
Research Article | DOI: https://doi.org/10.31579/2692-9406/031
*Corresponding Author: Gagik Hakobyan, Head of Department of Oral and Maxillofacial Surgery, Yerevan State Medical University after M. Heratsi, 0028 Kievyan str. 10 ap. 65 Yerevan, Armenia.
Citation: G Hakobyan, I Komissarova, Z Evsyukova, E Ribakova, A Haruthyunyan. (2020) Evaluation of the effectiveness of hyaluronic acid for the treatment of seborrheic dermatitis of the face. Biomedical Research and Clinical Reviews. 1(5); DOI:10.31579/2692-9406/031
Copyright: © 2020 Gagik Hakobyan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 October 2020 | Accepted: 27 November 2020 | Published: 07 December 2020
Keywords: hyaluronic acid; seborrheic dermatitis; erythema; scales
Objectives: The aim of the study was to assess the efficacy of 5% hyaluronic acid crem for the treatment of seborrheic dermatitis of the face.
Materials and methods: A total of 49 patients (28 men and 21 women, age from 31 to 64 years) with seborrheic dermatitis of the face were selected for the study. A single-site, prospective observational study of 5% hyaluronic acid cream for the treatment of facial seborrheic dermatitis was conducted from 2016 to 2020.
All patients underwent a thorough clinical examination according to the generally accepted scheme. Treatment planning includes a thorough history and physical examination, preoperative laboratory examination. At each visit, degrees of scale, erythema, and pruritus were evaluated.
To assess the effectiveness of patients were given a questionnaire to fill out the questions. The questionnaire evaluated the 5% hyaluronic acid crem effectiveness of the treatment.
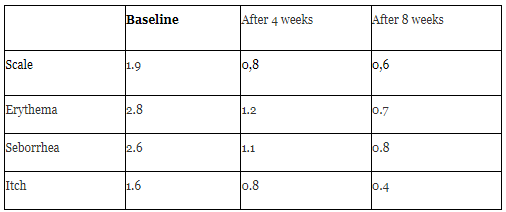
Outcome was the evolution of the Investigator Global Assessment (IGA) scale, assessing erythema, scale / scaling, seborrhea and pruritus, all measured on a five-point scale, from 0: no signs / symptoms to 4: very severe sign / symptom. Subjects were assessed at baseline after 4 and 8 weeks.
Results: Baseline IGA scores (mean ± SD) were 9 ± 3 (range: 5-13). The use of the EDS significantly reduced the IGA score by 67% at 4 week and by 83% at 8 week. The condition improved from baseline in 92.3% of subjects.
Conclusion: 5% hyaluronic acid crem has been effective in reducing erythema, scales, seborrhea, and itching. No local side effects were reported.
Seborrheic dermatitis of the face is a chronic and recurrent inflammatory skin disease that occurs in areas of the face that are rich in sebaceous gland and is a common dermatological disease worldwide, with a high frequency during puberty and a peak in the third and fourth decades of life [1, 2]. Many factors have been identified as predisposing, and understanding of the causes and pathogenesis has improved due to advances in microbiological and analytical methods [3,4]. The pathogenesis of seborrheic dermatitis is not yet fully understood, but Malassezia yeast, hormones, sebum levels and the immune response are known to play an important role [5, 6].
Clinically manifested as erythematous scaly patches or plaques, often associated with itching. Seborrheic dermatitis can affect the head, face, beard, eyebrows, ears or chest. Anywhere we have a proliferation of sebaceous (oil) glands.This inflammatory response additionally disrupts the differentiation of the epidermis and barrier function, and itching and combing can cause further disturbance: as a result, a cycle of immunostimulation, abnormal differentiation of the epidermis and violation of the barrier occur.
The typical symptoms are redness, inflammation, itchiness, flaking skin and thick crusts of buildup. In and in more severe cases sufferers will see yellow scaly pimples. Seborrheic dermatitis can affect the skin of the face, ears, eyebrows, beard, and chest, just like on the scalp.
The goal of treatment should be to provide a safe and effective treatment that improves symptoms, reduces relapses and causes minimal side effects [7]. Because the condition is chronic, treatment should be directed at controlling the frequency and severity of flare-ups. Management of seborrheic often requires medical treatment in the form of local antifungal agents, keratolytics, corticosteroids, and calcineurin inhibitors [8].
The treatment facial seborrheic dermatitis often requires drug treatments in the form of topical antifungals, keratolytics, corticosteroids, and calcineurin inhibitors.
Antimicrobial and anti-inflammatory ingredients used, such as zinc, pyroctonolamine, dihydroventantrimide, gum-2 biosaccharide and stearyl glycyrrhetinate, can accelerate the recovery of seborrheic dermatitis and avoid outbreaks [9, 10].
Corticosteroids are simple and effective, but they should be used with caution because of their side effects, such as thinning skin and stretch marks, which can occur with prolonged continuous use for weeks or months. Creams or lotions containing the calcineurin inhibitors tacrolimus and pimecrolimus may be effective and cause fewer side effects than corticosteroids, although they are more expensive. Such use is "not for its intended purpose", as they are allowed only for the treatment of atopic dermatitirs. Another reason they are not first-choice drugs is because the seborrheic dermatitis is concerned about a possible cancer link.
Patients often experience anxiety about the cosmetic symptoms of seborrheic dermatitis, so reducing clinical symptoms (erythema, scales, and itching) can help improve any psychological stress caused by the condition. Any concerns regarding the psychological impact of the disease should be addressed using the dermatological quality of life index.
Medical devices include items or substances used to aid in the recognition, prevention, monitoring, treatment, and relief of disease and that achieve this "intended primary effect" by physical, rather than direct pharmacological, immunological, or metabolic means, although such effects may support physical effects.
Hyaluronic acid (HA) plays a multifaceted role in regulating various biological processes and maintaining homeostasis in the body [11].
Hyaluronic acid (HA) is an essential component of connective tissue, skin, vitreous humor, umbilical cord and synovial fluid and plays an important role in maintaining the elasticity and viscosity of the extracellular matrix.
Novel, agents for facial seborrheic dermatitis are a welcome addition to the treatment armamentarium of the dermatologist.
The aim of the study was to assess the efficacy of 5% hyaluronic acid crem for the treatment of seborrheic dermatitis of the face.
Materials and methods: 49 patients (28 men and 21 women, age from 31 to 64 years) with seborrheic dermatitis of the face were selected for the study. A single-site, prospective observational study of 5% hyaluronic acid crem for the treatment of facial seborrheic dermatitis was conducted from 2016 to 2020.
All patients underwent a thorough clinical examination according to the generally accepted scheme. Treatment planning includes a thorough history and physical examination and laboratory examination.
Subjects were instructed to cleanse the affected area with the gentle cleanser and pat dry with a soft towel before applying the provided medication. A thin layer of medication was to be gently massaged in to the affected areas twice daily, in the morning and evening.
The 5% hyaluronic acid crem was used for four weeks and the purification procedure continued for another four weeks.
The primary outcome was the evolution of the Investigator Global Assessment (IGA) scale, assessing erythema, seborrhea and pruritus, all measured on a five-point scale, from 0: no signs / symptoms to 4: very severe sign / symptom. Subjects were assessed at baseline after 4 and 8 weeks of treatment by an investigator with no knowledge of the type of treatment. Local tolerance was assessed by checking self-reported side effects at each visit.
Results: Baseline IGA scores (mean ± SD) were 9 ± 3 (range: 5-13). The use of the 5% hyaluronic acid significantly reduced the IGA score by 67% at week 4 and by 83% at week 8. 5% hyaluronic acid has been effective in reducing erythema, scales, seborrhea, and itching (tabl.1), (figure 1).

Facial seborrheic dermatitis, characterized by erythema and or flaking/scaling in areas of high sebaceous activity, affects up to five percent of the population.
Despite ongoing study, the cause of the condition is yet unknown, but has been associated with yeast colonization and resultant immune derived inflammation
Facial seborrheic dermatitis is a very common presenting problem in dermatology patients. The papulosquamous disorder is usually found on the scalp, face, or trunk, all of which are sebum-rich areas [13].
The condition is associated with an abnormal immune response caused by a decrease in the titers of antibodies of auxiliary T cells, phytohemagglutinin, stimulation with concanavalin. Multiple factors have been identified as predisposing to facial seborrheic dermatitis, and understanding of the causes and pathogenesis of facial seborrheic dermatitis has improved thanks to advances in microbiological and analytical techniques.
The key factors of proliferation of Malassezia yeast, the state of the epidermis, and high levels of sebum secretion interact, along with other factors, to potentially culminate in facial seborrheic dermatitis.Topical antifungals are another therapeutic mainstay; however, some strains of Malassezia globosa and M. restricta, the etiological agents most associated with seborrheic dermatitis, are resistant to azole antifungals, resulting in treatment failure in clinical practice Susceptibility testing of Malassezia species using the urea broth microdilution method [15]. The components break down products that actively stimulate the production of beta-defensin 2 (DEFβ2) and induce an antibacterial response to allow for healing in the skin’s epithelium.
Common therapies often include a topical steroid, which can have untoward effects, such as atrophy, telangiectasias, acne, and perioral dermatitis.
The goal of treatment should be to provide safe and effective treatment that improves symptoms, reduces recurrence, and causes minimal side effects.
There are three main pharmacological treatments for seborrheic dermatitis: keratolytics, anti-inflammatories, and antifungals.
Topical steroids and calcineurin inhibitors reduce inflammation and antifungal agents reduce Malassezia populations. In addition, some agents, such as ketoconazole, have additional anti-inflammatory and anti-androgenic properties. Although these treatments have been demonstrated to be effective, the need for long-term treatment can cause side effects and cosmetic problems that may limit their use. In these cases, the use of topical non-pharmacological therapies may be considered.
Non-pharmacological treatments include cosmetics, cosmeceuticals, and medical devices. The definitions are imprecise, which means that regulations vary from country to country.
Hyaluronic acid (HA), a neutral salt, is a naturally occurring highly conserved polysaccharide found in the skin’s tissue.Numerous medical applications, including wound care, have seen improvements as a result of leukocyte, fibroblast, and endothelial cell migration and activation. The efficacy of topical 5 % hyaluronic acid gel on recurrent oral ulcers: comparison between recurrent aphthous ulcers and the oral ulcers of Behçet's disease [15-22].
This study evaluated the efficacy of 5% hyaluronic acid crem in the treatment of facial seborrheic dermatitis.
Of the parameters, pruritus showed the most pronounced improvement at 8 weeks of treatment. Other parameters also showed improved compared to the baseline, but not as pronounced. A multi-targeted therapy effectivenes whit hyaluronic acidhas anti-inflammatory, sebum-controlling, and anti-scaling properties is ideal for the management of the signs and symptoms of seborrhea and seborrheic dermatitis could be useful for daily routine use, controlling the symptoms without use of pharmacological therapy
Conclusion: In patients diagnosed with facial seborrheic dermatitis use of 5% hyaluronic acid crem has been effective in reducing erythema, scales, seborrhea, and itching.The condition improved from baseline in 92.3% of subjects.
Conflict of interest and financial disclosure
The author declares that he has no conflict of interest and there was no external source of funding for the present study. None of the authors have any relevant financial relationship(s) with a commercial interest.
CONSENT STATEMENT: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The work was not funded.
Ethical approval
The study was reviewed and approved by the Ethics Committee of the of the Yerevan State Medical University after M. Heratsi (protocol N16, 5.10.17) and in accordance with those of the World Medical Association and the Helsinki Declaration. Informed consent Patients were informed verbally and in writing about the study and gave written informed consent.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
