
Research Article | DOI: https://doi.org/10.31579/2643-6612/027
Rutgers School of Dental Medicine.
*Corresponding Author: Pamela L Alberto, Rutgers School of Dental Medicine.
Citation: Pamela L Alberto, M Conte,T Scorziello. (2022). Evaluation of Aerosol and Splatter Production using Dental Handpieces and Ultrasonic Scalers during Dental Procedures: A Pilot Study. Dentistry and Oral Maxillofacial Surgery. 5(1); DOI: 10.31579/2643-6612/027
Copyright: © 2022 Pamela L Alberto, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 November 2021 | Accepted: 27 December 2021 | Published: 06 January 2022
Keywords: aerosol; splatter; disease transmission
There have been many articles written about aerosols and splatter during dental procedures with the potential for disease transmission. Due to the global COVID-19 pandemic, aerosol production during dental procedures has been considered a potential disease transmission pathway. Since there is no documented cases of dental professionals acquiring SARS-Cov1 or COVID-19, we decided to see how much aerosol is produced by a Dental High speed drill and ultrasonic scaler. Also if the use of high volume suction can eliminate any aerosol transmission.
A pilot study using Glo Germ in the water to evaluate under blacklight the aerosol pattern and spread produced by a high speed dental handpiece and an ultrasonic scaler was performed. The results found that high volume suction using an 8mm diameter suction tip eliminated aerosol spray spread with a high speed dental handpiece. Minimal aerosol spread was found with the use of a cavitron scaler.
COVID-19 was first reported to the World Health Organization Country Office in China on December 31, 2019. Within a few months, it spread rapidly to become a global pandemic [1]. The mechanism of spread is important to try to prevent exposure. SARS-CoV-2 is thought to be transmitted via 2 mechanisms: 1) inhalation of droplets produced by close contact with infectious people and 2) contact with contaminated surfaces [2]. It is also thought to be transmitted directly or indirectly through saliva. There has been much concern about dental aerosols and splatters potential to transmit disease to dental health care providers. These aerosols are thought to remain suspended in air for 4 hours [3]. So dental health care professionals and patients are exposed to aerosols that contain microorganisms during dental treatment [4]. Harrel and Molinari reviewed the literature about aerosols, splatter and infection control and found that it showed dental procedures produced aerosols and droplets that contained bacteria and blood. These aerosols represent potential route of disease transmission [5]. These articles were not an evidence-based analysis and none determined the exact infection risk from this bioaerosol. Also, There are no documented cases of dental health care worker effected by SARS-Cov1 in a dental setting [6]. Peng and Xu looked at transmission routes of COVID-19 and controls in dental practice and found that no dental professional had reported to acquire COVID-19 infection in China at the time of their paper in February 2020 [3]. The object of our pilot study was to see exactly how much aerosol or splatter is produced during dental procedures and the effectiveness of high volume suction limiting the spread. This would provide information on infection risk during dental procedures.
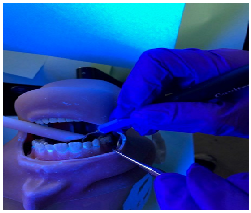
In this study, GloGerm an illumination marker was placed in the bottle resivar water supply of a dental unit. GloGerm contains proven safe ingredients formulated to be the same size as bacteria, basically 5 microns or less in size. An ultra-violet light was used to illuminate and visualize the spread of the aerosol and splatter. Using a high speed handpiece with a small round bur (figure.1), the handpiece was operated with full water on a flat surface to see the direction and amount of aerosol and splatter (Figure.2) and then the handpiece operated 1 inch above the flat surface (figure.3). Operatory lights were turned off and a UV light was used to view the aerosol and splatter pattern. Then a Typodont was placed in an operatory to simulate a patient. Construction paper was placed hanging from the light 2 ft (0.6 meters) down to the typodont. Also construction paper was placed on the chair in front of the typodont (figure.4). Then a preparation was performed on a posterior molar with full water spray and utilization of the existing dental high volume evacuation system with the bevel of the suction tip 90 degrees to the generated aerosol. Then a UV lamp was used to view the aerosol and splatter pattern. The construction paper was changed and then an anterior incisor tooth preparation was performed using a high speed handpiece with full water and the existing dental high volume evacuation system again with the bevel of the plastic suction tip placed at a 90 degree angle to the generated aerosol. Then a UV lamp was used to view the aerosol and splatter pattern. The construction paper was changed. Then an ultrasonic scaler with a high volume suction was used posteriorly for 1 minute (Figure .5). The UV lamp was used to view the aerosol and splatter pattern. The construction paper was changed. The ultrasonic scaler with high volume suction was then used anteriorly for 1 minute. The UV lamp was used to view the aerosol and splatter pattern. All the aerosol and splatter patterns were photographed for evaluation.
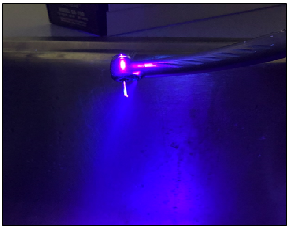

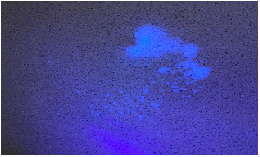


When a high speed handpiece is operated with full water it creates most of the splatter and aerosol posterior to the clockwise turning bur (Figure.1). Operating the handpiece with less water will create the most aerosol. Pam, is this correct? What about reducing the amount of water and “chip air” used to disperse the water spray????????? It would seem logical that we would recommend to reduce both. We then operated the handpiece on the flat surface with the bur just contacting the surface using full water spray and found that no spray could be visualized just a puddle of water in front of the handpiece(Figure.2). Repeating this but lifting the bur 1 inch above the flat surface, splatter and aerosol was visualized posteriorly with the puddle of water anteriorly (Figure .3).
During the typodont simulation, the handpiece was operated with full water spray without high volume suction preparing an anterior tooth. The UV lamp was used to view the aerosol and splatter pattern. There was visible spray or splatter on the construction paper in front of the typodont, on my personal protection gown and gloves but not on my facemask (Figure.6).

During the typodont simulation, the handpiece was operated with full water spray and high volume suction with a 8mm diameter suction tip preparing a posterior tooth. The UV lamp was used to view the aerosol and splatter pattern. There was no visible spray or splatter on the construction paper in front of the typodont, on my face mask or on my personal protection gown. Also no spray was noted on my gloves (Figure .7). Then the handpiece was operated with full water spray and high volume suction with a 8mm diameter suction tip preparing a maxillary central incisor. The UV lamp was used to view the aerosol and splatter pattern. There also was no visible spray or splatter on the construction paper in front of the typodont, on my face mask or on my personal protection gown. Also no spray was noted on my gloves.

Then an ultrasonic scaler without high volume suction was used posteriorly on the typodont for 1 minute. The UV lamp was used to view the aerosol and splatter pattern. There was visible spray on my gloves and gown in my lap. No spray was seen on my face mask. Then an ultrasonic scaler with high volume suction was used posteriorly on the typodont for 1 minute. The UV lamp was used to view the aerosol and splatter pattern. There was visible spray on my gloves. No spray was seen on my face mask. We then utilized the ultrasonic scaler on anterior teeth with no high volume suction. The UV lamp was used to view the aerosol and splatter pattern. There was visible spray on my gloves, gown and mask. When high volume suction was used with the ultrasonic scaler on anterior teeth, we found significant reduction in spray (Figure .8). There was no visible spray on the construction paper or my face mask. There was spray on my gloves, sleeves and lap of my gown.
It has been documented for many decades that dental procedures create aerosols. These aerosols are a natural result of the ether the dental high speed handpiece or ultrasonic instruments’ interaction with the unit supplied coolant, usually water and the working end of the dental instrument. (CHIPPER AIR) This aerosol can be contaminated via two vectors. The first is dental unit waterline biofilm. For years now, the development of a biological plaque buildup in the small diameter water lines has been understood. Many manufactures of dental units have incorporated auto flush valves as well as instructions for use related to shocking and maintaining their water lines. Most of the dental profession has now moved away from the municipal water supply, to a bottle water supply system to counter act the development of this biofilm. It is now a considered a standard of care to monitor the quality of our dental units water. The second vector of contamination of this aerosol originates from contamination via the patients saliva, blood, plaque, calculus [4]. Historically dentistry has been able to manage this contamination of the aerosol through the use of a rubber dam and the high volume evacuation, hence there is no documentation of transmission of airborne diseases from a dental office.
Transmission of SARS-COV2 is thought to be from inhalation of liquid droplets from close contact with infected people, and infected surfaces. Airborne transmission and spread depends on particle size. Coughing or sneezing disperses the pathogens into the air. There are small droplets which are about 1 to 5 microns in diameter that are called droplet nuclei and there are large droplets more than 5 microns in diameter called droplets. Both can carry infectious pathogens. Droplets travel shorter distances about 3 feet, before rapidly falling to the ground where droplet nuclei stay airborne longer. The dental handpiece produces aerosol and splatter which is defined as particles less than 50 microns in diameter for aerosols and splatter defined as particles more than 50 microns in diameter [5]. The SARS coronavirus is spread thru droplets and direct contact [6]. That is why close contact is required for direct transmission.
Our study has shown that aerosols from dental handpieces can almost be completely eliminated with the use of high volume suction. Aerosols from the use of ultrasonic scalers cannot be completely eliminated. This has also been documented in other studies [5]. With the use of high volume suction aerosols should be completely eliminated during dental procedures. Maintaining proper infection control methods with standard PPE and preprocedural rinsed will minimize the risk of exposure with all dental procedures [8]. Since no data exist regarding the infectivity of contaminated saliva through the droplet route more studies are needed.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
