
Research Article | DOI: https://doi.org/10.31579/2642-9756/175
1 Department of obstetrics and Gynecology, El Sahel Teaching Hospital, Egypt.
2 Lecturer of obstetrics & gynecology department, Suez University, MD, Egypt.
*Corresponding Author: Hany Mahmoud, Department of obstetrics and Gynecology, El Sahel Teaching Hospital, MD, fellow of obstetrics and gynecology, Egypt.
Citation: Hany Mahmoud Abd Elhamied, and Ahmed Mohamed Sewidan, (2022), Evaluation of Cholecalciferol Interaction with Pain Signaling after Laparoscopic Ablation of Endometriotic Lesions in Women with Hypovitaminosis D, J. Women Health Care and Issues. 5(4); DOI:10.31579/2642-9756/175
Copyright: © 2022, Hany Mahmoud. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 May 2022 | Accepted: 10 June 2022 | Published: 21 June 2022
Keywords: chronic pelvic pain; endometriosis; laparoscopy; cholecalciferol; hypovitaminosis D
Aim: The study's goals were to ascertain the subjective cure rate and the safety of giving cholecalciferol to women with hypovitaminosis D after ablative operations to relieve pain associated with endometriosis.
Patients and Methods: We enrolled participants in this double-blind clinical trial who had endometriosis diagnosed and treated by laparoscopy and who had at least three dysmenorrhea and/or pelvic pain scores at eight weeks following surgical therapy. They were given either a placebo or vitamin D (50 000 IU each week for 12 weeks). At 6 months following surgical therapy, the VAS test was used to assess the pain intensity between the two groups (placebo and treatment).
Results: Twenty patients were in the vitamin D group and twenty were in the control group. Both groups shared common traits that were analogous. After administering vitamin D or a placebo, there were no discernible differences between the two groups in the severity of the dysmenorrhea and pelvic pain scores (p>0.05). Mean pelvic discomfort at six months following laparoscopy was 3.2 ±1.6 in the vitamin D group and 3.7 ±1.1 in the placebo group (p>0.05). Mean dysmenorrhea score in the vitamin D group was 3.4±1.2, while it was 3.1±1.8 in the placebo group. The mean pain scores in the two groups did not differ significantly from one another (p>0.05).
Conclusion: Treatment with vitamin D did not significantly reduce dysmenorrhea or pelvic discomfort after ablative surgery for endometriosis.
The International Association for the Study of Pain has recently offered the following definition of pain: "An adverse sensory and emotional experience typically caused by, or resembling that caused by, actual or potential tissue injury." The body's alarm system, pain serves as a warning of impending danger. Since over 20% of those who have chronic pain experience no relief, the currently available analgesics have been regarded to be grossly insufficient for treating this complex disease. This is believed to be because chronic pain is complicated and changeable, and the underlying mechanisms are still unclear [1].
A prevalent gynecologic condition called endometriosis affects 10% of all women who are in the reproductive stage of their lives [2]. It is believed that the condition is caused by endometrial tissue growing outside of the cavum uteri and causes a long-lasting inflammatory response. Endometriosis resembles malignant diseases in a number of ways, including decreased apoptosis, invasion of neighbouring organs (the bowel and bladder), increased angiogenesis, recurrence, and the requirement for multiple surgical procedures [3].
1,25(OH)2 D3, the active form of vitamin D, is a lipophilic steroid hormone. Food can contain cholecalciferol (vitamin D3), but the skin is the main place where it is found because sunlight exposure transforms the precursor 7-dehydrocholesterol into vitamin D3 [4]. Vitamin D status and the risk of myasthenia gravis, endometriosis, breast and ovarian cancer, as well as increased arterial stiffness in older patients, may be related. Vitamin D has been discovered to play a part in the normal regulation of cellular growth. In chronic inflammatory responses, vitamin D has immune-regulatory effects. Vitamin D boosts the production of anti-inflammatory cytokines while lowering the production of pro-inflammatory cytokines [5].
There hasn't been a published randomised clinical trial on endometriosis and vitamin D treatment in women, despite the fact that numerous studies have found an indirect link between vitamin D and endometriosis. In a double-blind, randomised clinical trial, we investigated the association between vitamin D and endometriosis by examining the impact of vitamin D supplementation on pain relief in endometriosis patients who had undergone successful laparoscopic diagnosis and treatment.
From January 2017 to December 2019, this randomised, double-blind clinical trial was conducted in a single tertiary hospital. There were 40 patients in total with proven vitamin D deficiency (serum 25-OHD3 level 18 ng/ml).
Laparoscopy was used for a variety of symptoms, including ovarian cysts, infertility, pelvic pain, and dysmenorrhea, in order to identify patients with endometriosis.
A thorough medical history was taken once more the day before the procedure, and pain and dysmenorrhea were evaluated using VAS scoring, where a score of 0 indicates no pain and a score of 10 indicates the worst pain.
Endometriosis was identified during laparoscopy by attempting to remove or destroy all diseased tissue.
The VAS test was conducted once more on patients who had endometriosis in the second menstrual cycle following laparoscopic diagnosis and treatment.
Age 15 to 40 years, confirmed endometriosis cases by laparoscopy, and low serum vitamin D levels (18 ng/ml) are the inclusion criteria.
Exclusion criteria:
Following approval by the hospital ethics committee, eligible patients were randomly assigned to receive vitamin D or a placebo using a simple randomization process. For six months, we gave the vitamin D group (D group) 50 000 iu of oral vitamin D on a weekly basis, while we gave the placebo group (P group) one placebo capsule on a weekly basis. The VAS test was conducted twice for each group.
Analysis using statistics: The investigative report contains the retrieved data. SPSS® for Windows®, version 15.0 (SPSS, Inc., USA), was used to analyse the data.
In table 1, the mean age of participants in groups I and II was 25.3 ±7.2 and 25.4 ± 6.9 respectively. Dysmenorrhea in all cases, ovarian cysts (n=6 in group I and 5 in group II), chronic pelvic pain (n=18 in group I and 19 in group II), and infertility (n=10 in group I and 11 in group II) were the main reasons why women with endometriosis diagnosed by laparoscopy underwent the procedure. More than one factor led to the need for laparoscopy in some patients. Endometriosis severity was essentially comparable between the two groups (P>0.05).
The mean pelvic pain score prior to laparoscopy was 6.1 ±1.2 in the vitamin D group and 6.7 ±1.3 (P > 0.05) in the placebo group. The mean dysmenorrhea pain score before laparoscopy was 6±2.1 in the vitamin D group and 6.4 ±1.9 in the placebo group (p>0.05). A comparison of the two groups' levels of dysmenorrhea and/or pelvic pain prior to laparoscopy, during the second menstrual cycle following laparoscopy, and six months later.
There was no discernible difference between the two groups' mean pain scores at the second menstrual cycle following laparoscopy (p>0.05) or at six months (p>0.05) for dysmenorrhea or pelvic pain, respectively.
Mean pelvic pain at 6 months after laparoscopy in the vitamin D group was 3.2 ±1.6 and in placebo group it was 3.7±1.1 (p>0.05). Mean dysmenorrhea was 3.4±1.2 in the vitamin D group and 3.1±1.8 in the placebo group (p>0.05).
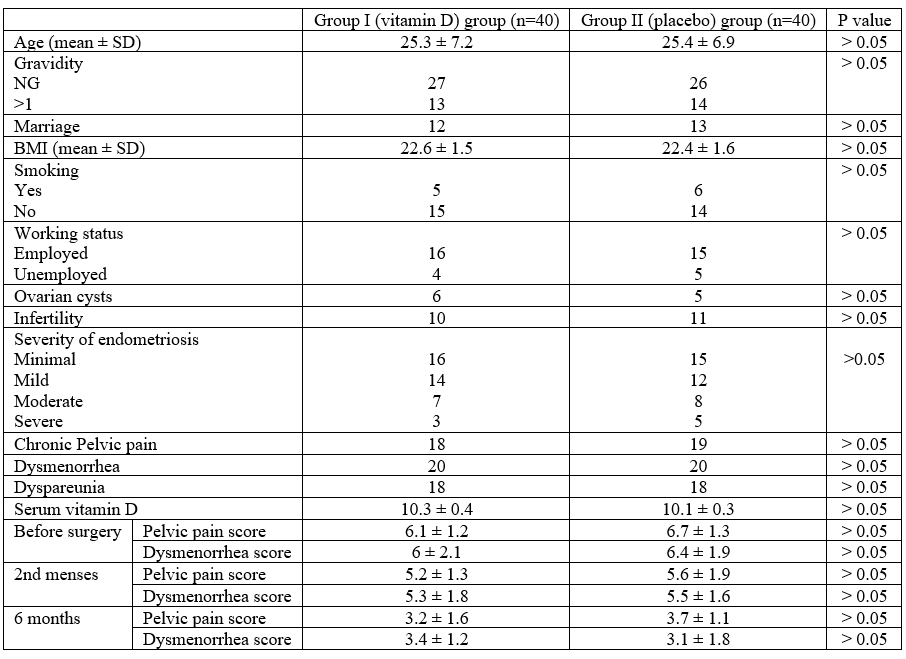
Table 1: Comparing the baseline characteristics and pain scores prior to and following laparoscopy between group I (vitamin D group) and group II (placebo group)
The frequency of vitamin D insufficiency is considerable worldwide. Reports state that it affects 52% of Black and Hispanic teens in Boston and 48% of girls in Maine. Furthermore, 40–100% of senior men and women in the US and Europe are affected [6]. Vitamin D insufficiency was found in 57% of people between the ages of 18 and 79, according to German research [7]. Ninety percent of healthy people in Delhi, India were found to be vitamin D deficient [8]. 37.3% of the 195 studies from 44 countries included in the systematic analysis had mean blood vitamin D levels less than 20 ng/ml [6]. Turkish women who were expecting had a high incidence rate of 81.4% [9].
The mean blood vitamin D level among high school students in Iran was found to be 14.7±9.4 ng/ml [10]. 51.2% of female university students in Shiraz, Iran, were found to have low blood levels of vitamin D in another research [11]. Following surgical endometriosis excision, a double-blind, randomised clinical trial examined the intensity of pelvic discomfort and/or dysmenorrhea. After six months, there was no discernible difference between the effects of vitamin D3 (cholecalciferol) and a placebo [12].
There was no statistically significant difference between 132 infertile women with endometriosis and 132 fertile women in a study looking into the relationship between vitamin D receptor gene polymorphism and endometriosis [12]. This suggests that the gene polymorphism has no significant effect on the pathophysiology of endometriosis. According to some researches, consuming more dairy products and 1,25-dihydroxyvitamin D3 may reduce the incidence of endometriosis [13, 14]. Additionally, research comparing women with and without endometriosis led to the conclusion that endometriosis is associated with increased blood levels of vitamin D [15].
On the other hand, different research discovered that endometriotic women ingested far less omega-3 fatty acids and vegetables than non-endometriotic women [16]. A plasma glycoprotein called vitamin D binding protein (DBP) is involved in immunological and inflammatory response regulation, bone development, and the transportation of vitamin D metabolites [17]. The ectopic endometrial tissues had a much greater level of vitamin D binding protein than the normal endometrial tissues, according to research [18]. Higher blood levels of vitamin D binding protein were found in endometriosis-affected women [19], according to a comprehensive evaluation of investigations done between 1946 and 2013.
Women with endometriosis exhibited greater serum DBP levels than women with other benign gynaecological disorders, according to different research comparing peritoneal and serum levels [20]. Furthermore, research comparing levels in endometriosis-positive and -negative women revealed that patients with endometriosis had noticeably higher urine DBP levels [21]. Vitamin D3 therapy was found to cause fibrosis and apoptosis in the stroma of endometriosis-affected tissues in a rat model [28]. Female Balb mice with endometriosis were given the vitamin D receptor agonist elocalcitol, which reduced their symptoms [22].
Research revealed that women who attended an infertility clinic frequently had low serum vitamin D3 levels, and that there was a significant correlation between these levels and height as well as a history of endometriosis [23]. It has been shown that vitamin D3 inhibits the growth, invasion, and generation of pro-inflammatory cytokines in endometriosis. This results in a decrease in the generation of interleukin 6 and other inflammatory cytokines that encourage the adherence of endometrial cells to the peritoneal cavity [24].
Furthermore, vitamin D3 dramatically reduced inflammatory responses, as well as the number of endometrial stromal cells and DNA synthesis, according to research on human endometriosis stromal cells [24].
Additionally, compared to healthy controls and patients with moderate endometriosis, the study revealed that patients with severe endometriosis had considerably lower blood vitamin D3 levels [25]. In Italian research on primary dysmenorrhea, forty women, aged 18 to 40, who had gone through four painful periods in a row during the preceding six months were assessed. High-performance liquid chromatography was used to measure the amounts of 25-hydroxy vitamin D in serum. Next, two groups of women were formed, and one group was given a single oral dosage of 300,000 units of vitamin D [26]. In Italy, a large percentage of healthy premenopausal women have low blood vitamin D levels.
There may be a link between the onset of endometriosis and vitamin D, even though our research revealed that vitamin D was useless in relieving pain associated with endometriosis.
Given the high frequency of vitamin D insufficiency in our country and throughout the world, it is possible that a sizable fraction of the research population was deficient, which might have an effect on our findings. Another drawback of our study is its tiny sample size. More clinical trials are necessary to better understand the significance of vitamin D medication for endometriosis-related pain. Subsequent research endeavours ought to evaluate the blood vitamin D levels of subjects before their enrolment and exclude those with insufficient levels. Larger sample sizes in clinical studies can yield more trustworthy results.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
