
Research Article | DOI: https://doi.org/10.31579/2692-9562/090
Başakşehir Çam and Sakura City Hospital, Department of otorhinolaryngology, İstanbul/Turkey.
*Corresponding Author: Ahmet Baki, Başakşehir Çam and Sakura City Hospital, Department of otorhinolaryngology, İstanbul/Turkey.
Citation: Ahmet Baki, İsmail Çalıkoğlu, Alaaddin Aydın, Sercan Yüksel, Şahin Öğreden, et al., (2023), Evaluation of Smell Functions in Bariatric Surgery, J Clinical Otorhinolaryngology, 5(4); DOI:10.31579/2692-9562/090
Copyright: © 2023, Ahmet Baki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 22 February 2023 | Accepted: 09 March 2023 | Published: 17 March 2023
Keywords: bariatric surgery; smell test; olfactory function
Objective: To evaluate olfactory functions in patients undergoing bariatric surgery.
Materials and Methods: The study included 30 patients who undergone bariatric surgery. Patients with indications for bariatric surgery in the general surgery clinic were referred to the otolaryngology clinic for smell testing. Smell tests were performed on the patients before and during the first month after the operation in the otorhinolaryngology clinic.
Results: There were 18 female and 12 male patients in the study. The ages of the patients participating in the study ranged from 19 to 56, and the mean age was 36.4±10.8 years. Preoperative, the patients' threshold, identification, and total score values were 6,93±0,25, 6,73±0,63, and 6,83±0,35, respectively. Postoperative, the patients' threshold, identification, and total score values were 2,8±1,03, 6,7±0,59, and 4,75±0,7, respectively. There were statistically significant differences in comparing the threshold and total scores before and after surgery. (p=0.001) There were no statistical differences in the identification scores before and after surgery. (p=0,462)
Conclusion: Temporary smell disturbance scores may be seen in patients undergoing bariatric surgery.
Running Title: Olfaction, Bariatric surgery
Obesity has recently become an important public health problem all over the world. [1]
Obesity is an important risk factor for many diseases and can lead to sudden death. [2] Diet and lifestyle changes are made in the treatment of obesity. It has been shown that conservative methods alone are not effective in the morbidly obese patient group. [3] When combined with the lifestyle change, diet, and increased physical activities, bariatric surgery is seen as a very effective method for permanent weight loss. Obesity surgery applies to people with a BMI (Body mass index) of 40 or more and can apply to those over 35 but with other diseases. [4] Bariatric surgery is now the most widely used intervention for the treatment of human obesity. Numerous literature studies have shown its effectiveness in permanent weight loss and improvement in weight-related comorbidities. [5] Types of bariatric surgery can be divided into restrictive, non-absorbent or combined. Sleeve gastrectomy (SG) is a restrictive surgery that significantly reduces the size of the stomach and limits solid food and calorie intake. SG creates a vertical tube through the stomach, shrinking the stomach by over 80%. This procedure, whose prevalence is increasing rapidly, is the most frequently applied method in many countries. [6] It has been shown in previous studies that there are changes in olfactory functions after bariatric surgery. There was a 40% change in olfactory functions after RYBG (Roux-en-Y gastric bypass) and 21 percentage after LGS (Laparoscopic gastric sleeve). [7] We evaluated the olfactory functions of patients after bariatric surgery to contribute to the literature because there are very few studies evaluating olfactory functions after bariatric surgery and the existence of different results.
This study included 30 patients who were candidates for bariatric surgery. The study was conducted between October 2021 and October 2022. The participants were selected from the general surgery clinic on the basis of their bariatric surgery and then referred to the ENT clinic for olfactory testing. A detailed history was taken from all the patients, and a routine ear, nose, and throat examination was also performed. Patients with nasal septum deviation, acute or chronic rhinosinusitis, active upper respiratory tract infection, nasal polyposis, history of nasal surgery, allergic rhinitis, smoking, systemic diseases (e.g., diabetes mellitus, hypothyroidism, hypertension, chronic renal failure, and chronic liver failure), neurological diseases, lessthan 18 after LGS (Laparoscopic gastric sleeve). [7] We evaluated the olfactory functions of patients after bariatric surgery to contribute to the literature because there are very few studies evaluating olfactory functions after bariatric surgery and the existence of different results.
Smell assessment
The CCCRC test comprises of a butanol threshold and an identification as already reported. (9) It was administered preoperative and in the 4th week postoperative. Also 12th week for smell evaluation.
Butanol threshold test
The participants were given two glass bottles of the same color and uniform view, one of which contained water and the other a dilute concentration of butanol during the test. They were then ordered to close one nostril and place the tip of the first bottle quickly below the other one. The second bottle was then sampled in a similar manner, and the participant had to select which of the bottles contained something other than water. If the selection was incorrect, a more potent concentration of butanol was submitted along with the bottle having only water. Possible scores ranged from 0–9, but scores ≥7 were scored as 7 per the olfactory test protocol. For the final score, the average of both nostril scores was taken.
Identification test
Cinnamon, Vicks, chocolate, Turkish coffee, peanut butter, carbonate, soap, and baby powder were added to opaque bot- tles. The ability to sniff out Vicks showed unimpaired trigeminal nerve function, and all the subjects easily recognized it; therefore, it was not added to the final score. Possible scores ranged from 0 to 7. For the final score, the average of both nostril scores was taken.
Total score
Scores for the butanol threshold and identification tests were later averaged to reach a total score, which was classified as defined by Cain et al. [10]
Statistical analysis
The Statistical Package for Social Sciences version 22.0 software (IBM Corp.; Armonk, NY, USA). The suitability of the parameters to normal distribution was evaluated by the Shapiro-Wilks test. Descriptive statistical methods (mean, median, and standard deviation) were determined when evaluating the study data. The Wilcoxon test was used in the comparison of non-parametric data between the same groups. The Spearman rho test was used for correlation analysis of non-parametric data. The difference between the scores before and after surgery was used to evaluate the correlation between threshold score and the weight loss.
There were 18 female and 12 male patients in the study. The ages of the patients participating in the study ranged from 19 to 56, and the mean age was 36.4±10.8 years. While preoperative the threshold, identification, and total score values of the patients were 6,93±0,25, 6,73±0,63 and 6,83±0,35 respectively, postoperative, 2,8±1,03, 6,7±0,59 and 4,75±0,7. A statistically significant difference was found in comparing the threshold and total scores before and after surgery (p=0.001), but the identification score did not change. (p=0,462)
| Preoperative | Postoperative | |||
| N | mean±SD (min-max) | mean±SD (min-max) | p | |
| Threshold score | 30 | 6,93±0,25 (6-7) | 2,8±1,03 (1-5) | 0,001 |
| Identification score | 30 | 6,73±0,63 (5-7) | 6,7±0,59 (5-7) | 0,462 |
| Total score | 30 | 6,83±0,35 (6-7) | 4,75±0,7 (3,5-6) | 0,001 |
| Wilcoxin signed rank test, N:patients number, SD: Standart deviation, p≤0,005 | ||||
Table 1: Comparison of preoperative – postoperative smell scores (1st month).
The preoperative mean body mass index (BMI) was 46.3±6.11 (39,2-64.9). Postoperative 1st month BMI 40.3±5.23 (34-52.9). Between the threshold score and BMI significant, mild and positive correlation was found in the correlation analysis. (r correlation value= 0.485.) (p value= 0.001) (p≤0.001) Postoperative first and third month mean percentage TWL is 12.4±4.5 and 22.6±5.1, respectively.
| Preoperative | Postoperative | ||||
| N | mean±SD (min-max) | mean±SD (min-max) | r | p | |
| Threshold score | 30 | 6,93±0,25 (6-7) | 2,8±1,03 (1-5) | 0,485 | 0,001 |
| BMI | 30 | 46,3±6,11(39,2-64,9) | 40,3±5,23 (34-52,9) | ||
| Spearman’s rho test, N: number of patients, Min: minimum, Max: maximum, BMI (Body mass index), r: correlation value, p≤0.01 | |||||
Table 2: Correlation analysis between weight loss and threshold scores (1st month).
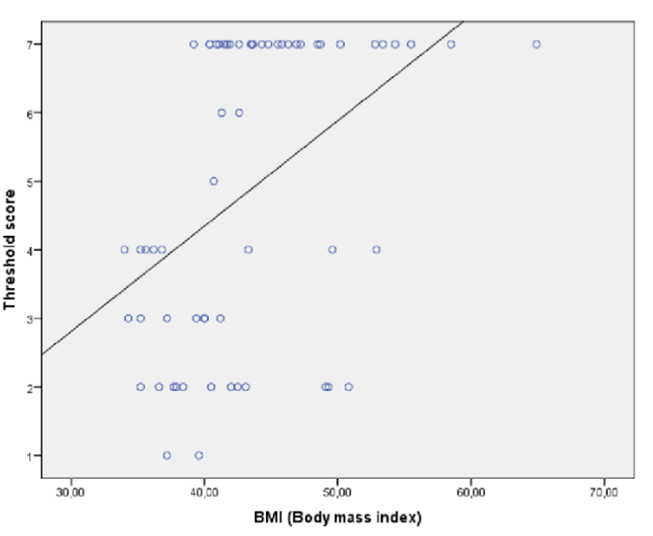
Figure 1: The correlation between BMI and threshold score. (r:correlation value:0,485) p=0.001. Correlation; significant, positive, and mild.
Obesity and obesity-related comorbidities cause increasing medical and socio-economic problems not only in developed countries but also in developing countries. [11] Treatment of obesity diet, exercise, lifestyle changes, specific drugs and bariatric surgery are can be used. Today, bariatric surgery indications are limited to morbid obesity, but it is also applied to obese patients with additional diseases such as cardiovascular and type 2 diabetes in patients who do not include the morbidly obese category (BMI 35 kg/m2 ≤). [12,13] Bariatric surgical procedures can be classified into three different types restrictive, malabsorptive, or combined. Gastric sleeve surgery (SG) was initially used as a first-line procedure for the duodenal switch (DS) but is now a stand-alone procedure that can significantly reduce stomach size. This operation, whose prevalence is increasing, is the most commonly used operation in many countries. [6] Roux-en-Y- is a malabsorptive and restrictive procedure that bypasses a large part of the stomach in gastric bypass (RYGB) surgery. [14] Besides obesity surgery, metabolic surgery methods have recently been applied, improving metabolic syndromes. The primary goal of bariatric surgery is to lose weight, but metabolic surgery's goal is to treat metabolic syndrome. After obesity and metabolic surgery, changes are observed in the smell and taste functions of the patients. [15] The sense of taste is governed by the gustatory system in the brain. There are very important connections between the olfactory and gustatory systems. [16] The comparison of RYGB and ileal interposition showed that RYGB reduced preference for higher concentrations, while ileal interposition had no effect on taste preference or weight loss. [17] It has been shown that there are changes in the sense of taste in patients who have undergone RYGB operation. In a bariatric surgery study in which the perception and recognition thresholds of various taste stimuli were evaluated, a significant decrease in bitter and sour taste thresholds was observed in the pre- and postoperative evaluations of patients who underwent RYGB operation, but no significant decrease was observed in sweet and salty tastes. [18] After the RYGB operation, there was an increase in the thresholds of sweet tastes by almost two times, while no change was detected in bitter tastes. [19] In comparing salty foods undergoing patients' RYGB operation, there was no difference in the threshold values before and after the operation. [20] The taste acuity study among RYGB and VSG (vertical sleeve gastrectomy) patients showed that RYGB patients had a significantly higher threshold for sourness. [21] In patients who underwent LGS, an increase was observed in all parameters of the Sniffin Sticks test at the 6th month postoperatively. [22] In other studies conducted with the same test, in comparisons before and after surgery in RYBG and LGS patients, only an increase in threshold values was found in LGS patients. In contrast, no change was found in identification and determination values. [23] In RYGB and LGS patients with a very low sense of smell, it was determined that the smell scores reached the levels of normal individuals after six months. [24] Non-specific olfactory changes were detected in 54% of patients after bariatric surgery. It was observed that the most smell change was in fatty, sweet and meaty foods. [25] There are very few studies in the literature evaluating olfactory functions after bariatric surgery. Studies on bariatric surgery have mostly been based on taste evaluations. As stated above, there are studies in which there are very important relationships between taste and smell. In these studies performed with many surgical techniques, we performed the study using the VSG (Vertical sleeve gastrectomy) surgical technique. It is known that the hypothalamus is involved in olfactory activity. [26] The lateral hypothalamus is the junction of many reciprocal pathways of the hypothalamic neuropil between the limbic forebrain and the limbic midbrain and a motor control system. [27] Histological studies have shown close relationships between the hypothalamus and the olfactory system. [28] The connections between the olfactory system and the hypothalamic system play a role in the modulation of feeding behavior. [29] Gastric distension affects the activity of lateral hypothalamic neurons that are sensitive to olfactory stimuli. [30] Lateral preoptic-lateral hypothalamic neuronal activity can be modulated by vagus nerve stimulation and gastric distension. [31] Both the olfactory system and the vagus nerve play a role in the regulation of food intake. [32] Vagus nerve stimulation causes impulse generation in the homolateral olfactory bulb. The discharge frequency of homolateral olfactory bulb neurons is modulated by single-pulse and sequential stimulation of the vagus nerve. This suggests that the gastrointestinal tract and the olfactory bulb are connected via the vagus nerve. [33] It has been shown that there is an oligosynaptic pathway between the vagus nerve and the olfactory bulb. [33] It has been shown that cholinergic elements in the olfactory bulb may originate from more caudal parts of the brain such as the olfactory tubercle and lateral preoptic area. [34] The presence of cholinergic cell bodies in the posterior hypothalamus has been demonstrated. [34] The vagus is a cholinergic pathway. [34] The activities of hypothalamic neurons are modulated by olfactory stimulation. [34] The hypothalamus receives sensory information from the stomach via the vagus nerve. [34] Distension of the gastric walls alters the activity of the olfactory bulb unit. [30] Sensory information from the stomach is transmitted to the brainstem via gastric vagal afferents the central terminals where the brainstem enters via the tractus solitarius and synapses on the nucleus tractus solitarius (NTS) neurons. [30] VSG causes minor damage to the gastric vagus and the antiobesity effect of this surgery is largely dependent on the distension of this surgery. [30] Hormonal changes are a major factor in weight loss in RYGB operation. The accompanying neural changes underlying the effects on food intake are still poorly understood. [35]
In our study, we evaluated the smell scores of the patients before and after the operation with the butanol smell test. In the olfactory test evaluation of the patients, we found only a decrease in threshold scores at the end of the first month. These threshold scores returned to preoperative levels in 3rd month. Studies have shown changes in both the sense of taste and the sense of smell after bariatric surgery. The existence of a relationship between the sense of taste and smell has been shown in many studies. It has been shown that the vagal nerve is affected due to gastric distension or direct neurological damage after bariatric surgery. The relationship between the vagal nerve and the olfactory bulb is clearly demonstrated. It has been shown that there is no vagal nerve damage in the VSG operation; it is affected due to distension. In our study, the deterioration in olfactory functions in the patients who underwent VSG operation in the 1st month after the operation and their smell function return to normal levels in the 3rd month may be due to the change in vagal nerve functions after gastric distension.
After bariatric surgery, changes are observed in the olfactory functions of patients. There are very few studies in the literature showing the relationship between smell and bariatric surgery, and we aimed to contribute to the literature. It can be said that patients undergoing bariatric surgery may experience deterioration in their olfactory functions, which is temporary. In order to demonstrate this situation, more comprehensive studies may be needed to evaluate the relationship between this operation and olfactory functions.
Financial disclosure: There is no financial support.
Conflict of Interest: There is no conflict of interest in this article
Ethical approval: All procedures performed in studies involving human participants were by the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the ethical research committee of the Başakşehir Çam and Sakura City Hospital in Istanbul.
Routine informed consent was obtained from all patients before the hospitalization and also inform consent from the individuals of the control group was obtained in the study. There is no support source that requires confirmation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
