
Research article | DOI: https://doi.org/10.31579/2692-9392/089
Cumhuriyet University Faculty of Health Sciences Department of Nursing/ Sivas/Turkey, ORCID: 0000 0002 2235 8084
*Corresponding Author: GÜRCAN ARSLAN, Cumhuriyet University Faculty of Health Sciences Department of Nursing/ Sivas/Turkey.
Citation: GÜRCAN ARSLAN (2022). Evaluation of the Difference Between non-COVID-19 Pneumonia and COVID-19 Pneumonia Nursing Care. Archives of Medical Case Reports and Case Study, 5(3); DOI:10.31579/2692-9392/089
Copyright: © 2022 GÜRCAN ARSLAN, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 October 2021 | Accepted: 03 January 2022 | Published: 10 January 2022
Keywords: chest diseases; hypertension; inflammatory
Aim
This study was aimed to contribute to the nursing care of COVID-19 pneumonia by determining the similarities and differences in nursing care for COVID-19 pneumonia and non-COVID-19 pneumonia.
Methods
This study aimed to retrospectively evaluate the nursing care applied to 84 pneumonia patients who were hospitalized in Sivas Numune Hospital Chest Diseases Service between 2018-2019 and 81 in patients with COVID-19 pneumonia between May and November 2020.
Results
COVID-19 pneumonia patients were older than non-COVID-19 pneumonia patients (p<0.001), and the majority of patients were hypertensive and diabetic (p<0.05). The most common symptom for COVID-19 pneumonia patients is dyspnea (p<0.05) while for non-COVID-19 pneumonia patients it is fever (p<0.001). 77.8% of COVID-19 pneumonia patients but non-COVID-19 pneumonia patients had bilateral pneumonia with the feature of multiple mottling and ground-glass opacity on CT images. LDH, CRP, PCT, AST/ALT, and D-dimer levels increased significantly higher in COVID-19 pneumonia patients than in COVID-19 pneumonia patients (p<0.001). 26.2% of non-COVID-19 pneumonia patients, all of COVID-19 pneumonia patients' liver function tests, and coagulation factors were regularly monitored. COVID-19 pneumonia patients received %100 of patients antiviral drugs, 74.1% of patients corticosteroids, 92.5% of patients anticoagulant, 39.5% psychological support different from non-COVID-19 patients.
Conclusion
D-dimer and procalcitonin elevation in patients who develop pneumonia due to COVID-19 may be indicators of the need for intensive care in nursing care. Besides, it was concluded that liver functions and DVT follow-up in COVID-19 pneumonia should be included in nursing care.
The new type of coronavirus (COVID-19) emerged in Wuhan, People's Republic of China, in December 2019 and was recognized as a pandemic by the World Health Organization (WHO) on March 11, 2020. While there were approximately 72 million people infected with COVID-19 in the world until 30 Januray 2021, more than 2.5 million people who died were recorded [1,2].
While relieving the symptoms of patients who are admitted to healthcare institutions and who are positive for COVID-19 is considered a priority, especially antiviral drugs are used and patients under treatment are isolated to prevent the spread of the virus [3,4].
COVID-19 is quite new in nursing care because it is a new disease. Nurses in the care of patients infected with COVID-19; continue to provide symptom relief in line with their experiences [5,6]. Nurses, who are at the forefront of combating COVID-19, need evidence-based practices in their care. The definition of many complications, including pneumonia, caused by COVID-19 is quite new [2,6]. It has been reported that pneumonia develops in approximately 5% of COVID-19 cases and most of these patients need intensive care and most of the deaths are related to this disease [1,2,7].
Nursing care applied to these patients is based on both COVID-19 patient procedure and patient care with pneumonia [2,5,8-10]. The symptoms of pneumonia caused by the virus are similar to symptoms of influenza virus-related respiratory diseases are very common, especially in winter 11-13]. However, the laboratory and radiological findings of this new disease differ from the findings of pneumonia [13,14]. However, clinical manifestations are very important for identifying patients infected with COVID-19 and applying treatment and nursing care correctly. COVID-19 pneumonia nursing care matures during the pandemic process. Therefore, nurses need guidelines for this new disease and its developing complications.
This study was conducted to contribute to the nursing care of COVID-19 pneumonia by determining the similarities and differences in nursing care for COVID-19 pneumonia and non-COVID-19 pneumonia.
2.1 Study design and participants
This study aimed to retrospectively evaluate the nursing care applied to 84 pneumonia patients who were hospitalized in Sivas Numune Hospital Chest Diseases Service between 2018-2019 and 81 in patients with COVID-19 pneumonia between May and November 2020.
Research approval (2020-05/28) was granted by the ethics board of Sivas Cumhuriyet University Faculty of Medicine/Turkey.
2.2 Research Inclusion and Exclusion Criteria
(1) being over 18 years (2) confirmed COVID‐19 based on a positive RNA test (3) presence of ground-glass opacity in computed tomography (CT); considered compatible with COVID-19 pneumonia. (4) Non-COVID-19 cases of pneumonia.
In consideration of the complex factors affecting pregnant women, they were excluded andthis file data was not investigated when there was missing information in file records.
2.3 Data Collection
Clinical charts, Nursing records, laboratory findings, and chest X-ray records were reviewed by the researcher for all COVID-19 pneumonia and non-COVID-19 pneumonia patients from May to November 2020. To decrease the possible effects on laboratory results, evaluated these patients with similar duration of COVID-19 pneumonia and non-COVID-19 pneumonia in this study. Clinical, radiological, and laboratory data were accessed from hospital records. The researcher did not communicate with patients or family. The patients' records were not investigated when there was missing information in the records.
2.4 Statistical Analysis
Categorical data were described as continuous data as median with interquartile range (IQR) and percentages (%). Nonparametric comparative test for continuous data and χ2 test for categorical data were used to compare variables between groups. Differences were considered significant at p < 0>
Demographic Characteristics of Cases
Demographic characteristics of cases are shown in Table 1, 81 COVID-19 pneumonia patients and 84 non-COVID-19 pneumonia patients had included in this study. The mean age was 68.40± 13.29 (32-94) years and 58.85± 14.79 (27-78) years in COVID-19 and non-COVID-19 patients. There were 26(32.1%) female COVID-19 pneumonia patients, and 30(35.7%) female non-COVID-19 pneumonia patients. COVID-19 pneumonia patients have the highest hypertension (60.4%), non-COVID-19 patients have COPD (30.9%) comorbidity.
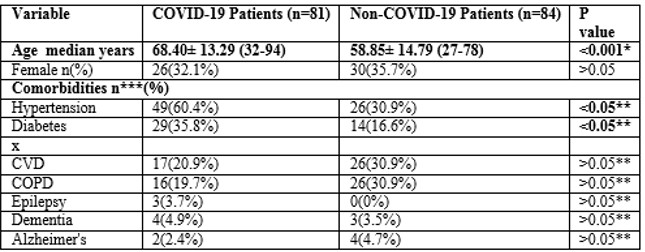
COVID-19, coronavirus 2019; Chronic obstructive pulmonary disease. COPD; Cardiovascular diseases, CVD
p* Mann-Whitney U test
p** chi-square test
n*** More than one answer was given and percentages were taken from n.
Illness Features of Patients
Illness features of patients are shown in Table 2. On admission, the most common symptoms of COVID-19 pneumonia patients were (75.3%) dyspnea, (34.5%) fever, and non-COVID-19 pneumonia patients have the most common symptoms of (80.9%) fever and (66.7%) cough. Less common symptoms of illness were headache (9.8%, 13.1%) and sore throat (12.3%, 1.2%) in COVID-19 pneumonia and non-COVID-19 pneumonia patients. There was a statistical difference between patients.
On admission, of the 81 COVID-19 patients, 62 (73.8%) had bilateral involvement, 75 (92.5) multiple lobular ground-glass opacity (Table 2) in COVID-19 patients. In comparison, of 84 non-COVID-19 patients, only 22 (26.1%) had bilateral involvement and, except for 3(3.5%) patients who had multiple patchy and mottling shadows with partial ground-glass opacity (Table 2). There was a statistical difference between patients.
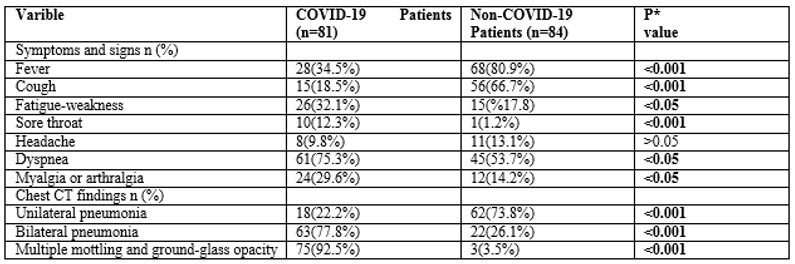
COVID-19, coronavirus 2019; CT, computed tomography
P* chi-square test
Laboratory Test Results of the Patients
Laboratory test results of the patients are shown in Table 3. In this study, white blood cell (WBC) counts of investigated COVID-19 pneumonia patients were in the normal range (8.99±4.20) but non-COVID-19 pneumonia patients were not in the normal (12.36±0.72). There was a statistical difference between patients.
Compared with non- COVID-19 pneumonia, COVID-19 pneumonia patients had higher levels of ratio of neutrophils (>0.05), aspartate aminotransferase (AST) (<0>0.05) (Table 3).
Nursing Care and Treatments
Nursing Care and treatments of the patients are shown in Table 4. Similar nursing practices applied to COVID-19 and non-COVID-19 patients; isolated room, maintain rest-sound sleep, maintain personal hygiene, oral care, monitor vital signs, management fever, maintain SpO2>90%, maintain acid-base balance, 30-45 degrees head-end elevation, assessing the risk of pressure sores, provide fluids and nutritious high protein diet with vitamins and minerals. However different nursing practices applied to COVID-19; pron position, follow-up of patients who need dialysis treatment due to pneumonia, follow-up coagulation profile (Procalcitonin, LDH, D-dimer), liver-renal function (ALT, AST, Creatine, Urea, Albumin), assessing signs of DVT and psychological support. 60 patients (74.1%) received corticosteroid, 49 patients (60.4%) received expectorant, 41 patients (50.6%) received vitamin C or B complex, 75 patients (92.5%) received anticoagulant. All of the COVID-
19 pneumonia patients received the antiviral drug, while non-COVID-19 pneumonia patients received antibiotics (Table 4).
In this article, the nursing care of COVID-19 pneumonia and non-COVID-19 pneumonia patients was retrospectively reviewed.
This study was found that male patients had a higher incidence of disease COVID-19 pneumonia. The mean age of COVID-19 pneumonia patients was significantly older than that of non-COVID-19 pneumonia patients (p<0>
The clinical data showed that dyspnea, fever, cough, and fatigue were the most common symptoms in both groups of patients. However, the most common symptom for COVID-19 pneumonia patients is dyspnea (p<0>
In laboratory findings, the count of WBC (p<0>0.05) in most COVID-19 pneumonia and non-COVID-19 pneumonia patients has changed (Table 3). This result suggests that COVID-19 pneumonia and other respiratory virus infections developed inflammatory immune responses [3].
This study results that COVID-19 pneumonia patients, LDH, CRP, and PCT levels increased significantly (p<0>0.5 µg/L [15,19]. In a recent study, COVID-19 patients treated in intensive care had a higher level of LDH, CRP, and PCT [17].
In the COVID-19 pandemic, determining the patient who will need intensive care in advance can provide significant contributions in terms of time gain in nurse care and the conduct of the intensive care process.
This study data showed that levels of liver function-associated markers (ALT and AST) were significantly higher in COVID-19 pneumonia patients than in COVID-19 pneumonia patients (p<0>
This study data showed that level of D-dimer was significantly higher in COVID-19 pneumonia patients than in non-COVID-19 pneumonia patients (p<0>

COVID-19, coronavirus 2019; CT, computed tomography
P* Mann-Whitney U test
Dynamic changes of D-dimer levels during the disease were prognostic of poor outcome in Chinese patients [21,22]. Tang et al (2020) said that; a close correlation has been observed between blood levels of D-dimer and COVID-19 disease severity [23]. Changes in D-dimer levels can be monitored to evaluate the nurses' COVID-19 process.
When the nursing care given to COVID-19 pneumonia and non-COVID-19 pneumonia patients were evaluated; in addition to similar nursing care, it has been determined that different applications are performed due to laboratory and radiological findings (Table 4).
In this study, 26.2% of non-COVID-19 pneumonia patients in nursing care plans, all of COVID-19 pneumonia patients' liver function tests (AST, ALT, LDH) and coagulation factors (PCT, D-dimer) were regularly monitored (Table 4). In a large studies from China, patients with severe COVID-19 seem to have higher rates of AST/ALT, LDH [18,21,22].
Liver damage in patients with COVID-19 might be caused by the viral infection of liver cells since pathological studies in patients with COVID-19 confirmed the presence of the virus in liver tissue because angiotensin-converting enzyme 2 (ACE2), the entry cell receptor for SARS-CoV2 is expressed in both liver cells [24-28]. It is recommended that COVID-19 pneumonia patients should be monitored regularly in terms of AST / ALT and LDH values, to prevent liver damage and to start treatment early in nursing care. Almost all (92.5%) patients with COVID-19 pneumonia receive anticoagulant treatment in the patient files examined due to the study (Table 4). High coagulation indicators in COVID-19 patients reveal the need for anticoagulant therapy [28,29].
Also, it was determined in the study that DVT risk assessment was performed in nursing care applied to COVID-19 pneumonia patients (Table 4). Studies have reported large and small venous and arterial blood clots in COVID-19 patients [30,31]. Nurses should be careful about deep vein thrombosis. Mindful to carefully evaluate COVID-19 pneumonia patients for signs of clotting, such as unilateral swelling or redness [16,32].
According to the results of this study, some pharmacologic treatments are applied to COVID-19 pneumonia patients (all patients antiviral drugs, 74.1% of patients corticosteroids, 92.5% of patients anticoagulant) different from non-COVID-19 pneumonia patients (Table 4). Used antiviral drugs, had anti-inflammatory and Immunomodulatory effects and are found to be effective in the management of COVID-19 but some antiviral drugs are known to cause AV blocks, cardiomyopathies, and retail damage [33-35]. Nurses should closely cardiac monitor and regularly checks patients' QT intervals for these adverse effects [32].
Low-dose corticosteroid therapy should be employed in adult patients with COVID-19 disease [1,2]. The corticosteroid therapy has side effects therefore it is recommended to monitor vital signs and side effects [36,37]. This situation is and further studies are needed. The inclusion of family members in the educational process meets the international patient’s safety requirements and shows the nurse’s concern about patient care during and after the hospitalization [38-40]. In the nurse care plans examined in this study, it was determined that (39.5%) COVID-19 pneumonia patients need psychological support different from non-COVID-19 pneumonia patients (Table 4).
The uncertainty, fear, and anxiety caused by the fact that COVID-19 is a new disease [41,42]. In the study conducted by Mazza et al. (2020) it is stated that COVID-19 has negative effects on psychological health and this situation causes the disease to be experienced with more severe symptoms [42].
Nurses should care about not only the improvement of physiological symptoms but also their psychological well-being in the care of individuals infected with COVID-19. For this reason, enriching nurse care plans for methods of coping with stress can be a guide.
4.1 Limitations and further research
There are several limitations to this study. First, the sample size was very small and COVID-19 disease is new. Second, inability to access some patient files.
Based on the current study, future research may use a large sample coverage and follow-up approach in the treatment process to evaluate the effects of COVID-19 pneumonia. The reflections of laboratory findings on nursing care can be investigated more comprehensively at certain intervals during the treatment process.
COVID-19 pneumonia requires different nursing care from non-COVID-19 pneumonia due to differences in laboratory results and radiological findings. COVID-19 pneumonia draws attention with the high rate of liver function tests such as AST / ALT, LDH, infection markers in the blood and coagulation factors such as PCT and D-dimer during the hospital stay compared to non-COVID-19 pneumonia. These laboratory findings such as AST/ALT, LDH, PCT, and D-dimer elevation in patients who develop pneumonia due to COVID-19 may be indicators of the need for intensive care in nursing care. Besides, it was concluded that liver functions and DVT follow-up in COVID-19 pneumonia should be included in nursing care. There is an urgent need to establish a systematic and scientific system for the effective control and treatment of COVID-19 pneumonia, which is among the complications of COVID-19.
5.1 Relevance to clinical practice
Since COVID-19 is a new disease factor, it makes nurses who are at the forefront of controlling the pandemic with its symptoms, findings, and treatment process. In this study, it was determined that COVID-19 pneumonia and non-COVID-19 pneumonia differ in terms of signs and symptoms. Unlike non-COVID-19 pneumonia in COVID-19 pneumonia; liver function tests such as AST/ALT, LDH, infection markers in the blood, and coagulation factors such as PCT and D-dimer stand out with the increase. Regular follow-up of these values can contribute to the proper organization of the hospital stay by ensuring that nurses have information about patient prognosis. Also, as a result of these findings, it is thought that they may contribute to the prevention of complications such as DVT. In the care of COVID-19 pneumonia, it is seen that acute improvement of symptoms is prominent by taking advantage of the care experiences of nurses for viral diseases. For this reason, it is thought that guidelines should be established at the earliest stage to maintain effective COVID-19 nursing care.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
