
Research Article | DOI: https://doi.org/10.31579/2690-1919/274
1 Department of medical laboratory Science, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Awka, Nigeria.
2 Department of Chemical Pathology, Faculty of Medicine, Nnamdi Azikiwe University, Awka, Nigeria.
3 Department of Human Biochemistry, Faculty of Basic Medical Sciences, Nnamdi Azikiwe University, Awka, Nigeria.
*Corresponding Author: Ogbodo Emmanuel Chukwuemeka. Department of medical laboratory Science, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Awka, Nigeria.
Citation: Analike Rosita Chinechelum, Okwara John Ekenedilichukwu, Meludu Samuel Chukwuemeka, Analike Rosemary Adamma, Ogbodo Emmanuel Chukwuemeka. (2022). Evaluation of dyslipidemia prevalence among undergraduate university students., J. Journal of Clinical Research and Reports, 12(1) DOI:10.31579/2690-1919/274.
Copyright: © 2022 Ogbodo Emmanuel Chukwuemeka. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 October 2022 | Accepted: 18 October 2022 | Published: 27 October 2022
Keywords: dyslipidemia; BMI; blood pressure; age; lipid profile
Dyslipidemia has grown to be a significant global public health issue particularly in developing nations like ours, as a result of rising trends in dietary habits, physical inactivity, and obesity, which each play essential roles in the development of cardiovascular diseases. The purpose of this cross-sectional study was to determine the prevalence of dyslipidemia among undergraduate students at Nnamdi Azikiwe University in Nnewi. Two hundred (200) students between the ages of 18 and 30 who appeared to be in good health were selected at random. After that, each participant provided a fasting blood sample of five milliliters (5ml) for the evaluation of serum total cholesterol (TC), triglycerides (TG), low density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) using standard laboratory techniques. Additionally, the body mass index (BMI) and the systolic and diastolic blood pressure readings were calculated. 44 percent of participants were males and 56 percent were females, with an average age of 22.41 ±1.68 years. While 3% of the participants were underweight, 27% of them were overweight, and 6% were pre-obese, the majority of them (64%) had a normal BMI. Three percent (3%) of the participants had pre-hypertension, whereas 97% of the participants had normal blood pressure. The prevalence of hypercholesterolemia, hypertriglyceridemia, low HDL-C, and high LDL-C among the participants, as defined by the World Health Organization, was 39.5%, 26.5%, 4%, 12.5%, and 16.5%, respectively. SBP Vs DBP, DBP Vs Weight, DBP Vs BMI, Weight Vs BMI, TC Vs TG, TC Vs HDL, and TC Vs LDL all had significant positive correlations (p<0.05) while SBP Vs TG, SBP Vs HDL, and TC Vs LDL all had significant negative correlations (r=-0.148, p=0.036, and r=-0.203, p=0.004). The female sex was strongly related with dyslipidemia (48.2%), whereas the male sex was not (28.4%). As a result, there is a pressing need to educate the public about the essential changes in food habits and overall lifestyle to maintain cardiovascular health.
The abnormal amount of lipids (e.g. triglycerides, cholesterol, and/or fats phospholipids) in the blood is known as dyslipidemia. Elevated plasma levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG), as well as reduced plasma levels of HDL cholesterol (HDL-C), are all characteristics of dyslipidemia (Manjunath et al., 2013; Bibbins-Domingo et al., 2016). Type 2 diabetes mellitus, hypothyroidism, excessive alcohol consumption, cholestatic liver disease, renal disease, smoking, and obesity are all conditions that can result in dyslipidemia (Okaka and Eiya, 2013). Despite being a modifiable risk factor for cardiovascular disease (CVD), dyslipidemia is becoming more common. Cardiovascular disease is the leading cause of morbidity and mortality worldwide (GBD 2017 Causes of Death Collaborators, 2018), with a high prevalence in most countries but a higher burden on the populations of developing countries like Nigeria as a result of dietary changes, physical inactivity, and increased alcohol consumption, among other factors (Munsinguiz et al., 2020). Prevalence varies by region in Sub-Saharan Africa, with rates of more than 50% in Nigeria, Ghana, and Senegal, and 39.30 percent in Nigeria (Fatou et al., 2016). Dylipidemia is growing more frequent, although most people are unaware of it because they are not identified and thus not treated. This increases the risk to an already vulnerable group, exacerbating the morbidity, death, and medical expenses associated with cardiovascular disease.
The burden of cardiovascular disease is increasing in emerging nations like Nigeria due to the increasing prevalence of cardiovascular risk factors (Nnamudi et al., 2020). The heart and blood arteries make up the cardiovascular system (Farley et al., 2012). On the other hand, cardiovascular diseases are a group of conditions that affect the heart and blood arteries. Atherosclerosis is the main underlying pathology of cardiovascular diseases, which continue to be a major cause of morbidity and premature death in the world. CVDs accounted for 11% of all fatalities in Nigeria in 2018 (WHO, 2018). Men appear to have a higher mortality rate than women of the same age (Ezeugwunne et al., 2017), with coronary artery disease and stroke accounting for 80% of CVD fatalities in men and 75% of CVD fatalities in women (WHO, 2011). Atherosclerosis is linked to dyslipidemia, which raises the risk of cardiovascular disease (CVD). Numerous risk factors for CVDs can be categorized as modifiable or non-modifiable. Risk factors that can be changed include unhealthy eating habits, inactivity, drinking alcohol improperly, and smoking, which can lead to dyslipidemia, hypertension, high blood sugar, and other conditions, as well as overweight and obesity (WHO, 2018).These factors can be avoided with a balanced diet, regular exercise, and a well-balanced lifestyle. Several research (Oguoma et al., 2015; Ezeugwunne et al., 2017; González-Rivas et al., 2018; Vizentin et al., 2019; Nnamudi et al., 2020) have found varied levels of abnormalities in lipid levels (dyslipidemia) in apparently healthy persons. In a study of a Nigerian adult population, Oguoma et al. discovered a prevalence of low HDL (17.8%), hypertriglyceridemia (23.2%), hypercholesterolemia (38.1%), and central obesity (52.2%) (Oguoma et al., 2015). Also, a study examining the frequency and pattern of dyslipidemia in Nigeria discovered that dyslipidemia was common in all of Nigeria's geographic zones. Overall 60 percent of the apparently healthy Nigerians had dyslipidemia, while 89 percent of diabetic Nigerians had dyslipidemia (Oguejiofor et al., 2012). Furthermore, Olamoyegun and colleagues discovered elevated TC, high LDL-C, elevated TG, and low HDL-C in 5.3 percent, 19.3 percent, 4.4 percent, and 76.3 percent of their semi-urban inhabitants in Nigeria (Olamoyegun et al., 2016). Furthermore, varying prevalence of prediabetes and prehypertension has also been recorded in the current area among the study population (Obiora et al., 2017; Oponi et al., 2017). In light of the foregoing, it is critical to address the issue of dyslipidemia and, by extension, cardiovascular disease by involving the population at risk in a well-designed study that will raise awareness of the risk factors for dyslipidemia and its associated diseases and provide guidance to health policymakers, laboratory scientists, and clinicians.
Study design
This cross-sectional study determined the prevalence of dyslipidemia among Undergraduate University students at Nnamdi Azikiwe University, Nnewi Campus.
Sample size
Using the procedure outlined by Charan and Biswas, the sample size was estimated (2013);
N = (Z2pq)
d2
Where:
N= Desired number of sample when population of the facility is limited
Z = The standard normal variance where confidence level is 1.96 at 95%
p = prevalence rate of dyslipidemia in Nigeria is 85.9% (Fatou et al., 2016)
q = 1 – p
d = 5% i.e degree of precision as desired by the researcher.
Applying the method,
N = Z2 x P x (1-P)
D2
N = 1.962 x 0.859x (1-0.859)
0.052
N = 186±10%
Participants’ Recruitment
200 college students, both male and female, between the ages of 18 and 30, who appeared to be in good health, were enrolled in the study.
Inclusion criteria
The study included undergraduates between the ages of 18 and 30 from the Faculty of Basic Medical Sciences, Faculty of Health Sciences and Technology, and Faculty of Medicine at Nnamdi Azikiwe University, Nnewi campus.
Exclusion criteria
This study excluded smokers, alcoholics, and individuals with pre-existing diseases (diabetes, hypertension, and heart disease).
Ethical consideration
The faculty of Health Science and Technology's ethics committee approved the study before it began (NAU/FHST/2021/MLS77). Also, prior to the start of the study, the participants were asked to give their written informed consent.
Collection Of Samples
Five milliliters (5ml) of venous fasting blood was aseptically taken from each person after a 10- to 12-hour fast through the antecubital vein using a plastic syringe that had little to no stasis and placed in a plain container. Before being centrifuged for five minutes at a speed of 1000 rpm, the blood sample was given time to clot and retracted. The sera were then separated into plain tubes for lipid profile estimation and the samples that wouldn't be evaluated immediately were frozen at -8ºC.
Laboratory Methods
According to Allain et al. (1974), Fossati et al. (1982), and Burstein et al. (1980), TC, TG, and HDL-C levels were measured using enzymatic techniques, while LDL-C was estimated using the formula provided by Assmann et al. (1984). Fasting total cholesterol >5.2 mmol/l, fasting TG >1.7 mmol/l, LDL ≥3.5 mmol/L, and HDL <0>Anthropometrics indices and Blood pressure reading
Body mass index (BMI) was computed using the following formula: BMI= weight (Kg) / height (m2). Weight was measured using an automatic weighing scale, and height was measured using a measuring tape fastened to a piece of wood. Body mass index (BMI) values ≥25 and above 30 kg/m2 were used to characterize overweight and generalized obesity, respectively.
Study design
This cross-sectional study determined the prevalence of dyslipidemia among Undergraduate University students at Nnamdi Azikiwe University, Nnewi Campus.
Sample size
Using the procedure outlined by Charan and Biswas, the sample size was estimated (2013);
N = (Z2pq)
d2
Where:
N= Desired number of sample when population of the facility is limited
Z = The standard normal variance where confidence level is 1.96 at 95%
p = prevalence rate of dyslipidemia in Nigeria is 85.9% (Fatou et al., 2016)
q = 1 – p
d = 5% i.e degree of precision as desired by the researcher.
Applying the method,
N = Z2 x P x (1-P)
D2
N = 1.962 x 0.859x (1-0.859)
0.052
N = 186±10%
Participants’ Recruitment
200 college students, both male and female, between the ages of 18 and 30, who appeared to be in good health, were enrolled in the study.
Inclusion criteria
The study included undergraduates between the ages of 18 and 30 from the Faculty of Basic Medical Sciences, Faculty of Health Sciences and Technology, and Faculty of Medicine at Nnamdi Azikiwe University, Nnewi campus.
Exclusion criteria
This study excluded smokers, alcoholics, and individuals with pre-existing diseases (diabetes, hypertension, and heart disease).
Ethical consideration
The faculty of Health Science and Technology's ethics committee approved the study before it began (NAU/FHST/2021/MLS77). Also, prior to the start of the study, the participants were asked to give their written informed consent.
Collection Of Samples
Five milliliters (5ml) of venous fasting blood was aseptically taken from each person after a 10- to 12-hour fast through the antecubital vein using a plastic syringe that had little to no stasis and placed in a plain container. Before being centrifuged for five minutes at a speed of 1000 rpm, the blood sample was given time to clot and retracted. The sera were then separated into plain tubes for lipid profile estimation and the samples that wouldn't be evaluated immediately were frozen at -8ºC.
Laboratory Methods
According to Allain et al. (1974), Fossati et al. (1982), and Burstein et al. (1980), TC, TG, and HDL-C levels were measured using enzymatic techniques, while LDL-C was estimated using the formula provided by Assmann et al. (1984). Fasting total cholesterol >5.2 mmol/l, fasting TG >1.7 mmol/l, LDL ≥3.5 mmol/L, and HDL <0>Anthropometrics indices and Blood pressure reading
Body mass index (BMI) was computed using the following formula: BMI= weight (Kg) / height (m2). Weight was measured using an automatic weighing scale, and height was measured using a measuring tape fastened to a piece of wood. Body mass index (BMI) values ≥25 and above 30 kg/m2 were used to characterize overweight and generalized obesity, respectively.
The Statistical Package for the Social Sciences (SPSS) version 23.0 was used to analyze the results. The paired student t-test and Pearson correlation were used to statistically analyze the data, which was presented as mean±SD, with level of significance assumed at p<0>
The anthropometric indices of the study subjects are shown in TABLE 1.
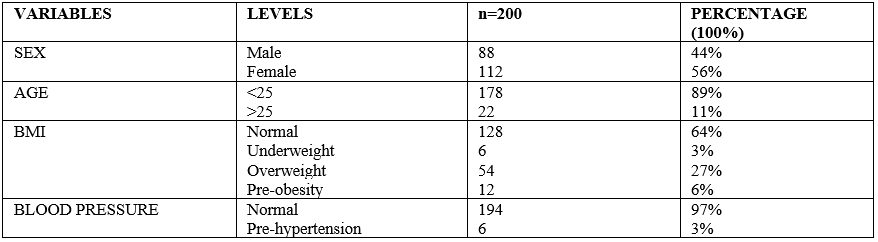
Table 1: Anthropometric Indices of the Students Studied
The study involved 200 students (88 men and 112 females) between the ages of 18 and 30. Female students accounted for 56 percent of the total, while male students accounted for 44 percent. 89 percent of the students who took part were under the age of 25, while 11 percent were beyond the age of 25. Students with a normal BMI, underweight, overweight, pre-obese, normal blood pressure, and pre-hypertensive blood pressure account for 64 percent, 3 percent, 27 percent, 6 percent, 97 percent, and 3 percent of the population, respectively.
Male systolic blood pressure (119.05 ± 9.73), female systolic blood pressure (116.82 ± 9.09), male diastolic blood pressure (70.59 ± 8.03), female diastolic blood pressure (69.33 ± 9.99), male body mass index (22.86 ± 3.96) and female body mass index (23.48 ± 3.84) had no sex differences (P>0.05). Male height (1.77 ± 0.08) and male weight (72.64 ± 11.07) had significantly higher mean ± SDs than female height (1.68 ± 0.08) and female weight (66.40 ± 10.32), respectively (p<0>
*Statistically significant at p<0>
Table 2: Blood Pressure and Anthropometric Parameters in participants studied Grouped by Sex (Mean±SD)
There were no sex differences in the mean and standard deviation of male high density lipoprotein cholesterol (1.21± 0.27) compared to female high density lipoprotein cholesterol (1.22 ± 0.23) (P>0.05). Male total cholesterol (4.56 ± 0.66) and male low density lipoprotein cholesterol (2.75 ± 0.62) mean ± SD were significantly lower than female total cholesterol (4.86 ± 0.84) and female low density lipoprotein cholesterol (3.08 ± 0.83), respectively (p<0>

*Statistically significant at p<0>
Table 3: Lipid profile levels in participants studied based on Sex (mean±SD)
*Statistically significant at p<0>
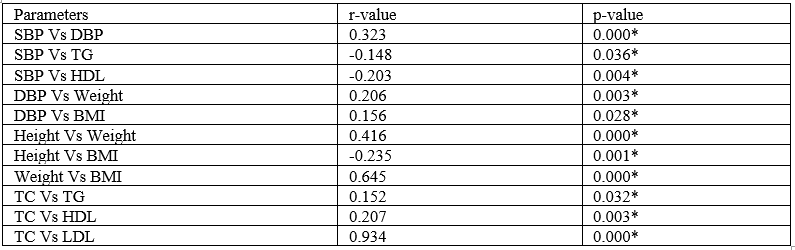
Table 4: Association between Parameters of the Studied Participants
Significant positive correlations were found between SBP and DBP (r= 0.323; p= 0.000), DBP and weight (r= 0.206; p=0.003), DBP and BMI (r= 0.156; p=0.028), height and weight (r=0.416; p=0.000), weight and BMI (r= 0.645; p=0.000), TC and TG (r=0.152; p=0.032), TC and HDL (r=r=0.207; p=0.003), TC and LDL (r=0.934, p=0.000) while SBP Vs TG (r=-0.148; p=0.036), SBP Vs HDL (r=-0.203; p=0.004), and Height Vs BMI (r=-0.235; p=0.001) all had statistically significant negative relationships.

*Statistically significant at p<0>
Table 5: Association between Parameters Studied in the Male Participants
The study parameters showed significant positive correlations between SBP and DBP (r=0.277; p=0.009), SBP and BMI (r=0.212; p=0.048), Height and Weight (r=0.464; p=0.000), Weight and BMI (r=0.537; p=0.000), TC and TG (r=0.280; p=0.008), TC and HDL (r=0.266; p=0.012), TC and LDL (r=0.881; p=0.000), while SBP and TG had a strong negative correlation (r=-0.276; p=0.009).
*Statistically significant at p<0>
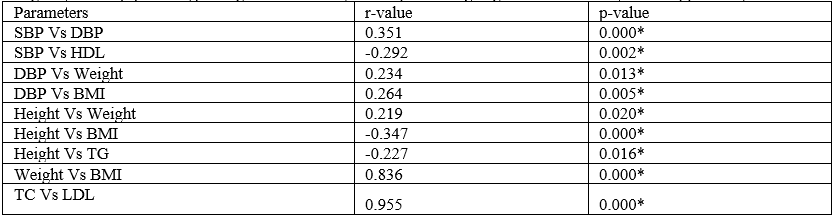
Table 6: Association between Parameters Studied in the Female Participants.
Significant positive associations were found in the study parameters between SBP and DBP (0.351; p=0.000), DBP and BMI (0.264; p=0.005), Height and Weight (0.219; p=0.020), Weight and BMI (0.836; p=0.000), TC and LDL (0.955; p=0.000), and DBP and Weight (0.234; 0.013).
Also, significant negative correlations were seen between SBP and HDL (r= -0.292; p=0.002), height and BMI (r= -0.347; p=0.000), and height and TG (r= -0.227; p=0.016), but not with the other parameters (p>0.05).

Table 7: Prevalence of Dyslipidemia Among Studied Group
Hypercholesterolemia, hypertriglyceridemia, low HDL-C, and high LDL-C were found to be prevalent in 26.5 percent, 4 percent, 12.5 percent, and 16.5 percent of the population, respectively.
Dyslipidemia is a global epidemic that is a major cause of cardiovascular disease.
Dyslipidemia was quite prevalent among the individuals in this study (39.5 percent). This increase in dyslipidemia prevalence could be due to changes in eating habits, decreased physical activity, and work intensity. The current result is higher than previous findings in Eastern Ethiopia (34.8%; Sufa et al., 2019), Africa (25.5%; Noubiap et al., 2018), China (32.2%; Liu et al., 2018); and Iran (30.0%; Najafipour et al., 2016). However, the prevalence recorded in the present study is lower compared to previous studies reported in Lithuania (89.7%; Rinkūnienė et al., 2015), South Africa (85.0%) (Dave et al., 2016), India (78.4%) (Banerjee et al., 2014), Poland (77.2%) (Pająk et al., 2016), India (50.7%) (Wankhade et al., 2018), Uganda (63.3%) (Bakesiima et al., 2018), Palestine (66.4%) (Ali et al., 2019) and South Africa (67.3%) (Reiger et al., 2017). This disparity could be attributed to differences in cutoffs applied in the different studies.
Elevated LDL-C (16.5%) and high total cholesterol (26.5%) were the two most common components of dyslipidemia, which is consistent with earlier findings in Nigeria reported by Okaka and Eiya (Okaka and Eiya, 2013) and Oguoma et al. (Oguoma et al., 2015). (Okaka and Eiya, 2013). The increasing consumption of simple carbohydrates and saturated fat in modern diets may be the cause of this phenomenon.
The prevalence of high total cholesterol (26.5%) in this study is lower than that in the prior study published in Ethiopia (33.7%) and Iran (29.6%) (Sufa et al., 2019), but is higher than the study results in Ethiopia (5.2%) (Gebreyes et al., 2018), Northern Ghana (4.02%) (Agongo et al., 2018), South Western Uganda (6%) (Asiki et al., 2015), South East Nigeria (8%; 11.4%) (Okwara et al., 2021; Anyabolu, 2017) and South East costal region in China (8.4%) (Lin et al., 2019).
The prevalence of high LDL-C (16.5%) in this study is higher than the previous finding reported in Ethiopia (14.1%) (Gebreyes et al., 2018), Northern Ghana (5.55%) (Agongo et al., 2018) and in South East costal region in China (13.9%) (Lin et al., 2019). But lower than the findings reported in Thailand (56.5%) (Narindrarangkura et al., 2019), Uganda (60.9%) (Lumu et al., 2017), Ghana (61.0%) (Micah and Nkum, 2012), Senegal (66.3%) (Doupa et al., 2014), Jordan (75.9%) (Abujbara et al., 2018), and India (47.8%) (Banerjee et al., 2014)
The current study's prevalence of low HDL-C (12.5%) is somewhat comparable to earlier studies conducted in various African nations, notably Malawi (15.9%) (Amberbir et al., 2018), Ghana (17.0%) (Micah and Nkum, 2012), and Africa (18.5%) (Micah and Nkum, 2012), unlike many prior studies in the South East costal region of China (23.1%) (Lin et al., 2019), South East Nigeria (34.4%) (Anyabolu, 2017), Northern Ghana (60.30%) (Agongo et al., 2018), Ethiopia (68.7%) (Gebreyes et al., 2018), and South Western Uganda (71.3%) (Asiki et al., 2015).
The prevalence of high triglycerides (4%) in this study is higher than the results from Northern Ghana reported before (2.12%) (Agongo et al., 2018), but lower than those reported in Thailand (49.9%) (Narindrarangkura et al., 2019), South Africa (59.3%) (Reiger et al., 2017), Brazil (65.3%) (Feitosa et al., 2017), Senegal (7.1%) (Doupa et al., 2014), Ethiopia (21.0%) (Gebreyes et al., 2018), Malawi (28.7%) (Amberbir et al., 2018), Venezuela (39.7%) (González-Rivas et al., 2018), Jordan (41.9%) (Abujbara et al., 2018), and Uganda (42.1%) (Lumu et al., 2017).
Males (28.4%) had a lower prevalence of dyslipidemia in this study than females (48.2%), which was 39.5 percent. There were no sex differences in the mean and standard deviation of male high density lipoprotein cholesterol (1.21±0.27) compared to female high density lipoprotein cholesterol (1.22±0.23). Male total cholesterol (4.56 0.66) and male low density lipoprotein cholesterol (2.75±0.62) had mean and standard deviations that were significantly lower than those of female total cholesterol (4.86±0.84) and female low density lipoprotein cholesterol (3.08±0.83), respectively (P 0.05). Additionally, the mean and standard deviation of the male triglycerides (1.34±0.34 Vs 1.24 ±0.20) were significantly higher (P <0>
Significant positive correlations were found between SBP and DBP, DBP and weight, DBP and BMI, height and weight, weight and BMI, TC and TG, TC and HDL, TC and LDL while SBP and TG, SBP and HDL as well as Height and BMI all had statistically significant negative relationships.
Although the prevalence of dyslipidemia among the undergraduate students studied was not as high as that reported in Lithuania, South Africa, India, Poland, Uganda, Palestine, and South Africa, it was higher than that reported in Ethiopia, Africa, China, and Iran. The most common kind of dyslipidemia was high total cholesterol, followed by raised LDL-C. Lifestyle and diet appear to be driving a rise in prevalence, particularly among women. Among other interventions, population-wide awareness, specialized education on increased cholesterols and related dangers should be encouraged.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
