
Research Article | DOI: https://doi.org/10.31579/2690-8816/107
1 Department of Medical Laboratory Sciences.
2 Department of Chemistry Rivers State University, Port Harcourt, Nigeria.
*Corresponding Author: Oladapo-Akinfolarin T. T, Department of Medical Laboratory Sciences.
Citation: Oladapo-Akinfolarin, T. T, Bartimaeus, E.S and Akinfolarin, O.M. (2022). Human Chromosomal Q-heterochromatin Regions as a System. Biomedical Research and Clinical Reviews. 6(4); DOI: 10.31579/2690-8816/107
Copyright: © 2022 Oladapo-Akinfolarin, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 February 2022 | Accepted: 03 March 2022 | Published: 11 March 2022
Keywords: pregnancy; lipoprotein; apolipoproteins; uric acid; C-reactive protein
Pregnancy is associated with series of biochemical changes such as changes in cardiovascular markers. These changes may contribute to risk of developing cardiovascular disease among this group of people. Therefore, this work was aimed at evaluating changes in cardiovascular biochemical markers in pregnancy. This research was a cross-sectional study with 150 female subjects divided into three groups; control (non-pregnant women), 2nd trimester and 3rd trimester. Each of the group had 50 subjects each. Subjects were selected randomly from Rivers State University and Rivers State University Teaching Hospital. Fasting blood was collected using venipuncture technique (WHO, 2010). The collected blood was carefully dispensed into plain vacutainer tubes and assayed for uric acid, Apo A1 and B, CRP, TG, HDL and TC while VLDL and LDL were calculated. The data obtained from the study were analyzed using GraphPad Prism Version 8.0.2.263. ANOVA results revealed that there were significant differences in TC, TG, LDL, HDL, VLDL, CRP, ApoA1, and ApoB levels among non-pregnant, 2nd trimester and 3rd trimester groups of normotensive pregnant women (P<0.05) except for uric acid (UA) that showed no significant difference. Post hoc analysis revealed significant difference in studied parameters between groups except in HDL, TG and VLDL in non-pregnant and 2nd trimester group while UA remained non-significant between compared groups. This study has shown that pregnancy causes significant changes in cardiovascular risk markers in healthy pregnant women.
Cardiovascular disease such as atherosclerosis remains the leading cause of mortality and morbidity in Western countries. Atherosclerosis which is a disease of large arteries (Hussain et al., 2013), results from the interaction between genetic and environmental factors modulating the functions of various cell types and inflammatory molecules within the arterial wall (Dashti et al., 2011). The major risk factor of this disease is hyperlipidaemia, which can arise due to either overproduction of lipoproteins and/or their reduced clearance from the plasma. Plasma lipoproteins are responsible for the transport and delivery of lipids throughout the body. The primary function of plasma lipoproteins is to deliver hydrophobic lipids such as triglycerides and cholesterol to peripheral tissues for storage as sources of energy and substrates for steroidal hormone synthesis (Farkas-Epperson and Le, 2012). The liver and the intestine are the two major organs that assemble lipoproteins. The liver synthesizes VLDLs (mainly apoB100- containing lipoproteins in humans) to transport endogenous fat to peripheral tissues. These particles are catabolised in the circulation, thereby producing a generation of plasma LDL: It is known that LDL cholesterol is atherogenic, therefore, it is assumed that hepatic lipoproteins are the main and only contributors to atherosclerosis (Hussain et al., 2013). ApoB100 is independently associated with ischaemic heart disease and identifies high-risk phenotypes in normocholesterolaemic diabetic patients. This could be used to evaluate the lipidaemic pattern of these patients (American Diabetes Association (ADA), 2010).
C-reactive protein (CRP) is an acute phase reactant synthesized in the liver in response to the cytokine interleukin-6 (Casas et al., 2008). It has been anticipated that even cells of the smooth muscles present in the human coronary arteries can also produce C-reactive protein in response to cytokines that have inflammatory actions (Liu et al., 2013). According to a study, CRP plays an active role in atherosclerosis in addition to being a marker for vascular inflammation. This is a factor responsible for the progression of atherosclerotic plaque.
Human pregnancy also known as gestation or gravidity is a period when a woman has one or more progenies in her womb. It is typically separated into three trimesters based on gestational age which is measured in weeks and months. The first trimester is from conception to 12 weeks (2 months and 3 weeks). The second trimester is from 13-27 weeks, (3 months to 6 months and 2 weeks); while the third trimester starts about. 28weeks and lasts until birth (7 months to 9 months) (Huda et al., 2009).
According to Global Burden of Disease (2014), deaths resulting from complications of pregnancy reduced from 377,000 in 1990 to 293,000 in 2013, and the general causes include arterial blood pressure of pregnancy, maternal bleeding, complications of abortion, obstructed labour and maternal sepsis.
Pregnancy is characterized by changes in maternal metabolism and body composition in order to provide sufficient energy and nutrients to the developing fetus and later for lactation. There are marked increases in plasma lipid concentrations as gestation advances, with plasma cholesterol and triglyceride concentrations rising typically by 25-50% and 20-40% respectively. Therefore, this study is focused on evaluating changes in cardiovascular markers in normotensive pregnant women.
Study Design
This research was a cross-sectional study with 150 female participants recruited from Rivers State University Teaching Hospital, Port Harcourt and the Rivers State University, in Rivers State, Nigeria. The participants were grouped into three major groups: control (non-pregnant women), 2nd trimester and 3rd trimester. Each of the group had 50 subjects.
Study Location
This study was carried out jointly in the Rivers State University and the Rivers State University Teaching Hospital (formerly called Braithwaite Memorial Specialist Hospital) in Port Harcourt, the capital city of Rivers State in Nigeria. Port Harcourt is a cosmopolitan city with a population of about two million residents.
Eligibility Criteria
Inclusion criteria
All apparently healthy pregnant women attending antenatal care were eligible for inclusion in this study, except the control subjects. Other inclusion criteria are no history of surgery and blood transfusions, not diagnosed diabetic and subjects gave written consent after counseling.
Exclusion Criteria
These included those who were apparently ill or with known history of any of the infectious diseases, underlying chronic illness for example; gastric and intestinal illness, history of prenatal bleeding, malignancy, tuberculosis, diagnosed diabetes, and cardiovascular disease. A history of blood transfusion, surgery or an inability to provide informed consent was also noted for exclusion.
Ethical Consideration and Informed Consent
Ethical clearance for the study was obtained from the Ethics Committee of Rivers State Ministry of Health, Port Harcourt, Nigeria and upon the study approval, the work was conducted.
Subject Selection
Subjects were selected randomly from Rivers State University and Rivers State University Teaching Hospital, having ensured that they met the criteria on the questionnaire that made them suitable for inclusion and exclusion.
Sample Collection Method
Subjects were selected using simple random method as described by Fyneface et al., (2018) and Fyneface et al., (2020). Blood was collected using venipuncture technique. The collected blood was carefully dispensed into plain vacutainer tubes, left to clot and centrifuged at 1500rpm for 10 minutes. Serum was separated and stored at -4oC until it was assayed for CRP, apoA1, apo B, uric acid, total cholesterol, triglycerides and high density lipoprotein cholesterol, while the values of LDL and VLDL were calculated (Friedewald et al.,1972).
Biochemical Determinations
Fasting blood samples were used for the biochemical investigations for uric acid, Apo A1 and B, CRP, TG, HDL and total Cholesterol. All biochemical analyses were carried out in the Department of Medical Laboratory Science, Rivers State University.
Determination of High Sensitive C-reactive Protein Concentration in Human Serum.
The method of Nazir & McQueen, 1993 was used.
Procedure
2µl of sample was added to the test tubes, and 5 other tubes for calibration. 250ul of R1 assay buffer (see composition in appendix) was added to all the tubes. It was mixed by tilting the bottom of the tubes and then incubated at 370C for 5 minutes and read as absorbance OD1. 50ul of R2 antibody reagent (see composition in appendix) was added to all the tubes. It was mixed by tilting the bottom of the tubes and then incubated at 370C for 3 minutes and read as absorbance OD2.
Determination of Apo Lipoprotein A1 in Human Serum
The method of Nazir and McQueen, 1993 was used.
Procedure
2µl of serum was placed in the test tubes and 5 other tubes for calibration. 250µl of buffer (R1) was added to all the tubes, mixed by tilting the bottom of the tubes, and allowed for 5 minutes at 37oC in a water bath. It was then read in a spectrophotometer at 340 nm. The absorbance was recorded as OD1. 50µL of the antibody reagent (R2) was added to the reaction and allowed for 5 minutes at 37oC in a water bath. It was then read at 340nm using the spectrophotometer. The absorbance was recorded as OD2. The absorbance was taken as [OD2– OD1] of standard and sample.
Determination of Apolipoprotein B in Human Serum
The method of Nazir and McQueen, 1993 was used.
Procedure
2µl of serum was placed in the test tubes and 5 other tubes for calibration. 250µl of buffer (R1) was added to all the tubes, mixed by tilting the end of the tubes and allowed for 5 minutes at 37oC in a water bath. It was then read in a spectrophotometer at 340 nm wavelength. The absorbance was recorded as OD1. 50 µl of the antibody reagent (R2) was added to the reaction and allowed for 5 minutes at 37oC in a water bath. It was then read at 340nm, using the spectrophotometer. The absorbance was recorded as OD2. The absorbance was taken as (OD2 – OD1) for samples and standard. A standard curve was plotted and the concentration of controls, standard and sample was read.
Determination of Total Cholesterol in Serum
The method of Allain et al., 1974 was used.
Procedure
The assay conditions were considered. The instrument was zeroed with distilled water. One ml of the cholesterol reagent was transferred by pipetting into clean dry test tubes labelled as blank, standard and tests and 10 µl of distilled water, standard and sample were added to their respective tubes. It was properly mixed, by tilting the bottom of the tubes and incubated in a waterbath at 37oC for 5 minutes. The absorbance of the standard and test samples was measured against the blank in a spectrophotometer at 540nm wavelength.
Determination of High-Density Lipoprotein (HDL) Cholesterol in Serum
The method of Tietz, 1987 was used.
Procedure
The blood samples were transferred into tubes and centrifuged for five minutes at 12,000rpm. The supernatant (sera) was separated and arranged according to the labelled tubes as control, standard and samples. 200µl of precipitating reagent (R) and 20µl of sample were transferred into the tubes for test, 20ul of standard for standard tube and distilled water for blank. It was mixed properly by tilting the bottom of the tubes and allowed to stand for 10 minutes at room temperature. The contents of the tubes were centrifuged for 2 minutes at 12,000rpm. Thereafter, the clear supernatant was separated and determined for HDL cholesterol.
Determination of Triglycerides in Serum
The method of Fraser & Hearne, (1981) was used.
Procedure
The assay conditions were considered. The instrument was zeroed with distilled water. 1ml of triglyceride reagent was added to the tubes as blank, standard and test. 10 µl of standard and sample were added to the tubes, mixed and incubated for 5 minutes at 37oC. The absorbance was read using 1cm light path (cuvette) for samples against blank at 505nm wavelength.
Determination of Low-Density Cholesterol (LDL-C)
The method of Friedwald et al., 1972 was used.
Calculation
LDL cholesterol values in the serum sample were calculated as a difference in the results of the total cholesterol, triglycerides and HDL.
LDL – Cholesterol = Total Cholesterol – (TG/2.2) – HDL
(3.8 - 4.9)mmol/l
Determination of Uric Acid in Serum
The enzymatic method of Barr (1990) was used.
Procedure
Tubes were arranged according to labels as blank, standard and test. 20µl of distilled water was added into the blank tube, 20µl of standard to standard tube and 20µl of serum to test tubes and properly mixed by tilting the bottom of the tubes. It was incubated for 5 minutes at 37oC. It was then read in a spectrophotometer at 520nm wavelength.
Quality Control
Two levels of normal and abnormal controls were used to verify the performance of the procedures for each batch of analysis. Other control measures followed were checking instrument settings, and light source, cleanliness of all equipment used, ensuring the water used was free of contaminants to avoid interferences, checking reaction temperature and checking expiry date of kit and contents.
Statistical Analysis
The data obtained from the study were analyzed using the GraphPad Prism Version 8.0.2.263. The data were expressed as mean and standard deviation. Comparison of the means was done using the one-way analysis of variance (ANOVA). The Turkey comparison test was used to verify significant differences between the groups at P<0>
Comparing cardiovascular markers in Normotensive Pregnant Women.
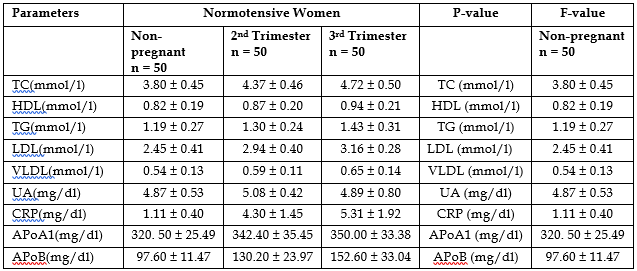
The results above showed that there were significant differences in TC, TG, LDL, HDL, VLDL, CRP, ApoA1, and ApoB levels among non-pregnant, 2nd trimester and 3rd trimester groups of normotensive pregnant women (P<0>
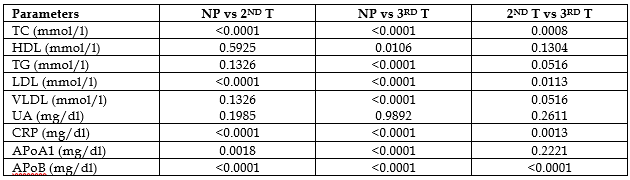
NP- Non-Pregnant, 2nd T – second Trimester, 3rd T- third trimester.
The above Post hoc analysis revealed significant difference in studied parameters between groups except in HDL, TG and VLDL in non-pregnant and 2nd trimester group while UA remained non-significant between compared groups.
The analysis of the mean values of the maternal characteristics of the Normotensive women in the 2nd and 3rd Trimester and comparing with Non-pregnant showed that there was a significant difference in TC, LDL, HDL, TG, VLDL, CRP, ApoA1, and Apo B at P < 0>et al, 2015; this difference in HDL and LDL, could suggest that, pregnancy as a stress test for the cardiovascular system may have simply revealed a pre-existent cardiovascular dysfunction rather than cause it, as obesity and dyslipidemia are shared between cardiovascular disease and pregnancy disorders (Wenger, 2014).
For TC, it has been determined several decades ago that the average total cholesterol level in the Nigerian population is 3.54±0.14mmol/L. In the present study, the serum total cholesterol levels obtained for the normotensive subjects were 3.80±0.45 mmol/L (non-pregnant women), 4.37±0.46mmol/L (2nd trimester pregnant women) and 4.72±0.50 mmol/L (3rd trimester pregnant women). Both trimesters in the normotensive subjects were significantly higher than the non-pregnant women. This implied that pregnancy induced the rise in TC level. The third trimester was also significantly higher than the second trimester, thereby pointing to the fact that the longer the duration of pregnancy, the higher the total level of cholesterol. Conversely, another study reported that pregnancy does not affect the concentration of TC and other lipid parameters (Oladapo-Akinfolarin, et al., 2018).
CRP is known to be slightly elevated during pregnancy, due to maternal inflammatory reaction to the pregnancy. However, Ernest et al. (2011) suggested that CRP of 2.5 mg/dl and above could be considered high for pregnant women. In this study, the level of CRP was significantly higher (P<0>et al., 2017). Elevated levels of CRP in pregnancy may be a marker for complications, but more studies are necessary to fully understand the role of CRP and pregnancy.
Previous studies showed that measures of unhealthy lifestyle habits such as cigarette smoking are also associated with the elevated CRP levels whereas moderate alcohol consumption and increased physical activity are associated with lower CRP levels (Fredrikson et al., 2004; Oliveira et al., 2010). Normal people with CRP levels greater than or equal to 2mg/dl likely need more intense management and treatment for heart disease. Elevated levels of CRP may have an important role in identifying those who might need closer follow-up or more intensive treatment after heart attacks or heart procedures. The CRP levels may also be useful in uncovering those at risk of heart disease where cholesterol levels alone may not be helpful.
The two lipoproteins investigated in this work were ApoA1 and Apo B. The Apo A1 levels for normotensive subjects were; non-pregnant 320.50±25.49 mg/dl, second trimester 342.40±35.45 mg/dl and third trimester 350.00±33.38 mg/dl. The results were far above the normal level of 225 mg/dl for all the three groups. This could indicate that the subjects are protected from CAD. Apo A1 is the major component of HDL and has been shown to predict short term and long term risk in patients with normal HDL according to May et al, 2013. The HDL values in this work were lower than normal, and could be as a result of change in HDL composition, but Apo A1, is the major protein component of HDL, which is largely responsible for reverse cholesterol transport. In essence, the functional-state of the HDL molecule is reflected by Apo A1. May et al, 2013 also stated that Apo A1 has a constant inverse relationship with CAD events, that is, an increase in Apo A1 will always lead to a decrease in CAD events.
The Apo B values in this work were within the normal range of 117 mg/dl for non-pregnant normotensives (97.60±11.47 mg/dl). However, the values for 2nd trimester (130.20±23.97 mg/dl) and 3rd trimester (152.60±33.04 mg/dl) were higher than the normal range. The Apo B concentration reflects the number of atherogenic particles (VLDL, IDL and LDL) according to American Diabetes Association (2010).
There is only one Apo B molecule for each VLDL-C and LDL-C particle and because VLDL-C particles are cleared much faster than are LDL-C, Apo B levels in essence reflect LDL-C number and high Apo B levels reflect a relative reduction in cholesterol level, resulting in small dense LDL-C particles derived from VLDL-C overproduction. These could be the reasons why the cholesterol values were in the normal range for 2nd and 3rd trimester, though LDL levels were unusually below the normal reference range of 4.9mmol/L.
This study has shown that changes in pregnancy period such as second and third trimesters have significant effect in cardiovascular markers. Thus, pregnancy could become a risk factor for cardiovascular disease among women especially when the changes in these biomarkers are not corrected after pregnancy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
