanbul, Turkey.
4Necmettin Erbakan University, Meram Faculty of Medicine, Department of Anesthesiology and Reanimation, Konya, Turkey.
*Corresponding Author: Yasin Tire, Department of Anesthesiology and Reanimation, Konya City Hospital, University of Health Science, Konya, Turkey.
Citation: Bülent Hanedan, Mine Hanedan, Yasin Tire, Barış Çankaya, Sema T. Uzun, (2025), Evaluation of the Effectiveness of Non-Steroidal Anti-Inflammatory Drugs (Nsaids) According to Their Cyclooxygenase Selectivity in Neuropathic Pain Model in Rats (Experimental Study), J Clinical Research and Reports, 19(5); DOI:10.31579/2690-1919/492
Copyright: © 2025, Yasin Tire. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 March 2025 | Accepted: 18 April 2025 | Published: 05 May 2025
Keywords: lornoxicam; meloxicam; dexketoprofen; neuropathic pain models in rats; neuropathic pain
Aim: Recent studies on neuropathic pain treatment and mechanisms reveal that NSAIDs, which are mostly used in types of pain related to inflammation, may also be effective in neuropathic pain. In this experimental study, we created a neuropathic pain model in rats with sciatic nerve ligation. We investigated the effectiveness of lornoxicam (nonselective COX enzyme inhibitor), meloxicam (selective COX-2 enzyme inhibitor), and dexketoprofen (nonselective COX enzyme inhibitor) on mechanical hyperalgesia, which is a clinical finding of neuropathic pain and can be measured objectively and numerically with electronic von Frey (evF) according to their cyclooxygenase enzyme (COX) selectivity. Thus, we aimed to contribute to the literature and clinical practice by demonstrating the effectiveness of COX selectivity in the treatment of neuropathic pain.
Materials and Methods: 35 male Wistar-albino rats with normal motor activity were included in the study. The animals were randomly divided into 5 groups as control (Group I n=7), lornoxicam (Group II n=7), meloxicam (Group III n=7), dexketoprofen (Group IV), and sham surgery (Group V). The Chronic Constriction Injury (CCI) - induced neuropathy model described by Bennett and Xie was applied. As described in this model, after the sciatic nerve of the right hind legs of the rats was surgically exposed, three loose knots were tied with 4/0 catgut at 1 mm intervals from 4 different places. In the group that underwent sham surgery, the sciatic nerve was re-closed without any procedure after being exposed. In this way, lornoxicam 1.3 mg/kg, meloxicam 5.8 mg/kg, and dexketoprofen 15 mg/kg were administered intraperitoneally to the groups that developed neuropathic pain. Drug applications were performed in a single-blind manner. Mechanical hyperalgesia measurements were made with an EVF device and recorded. The study was completed without any problems with 35 subjects.
Results: In rats with neuropathic pain, a significant difference was found between the control group that received physiological serum and the groups that received COX inhibitors at all measurement times (p<0.008). When the drug-administered groups were compared in pairs; Intraperitoneal dexketoprofen administration was found to be statistically more significant than intraperitoneal lornoxicam or meloxicam administration at 30th minute (p<0.008). Intraperitoneal lornoxicam administration was found to be statistically more significant than intraperitoneal meloxicam or dexketoprofen administration at 150th and 180th minute (p<0.008).
Conclusion: COX inhibitors are effective in preventing mechanical hyperalgesia in neuropathic pain.
Neuropathic pain is defined as “pain resulting from a disease or lesion affecting the somatosensory system” (Treede RD, 2008). It is a chronic condition when not treated promptly and correctly. A better understanding of the mechanisms of neuropathic pain, which is completely different from other types of pain, has made it easier for us to approach this group of diseases that are difficult to diagnose and treat. Antidepressants, anticonvulsants, opioids, local anesthetics and capsaicin, local preparations and interventional methods are used in the treatment of neuropathic pain. Simple analgesics, such as paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs), are generally ineffective in the treatment of neuropathic pain (Namaka M. 2004, Namaka M. 2009). However, in experimental studies conducted in recent years, the effectiveness of simple analgesics in neuropathic pain models has been evaluated, and it has been argued that paracetamol and NSAIDs will increase the effectiveness of these drugs, especially when added to other drugs used in the treatment of neuropathic pain (McCormack KJ. 1994, Eroğlu L 2002). The antihyperalgesic effect of paracetamol increases dose-dependently and shows a synergistic effect when used together with other drugs used in the treatment of neuropathic pain (Raffa R. 2010, Dani M. 2007, Bonnefont J. 2003). Experimental studies have shown that NSAIDs reduce mechanical hyperalgesia and their effectiveness varies according to their COX selectivity (Kimura S. 2009). Meloxicam, a selective COX-2 inhibitor, was found to be more effective than ibuprofen, a selective COX-1 inhibitor, in rats with diabetic neuropathy. Lornoxicam, a nonselective COX inhibitor, was reported to be more effective than proxicam in the same group and to reduce mechanical hyperalgesia (Bianchi M. 2002). We did not come across a study in the literature evaluating the effectiveness of dexketoprofen, which has been widely used in our country in recent years, on mechanical hyperalgesia. In this study, lornoxicam, meloxicam and dexketoprofen were used in rats in an experimental neuropathic pain model. We aimed to . evaluate the effects of profen on mechanical hyperalgesia.
This study was conducted in SUDAM laboratories and Selcuk University Selcuklu Medical Faculty Pharmacology Department laboratory after receiving approval from Selcuk University Meram Medical Faculty Experimental Animal Research Center (SUDAM) ethics committee with the number 2011-050.
Subjects:
35 Wistar-albino male rats were included in the study. The rats weighed between 315-520 gr and had normal motor activity. The floor of the cages where the experimental animals were housed was kept soft with sawdust in order to minimize possible painful mechanical stimulation. Rats were placed in cages in numbers of maximum 4. The rooms where the cages were located were standardized to prevent external light from passing through and to have a 12-hour light and 12-hour dark cycle, an ambient temperature of 22 ±2oC and a humidity of 70-75%. They were fed with standard rat food and tap water.
Preparatıon of the subjects:
Before the surgical procedure, the responses of all animals to mechanical stimulation were measured with evF to establish baseline values and recorded. All rats, whose feeding was stopped 12 hours before the operation and who were allowed to drink only water, were anesthetized with a mixture of 50 mg/kg intraperitoneal ketamine 10% (Ketalar®) and 10mg/kg intraperitoneal xylazine 2% (Rompun®) (Figure 3.1).

Figure 3.1: Administration of anesthesia with an intraperitoneal ketamine-xylazine mixture.
After anesthesia induction, the CCI-related neuropathy model described by Bennett and Xie was applied. For this purpose, the hair covering the right thigh region of the rats was shaved and cleaned, and the opened area was wiped with povidone iodine. The skin was cut with a scalpel so that it would extend parallel to the thigh. The sciatic nerve was reached with blunt dissection along the M. Biceps femoris. Three loose knots were tied with 4/0 catgut at 1 mm intervals from 4 different places on the exposed sciatic nerve (Figure 3.2).
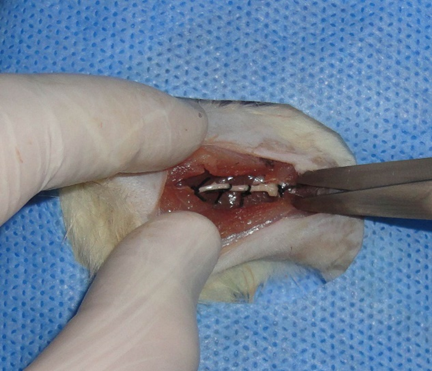
Figure 3.2: Ligation of the sciatic nerve.
The incision was closed in layers with 3/0 silk (Figure 3.3).

Figure 3.3: Closure of the skin.
The rats were waited for 21 days for neuropathic pain to develop. In the sham (pseudo-surgery) group, similar surgery was applied without affecting the sciatic nerve, and the skin was closed after the sciatic nerve was exposed.
Experımental groups:
Animals that developed neuropathic pain were randomly divided into control, lornoxicam, meloxicam, and dexketoprofen groups (Table 3.1). Drug administrations were performed in a single-blind manner.
| Groups | Explanation | Number of subjects | Applied content |
| 1 | Control group | 7 | 2 ml saline |
| 2 | Lornoxicam group | 7 | 1.3 mg/kg lornoxicam |
| 3 | Meloxicam group | 7 | 5.8 mg/kg Meloxicam |
| 4 | Dexketoprofen group | 7 | 15 mg/kg deksketoprofen |
| 5 | Sham group | 7 | none |
Table 3.1: Working groups and drugs administered
Preparatıon And Admınıstratıon Of Drugs
Xefo vial (Lornoxicam, Abdi İbrahim, 4 mg/ml), Meloks ampoule (Meloxicam, Nobel İlaç Sanayi, 10 mg/ml) and Arveles ampoule (Dexketoprofen, İbrahim Etem Ulagay, 25 mg/ml) were used as drugs. The drugs were drawn into 5 ml syringes in doses appropriate to the weights of the rats. They were completed to 10 ml volume with physiological serum. The prepared drugs were injected intraperitoneally with a 22 G needle into the right lower quadrants of the rats that were held with the appropriate method.
Measurement Wıth Evf
After the surgical intervention and waiting 21 days for the development of neuropathic pain, the weights of the rats were measured again before the drug injection. In the extremity where the CZ-induced neuropathy model was applied, mechanical hyperalgesia was measured with the evF device at minute 0 (before drug or physiological serum application) and at minutes 30, 60, 90, 120, 150 and 180 after the application of the drugs. After the device was calibrated, each rat was placed in open-topped, transparent-sided cages with holes suitable for mechanical stimulation to the plantar surface of the foot. Measurements were started on rats that got used to the environment and exhibited natural behaviors. All measurements were performed by the same researcher in order to avoid hand changes. The evF fiber was contacted at a right angle to the mid-plantar surface of the right hind extremity of the rats with the help of the mirror under the measurement cages (Figure 3.4).
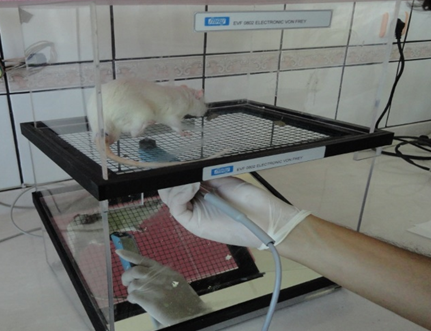
Figure 3.4: Measurement with electronic von Frey
The applied pressure force was gradually increased. The increase in the applied force was observed graphically and numerically on the computer screen (Figure 3.5).
Figure 3.5: The increase in applied force Graphical and numerical detection
The numerical value when the rat withdrew its paw was recorded by viewing it on the computer screen. The measurements were repeated and the values were confirmed. The withdrawal made by the animal during spontaneous movement, independent of pain, was evaluated as false positive and was not considered significant. The cut-off value was determined as 200 g since it would damage the rat's paw and could also falsely affect the reliability of the measurement. After the measurements, the rats were sacrificed under anesthesia by the cervical dislocation method.
After calculating the % maximal possible effects (MPE) of the withdrawal threshold values measured at the end of the study, the new values obtained were used for statistical analysis. The following formula and the 200 g cut-off value were used for this calculation. Statistical analysis was performed using the SPSS v16.0 (SPSS Inc., Chicago, IL, USA) package program. Continuous variables were shown as mean±standard deviation. Categorical variables were expressed as frequency percent It was given as a series. The difference between all groups was made with Kruskal-Wallis one-way variance analysis. A value smaller than P<0>
There was no significant difference between the weights measured before and after surgery of Wistar Albino male rats included in the study (p<0>WEIGHT (gr) Group I Group II Group III Group IV Group V P Weight before surgery 371,85±42,95 354,85±35,41 370,85±43,75 378,28±78,49 372,28±40,48 1,00 Weight after surgery 372,28±42,80 354,42±37,72 372,00±45,10 378,85±77,88 372,57±42,01 1,00
Table 4.1: Rat weights.
Effectiveness of the CCI model:
The measurement values in the control group (Group I) were numerically lower than those in the sham group (Group V). When the measurement values of Group I and Group V were compared statistically to evaluate the effectiveness of the CCI model, a significant difference was found (p<0> Group I (n=7) Group V (n=7)Time (min.) P 30. min. 1,09±085 4,62±1,65 0,002* 60. min. 1,12±1,06 4,59±2,20 0,003* 90. min. 0,80±044 4,67±2,07 0,002* 120. min. 0,78±036 5,01±2,16 0,002* 150. min. 1,34±0,81 5,79±1,46 0,002* 180. min. 1,061±0,55 6,21±2,08 0,002*
*p<0>
Table 4.3: Measurement values of all groups (Mean± SD).
Effectiveness of drugs compared in the study:
Measurement values after drug applications are shown in (Table 4.3, Graph 4.1).
Effect of Lornoxicam:
When Group II, which received lornoxicam, was examined; Measurement values were higher at all evaluation times compared to Group I (p<0> Group I (n=7) Group II (n=7)Time (min.) P 30. min. 1,09±0,85 10,22±4,75 0,002* 60. min. 1,12±1,06 24,58±3,34 0,002* 90. min. 0,80±0,44 22,94±7,32 0,002* 120. min. 0,78±0,36 33,36±4,81 0,002* 150. min. 1,34±0,81 50,86±8,68 0,002* 180. min. 1,061±0,55 71,51±1,90 0,002*
* P <0>
Table 4.4: Group I and Group II measurement values (Mean± SD).
When Group II measurement values were compared with Group III, it was observed that they were more effective at 150 and 180 minutes. When compared with Group IV, it was observed that Group IV was more effective at 30 minutes, while Group IV was more effective at 150 and 180 minutes (p<0> Group II (n=7) Group III (n=7)Time (dk) P 30. min. 10,22±4,75 10,74±5,31 0,848 60. min. 24,58±3,34 30,29±8,89 0,180 90. min. 22,94±7,32 27,09±9,51 0,277 120. min. 33,36±4,81 28,31±1,12 0,406 150. min. 50,86±8,68 23,81±1,39 0,003* 180. min. 71,51±1,90 33,05±1,21 0,004*
* P <0>
Table 4.5: Group II and Group III measurement values (Mean± SD).
| Time (min.) | Group II (n=7) | Group IV (n=7) | P |
| 30. min. | 10,22±4,75 | 25,22±5,05 | 0,003* |
| 60. min. | 24,58±3,34 | 16,15±7,73 | 0,025 |
| 90. min. | 22,94±7,32 | 21,91±3,08 | 0,277 |
| 120. min. | 33,36±4,81 | 25,62±8,2 | 0,018 |
| 150. min. | 50,86±8,68 | 22,20±4,00 | 0,002* |
| 180. min. | 71,51±1,90 | 27,84±6,65 | 0,002* |
* P <0>
Table 4.6: Group II and Group IV measured values (Min.± SD).
Effect of Meloxicam:
When Group III, where meloxicam was applied, was examined; the measurement values were higher at all evaluation times compared to Group I (p<0> Group I (n=7) Group III (n=7)Time (min.) P 30. min. 1,09±085 10,74±5,31 0,002* 60. min. 1,12±1,06 30,29±8,89 0,002* 90. min. 0,80±044 27,09±9,51 0,002* 120. min. 0,78±036 28,31±1,12 0,002* 150. min. 1,34±0,81 23,81±1,39 0,002* 180. min. 1,061±0,55 33,05±1,21 0,002*
* P <0>
Table 4.7: Group I and Group III measurement values (Min.± SD).
When compared to Group IV, it was observed that Group IV was more effective at the 30th minute (p<0> Group III (n=7) Group IV (n=7)Time (dk) P 30. min. 10,74±5,31 25,22±5,05 0,004* 60. min. 30,29±8,89 16,15±7,73 0,018 90. min. 27,09±9,51 21,91±3,08 0,142 120. min. 28,31±1,12 25,62±8,2 0,949 150. min. 23,81±1,39 22,20±4,00 0,749 180. min. 33,05±1,21 27,84±6,65 0,565
Table 4.8: Group III and Group IV measured values (Mean± SD).
Effect of Dexketoprofen:
When Group IV, where dexketoprofen was applied, was examined; the measurement values were higher at all evaluation times compared to Group I (p<0> Group I (n=7) Group IV (n=7)Time (dk) P 30. min. 1,09±0,85 25,22±5,05 0,002* 60. min. 1,12±1,06 16,15±7,73 0,003* 90. min. 0,80±0,44 21,91±3,08 0,002* 120. min. 0,78±0,36 25,62±8,2 0,002* 150. min. 1,34±0,81 22,20±4,00 0,002* 180. min. 1,061±0,55 27,84±6,65 0,002*
*P<0>
Table 4.9: Group I and Group IV measured values (Mean± SD).

Figure 4.1: Metric values of all groups.
The significant differences in the regions where it originates and its symptoms, inadequacies in diagnosis, the lack of a complete understanding of the mechanism, and the disregard of factors that increase pain such as depression and anxiety are among the most important reasons why neuropathic pain treatment is difficult (Tuncer A. 2003, Attal N. 2005). Despite the better understanding of its mechanisms and the diversification of drug groups used in its treatment with experimental and clinical studies conducted in recent years, neuropathic pain is still a difficult pain to treat. Today, the main limiting factor in the treatment of neuropathic pain is that frequently used drugs such as anti-depressants and anti-convulsants are off-label (use outside the approved area of use of a drug). Beneficial effects have been shown for agents such as opioids, tramadol, topical medications (lidocaine, capsaicin) used in treatment, and mexiletine, baclofen, ketamine and NSAIDs have been used in some treatments. Despite the use of all these agents, significant pain reduction in patients with neuropathic pain is less than half (Eisenberg E. 2005). Various algorithms and guidelines have been published on the treatment of neuropathic pain.
Namaka M. et al.'s 2009 report on neuropathic pain management outlined four phases based on scanning all articles and researchers' experiences. Antidepressants, antiepileptics, and topical analgesics are advised first. The second phase should utilise narcotic analgesics and refractory medicines, and the third step should use combination therapy. Surgical procedures are indicated as the fourth step if these medications fail to relieve discomfort. Adjuvant analgesic therapy with NSAIDs is possible at all stages (Namaka M. 2009). Despite emerging treatments, no single treatment works for all neuropathic pain. Chronic neuropathic pain is rarely relieved by monotherapy, despite the goal of treating it with one drug. NSAIDs may cure neuropathic pain by modulating several central and peripheral components of pain processes (Namaka M. 2009, Bianchi M. 2002). COX selectivity was used to assess NSAID efficacy in rats with experimental neuropathic pain. Experimental models for animal neuropathic pain use peripheral nerve mechanical damage. Chronic constriction injury (CCI), partial tight ligation (PSL), and spinal nerve ligation (SSL) are the most common partial denervation models, along with the streptozocin-induced diabetic neuropathy model (Ulugöl A. 2012). The CCC model by Bennett and Xie involves tying knots around the sciatic nerve to cause chronic constriction injury and inhibit superficial epineural vascularization (Bennett GJ. 1988). Four ligatures at 1 mm intervals strangle the sciatic nerve by causing intraneuronal oedema. Compression disrupts nerve axons. Destruction of neural structure distal to compression is typical. Due to spontaneous discomfort, rats exhibit several behaviours. These include mild-moderate autotomy (self-attack on the lesioned leg resulting in amputation), protection, excessive licking, limping, and not stepping on it. Autotomy rats are not used in experiments. Detect cold allodynia and hyperalgesia from noxious thermal and mechanical stimulation. Unilateral symptoms. Allodynia, hyperalgesia, and spontaneous pain-related behavioural markers peak two weeks after surgery and persist 2-3 months. We used the CCI neuropathic pain model on rats in this work. Three weeks passed before we measured, including the second week following surgery when neuropathic pain peaked. We compared the sham group, which underwent surgery without harming the sciatic nerve, to the control group to determine if our surgery was effective. Control group (Group I) measurement values were lower than sham group (Group V). Statistics showed a considerable disparity between Group I and Group V measurement values. (p<0>
In their investigation on mice with diabetic neuropathic pain, Kimura S. et al. compared 30 mg/kg ibuprofen to 3, 10, and 30 mg/kg meloxicam. They found that dosages above 3 mg/kg significantly enhanced paw withdrawal threshold. Ibuprofen was minor (Kimura S. 2009). Like our trial, meloxicam was beneficial in neuropathic pain. Meloxicam in combination reduces neuropathic pain, according to research. It reduced neuropathic pain better when administered with aminoguadine hydrochloride than alone, according to Dudhgaonkar SP. et al. (Dudhgaonkar SP 2007). No meloxicam combinations were used in our study.
Similar to our investigation, Takahashi M. et al. found that systemic meloxicam significantly improved tactile allodynia in mice following L5 spinal nerve injury compared to vehicle treatment (Takahashi M. 2005). Lornoxicam demonstrated great tolerability and a higher analgesic efficacy than placebo in a double-blind multicentric parallel group study of 171 individuals with acute sciatic or lumbosciatic pain (Herrmann WA. 2009). Lornoxicam had similar effects to diclofenac in this study. Hu Y. et al. compared lornoxicam to amitriptyline, a common neuropathic pain therapy, on 60 male rats after L5 spinal incision and sham surgery. Amitriptyline treated mechanical allodynia, depression-related behaviours, and cognitive functioning, while lornoxicam only treated mechanical allodynia (Hu Y. 2010). It solely affected mechanical allodynia in our investigation. Lornoxicam, piroxicam, and meloxicam were tested for pain in rats with 10% formaldehyde-damaged tails by Bianchi et al. These medicines greatly reduced hyperalgesia but did not modify thermal pain summation. However, lornoxicam alone prevented hyperalgesia (Bianchi M 2002). As in this study, lornoxicam outperformed meloxicam at 150 and 180 minutes. In rats and mice, Cabra F. and colleagues found dexketoprofen to be strong anti-inflammatory, analgesic, and antipyretic (Cabré F. 1998). No study on dexketoprofen and neuropathic pain was found. However, a study found that dexketoprofen synergistically improves pain therapy when combined with other drugs. Miranda HF. and colleagues examined acute tonic, phasic, and inflammatory pain in mice with dexketoprofen, morphine, and paracetamol. Dexketoprofen synergised with both medicines in all three experiments (Miranda HF. 2007). Like Miranda HF and colleagues, The combination with tramadol was found to be synergistic as antinociceptive and antiexudative (Miranda HF. 2012).
In conclusion, our research indicates that COX inhibitors, such as lornoxicam (1.3 mg/kg), meloxicam (5.8 mg/kg), and dexketoprofen (15 mg/kg), have substantial antihyperalgesic effects in rats suffering from neuropathic pain caused by chronic constriction injury (CCI). Of these, dexketoprofen exhibited the swiftest onset of action, being most efficacious at 30 minutes, although lornoxicam displayed greater efficacy at 150 and 180 minutes in comparison to meloxicam and dexketoprofen. Due to the insufficient evidence on dexketoprofen in neuropathic pain models, additional research is required to investigate its complete potential. This study, focussing on single-dose administration, necessitates further long-term investigations to validate the enduring efficacy of these COX inhibitors in the management of neuropathic pain.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
