
Research Article | DOI: https://doi.org/10.31579/2642-9756/022
1* Department of Obstetrics and Gynecology, Faculty of Medicine, Tanta University, Tanta, Egypt.
2 Department of Diagnostic Radiology, Faculty of Medicine, Tanta University, Tanta, Egypt.
*Corresponding Author: Ahmed M.Hagras, Lecturer of Obstetrics and Gynecology, Faculty of Medicine, Tanta University, Tanta, Egypt.
Citation: Ahmed M.Hagras., Neveen S. Shaker. (2020) Evaluation of International Endometrial Tumor Analysis Sonographic Criteria in diagnosis of Endometrial Carcinoma. J Women Health Care Issues, 3(2); Doi:10.31579/2642-9756/022
Copyright: © 2020 Ahmed M.Hagras, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 February 2020 | Accepted: 22 February 2020 | Published: 26 February 2020
Keywords: obstetrics & gynecology; diagnostic radiology; endometrial carcinoma
Postmenopausal vaginal bleeding is a sign that should not be Ultrasound imaging has become an effective diagnostic tool of gynecological practice throughout the years. Endometrial diagnosis typically involves invasive investigational approaches. Today, however, with the advent of high-resolution transvaginal ultrasound and Doppler ultrasonography (non-invasive diagnostic tool), is an alternative candidate to replace invasive approaches.
The aim of this study is to evaluate the contribution of the terms and definitions described by the IETA group when designing a malignancy model for better diagnosis of malignancy in cases with postmenopausal uterine bleeding.
In the present study 120 patients with postmenopausal bleeding were included in the study. The study was conducted from April 2017 to April 2019 at Tanta University hospitals, Obstetrics & Gynecology and Diagnostic Radiology departments.
Both patients were subjected to the following: full history taking, general examination, local examination, 2D transvaginal ultrasonography, Doppler study, hysteroscopy examination, endometrial biopsy. Symptomatic postmenopausal women with endometrial thickness > 5 mm have been chosen because women with a lower endometrial thickness have a very low incidence of cancer and a prospective evaluation.
In this study:
Conclusion: We may conclude that: applying a malignant model for postmenopausal bleeding cases allows for easy classification of cases into low and high risk, with the ability to restrict the invasive procedure on dangerous cases only for better diagnosis of endometrial cancer.
Postmenopausal bleeding (PMB) in both the general and hospital settings is a serious clinical issue [1].
It is estimated that about 90–95% of postmenopausal women with endometrial cancer report a vaginal bleeding experience, while about 10% of postmenopausal women report an intrauterine malignancy. Therefore, a postmenopausal vaginal bleeding is a warning not to be ignored. [2]
In this regard a good clinical practice provides, as first diagnostic step, a transvaginal ultrasound in order to discriminate women at high or low risk of malignancy. But in order to obtain an efficient ultrasound report we must solve certain problems that will be discussed in the following.
Most reports describing uterine cavity ultrasonography are limited and sometimes contradictory, the lack of standardization of words and meanings used to define endometrial ultrasound results and uterine cavity makes the meta-analysis of small studies meaningless [3].
there is no absolute diagnostic consensus on the appearance of endometrial cancer. Sometimes abnormal appearing masses may not be carcinoma and small foci of carcinoma may be present in simple lesions [4,5].
The International Endometrial Tumor Analysis (IETA) group, established in Chicago in 2008, has created a common consensus to agree on terms and definitions to identify ultrasound findings in the uterine cavity and to establish guidelines to promote the prediction and diagnosis of endometrial disease [6].
Several studies try to use variables other than endometrial thickness e.g. the gray-scale ultrasound morphology of the endometrium, the vascularization of the endometrium as assessed by Doppler ultrasound and clinical variables, in order to discriminate between benign and malignant endometrium in women with postmenopausal bleeding and improve the diagnostic performance of the procedures [7].
Finally, trials including patient characteristics and sonographic characteristics were conducted to design a model for endometrial cancer and then to estimate its risk and clinical usefulness. Some authors are using, as study participants, all postmenopausal women with vaginal bleeding, whereas other authors included only symptomatic postmenopausal women with an endometrial thickness at risk of intrauterine malignancy, the majority of these studies showed fair outcomes with an improvement of diagnostic performance in detecting endometrial cancers. However, up to date, these models are not yet validated externally [8].
Aim of the work:
To detect the diagnostic accuracy of transvaginal ultrasound in detecting endometrial cancer has been questioned in the most recent meta-analysis that justifies further studies in order to get simple, no invasive and valuable method in screening women with post-menopausal bleeding.
Patients and methods:
It was Prospective cross-sectional study. The study was conducted from April 2017 to April 2019 at Tanta University hospitals, Obstetrics & Gynecology and Diagnostic Radiology departments. 120 patients with postmenopausal bleeding selected from the attendees of the outpatient Gynecology clinic of the Department was recruited in this study.
Inclusion criteria:
(1) Natural menopause; defined as 1 year of absence of menstruation in women older than 40 years provided that the amenorrhea was not explained by medication or disease.
(2) Postmenopausal bleeding; defined as any vaginal bleeding in a postmenopausal woman not on hormone replacement therapy.
Exclusion criteria:
Ethical consideration: They were properly counseled & signed informed consent.
All patients were submitted to the following:
CBC, LFT, KFT, PT, PTT, INR, Viral marker.
4. Transvaginal sonography:
Examination was performed with endovaginal transducer of 4-7 MHz frequency on volusion 730 pro machine (GE Healthcare, Austria) after complete emptying of the urinary bladder.
All pelvic organs were assessed as the following:
The uterus: its central location and large size in the pelvis was used as a landmark for orientation, it is a hollow thick muscular organ, pear shaped situated in true pelvis between urinary bladder anterior and rectum posterior, the wall of the uterus is composed of 3 layers: endometrium, myometrium, perimetrium.
Ovaries, Fallopian tubes and Pelvis: TVS allowed us to assess the presence or absence of free fluid in Douglas pouch, and the presence of lesions within neighboring organs as the bladder or rectum.
5. DOPPLER study:
The endometrial vasculature was scored using the International Endometrial Tumor Analysis (IETA) color score (score of 1 is given when no color flow signals, score of 2 when only minimal color can be detected, score of 3 when the color is mild, score of 4 when the color is abundant), and also its pattern described in the (IETA) terms Single vessel, Multiple dominant vessels, Scattered vessels.
6. Hysteroscopy:
After the sonographic and Doppler tests, diagnostic hysteroscopy was performed for all patients. Hysteroscopic controlled biopsy was taken under local anesthesia (para cervical block) or general anesthesia from suspected endometrial areas where appropriate. The endometrial examination offers a tissue diagnosis that directs further management Then sonographic findings have been compared to the final histopathology
Statistical analysis:
Data collected throughout history, basic clinical examination, sonographic reports and histopathology reports were analyzed with (SPSS) version 20.
Quantitative results were represented as mean±standard deviation (SD) data were analyzed by independent t-test, paired t-test, using univariate analysis. In malignant situations, the receiver operating characteristic (ROC) curve was done to determine the best cutoff value. P-value was deemed meaningful if < 0>
Results:
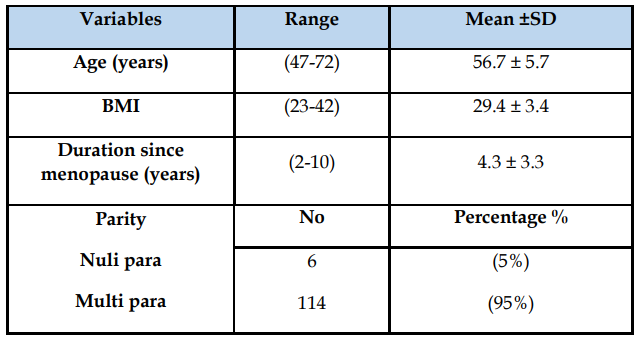
In this study (patient characters): mean values of the clinical variables (Table 1) were: age 56.7, BMI 29.4, Duration since menopause 4.3.
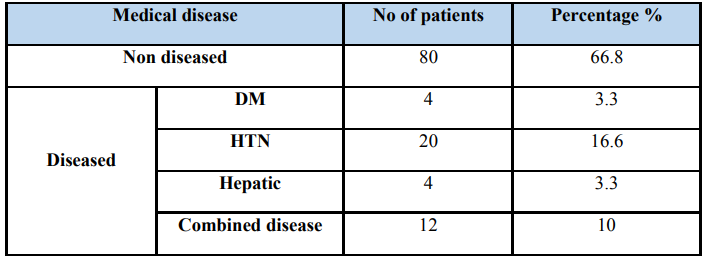
66.8% of patients have no medical disease while, the most frequent medical disorder recorded in diseased patients was hypertension (16.6%) as in Table 2.
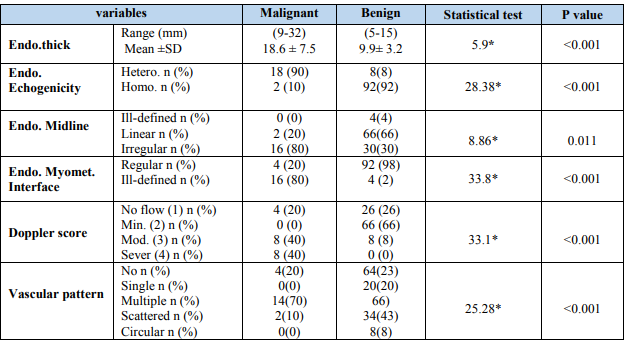
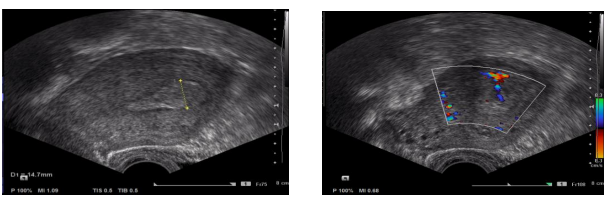
The most common lesions were benign in nature (specially the endometrial hyperplasia with highest frequency about 33%) while the endometrial carcinoma was only 16.7%) (Table 3). Including clinical variables (Age, Parity, BMI, HPN and Diabetes) shows a statistically significant difference between benign and malignant cases. While (duration since menopause, hepatic disease and combined disease) the table shows statistically non-significant differences (Table 4). The mean endometrial thickness in malignancy cases (18.6 ± 7.5). (Figure 1&2).
The most frequently identified sonographic variables with malignancy were endo-heterogenous. Echogenicity, and endo irregularity. Midline, the endo is poorly defined. end. myo. System, Doppler score > 2, multiple vessel patterns and all show a significant difference between table of benign and malignant cases (Table 5). Endo. Endo. Power. (1.2 cm), endometrium heterogeneous, irregular. Endo. Endo. Midline, endo is ill-defined. Myo. myo. Browser (Table 6). Score cut off (≥10) had the largest area under receiver operator curve and had the best accuracy for detection of malignancy Area under curve (AUC) =0.94 (Table 7).


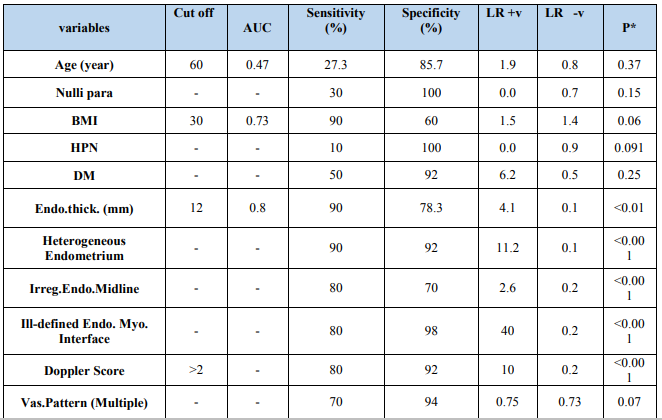
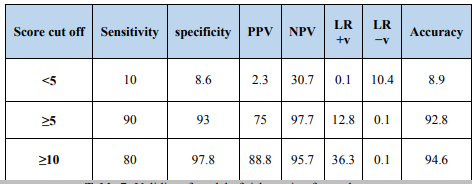
Score cut off (≥10) had the largest area under receiver operator curve and had the best accuracy for detection of malignancy
Area under curve (AUC) =0.94 table (7)
Confidence interval (95%)

Conclusion:
We can conclude that:
• Words used to characterize endometrial sonographic characteristics identified by the (IETA group) are clinically useful and appropriate for endometrium evaluation using a standardized measuring technique.
• The implementation of a malignancy model for postmenopausal bleeding cases makes it easy to distinguish cases into low-risk cases with the ability to restrict the dangerous invasive procedure
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
