
Case Report | DOI: https://doi.org/10.31579/2694-0248/032
1 Central Mexican University in Stomatology, Specialty of Orthodontics and degree in Stomatology Campus Veracruz, Mexico.
2 University of Stomatological Sciences of Havana. Faculty of Stomatology. Havana Cuba.
3 University of Medical Sciences of Havana. Faculty of Medical Sciences "Finlay-Albarrán". Department of Medicine. Havana Cuba.
*Corresponding Author: Agustín Arano Hernández, Av. Juárez 603-A col centro, C.P. 95100 Tierra Blanca, Veracruz Central Mexican University in Stomatology. Department of Orthodontics. Veracruz, Ver. (Mexico).
Citation: Agustín A. Hernández, C Ileana Bárbara Grau León, Marisel I. Carreras, (2022). Evaluation and Multidisciplinary Treatment of a Patient with Temporomandibular Disorder. J. Clinical Orthopedics and Trauma Care, 4(2); DOI:10.31579/2694-0248/032
Copyright: © 2022 Agustín Arano Hernández, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2022 | Accepted: 15 February 2022 | Published: 21 February 2022
Keywords: temporomandibular joint; temporomandibular disorder; position
Background
Demonstrate that patients with signs and symptoms of the temporomandibular joint, prior to orthodontic treatment, should be treated multidisciplinary
A 31-year-old female, a student at the Mexican Center for Stomatology, with a personal and family health history and orthodontic treatment who came to the clinic for presenting symptoms of pain in the face over the region of the bilateral temporomandibular joint, with alterations of the function, which radiated to the neck and back of several months of evolution. The clinical findings presented by the patient were: wear on the upper anterior teeth. The pain map diagnostic index was used, photographs of the face, whole body from the front and sides, panoramic radiography, lateral skull, anteroposterior and spine, articulated models in semi-adjustable articulator, this facilitated us to diagnose joint disorders. The proposed treatment was multidisciplinary treatment: Neuro-muscular rehabilitation and the use of physical agents, massage therapy, Kinesiology and manual therapy.
The multidisciplinary treatment of occlusal guard by stomatology and the combination of physical agents, Kinesiology and manual therapy by physiotherapy, demonstrated excellent results with the disappearance of the symptoms in the patient, improved her expectations. Giving you a better quality of life.
The temporomandibular joint (TMJ) is a synovial joint that connects the jaw with the skull through the temporal bone. It is one of the most complex in the body, it is part of the masticatory system. There are two joints, one right and one left, they are located on both sides of the face at the level of the base of the skull, it can be easily palpated in front of the external auditory meatus. [1] The stomatognathic system is closely related to the control of posture. It is a functional unit, characterized by various structures, such as skeletal components (maxilla and mandible), dental arches, soft tissues (salivary glands, nerve and vascular supplies). [2]
This joint system includes jaw movements for chewing food, interferes with swallowing and phonation, as well as intervening in breathing and the sense of taste. [1] The etiology of temporomandibular joint dysfunction constitutes one of the most controversial issues, and it can be assured that it is multifactorial in nature. [3]
Orthodontics is an irreversible procedure that corrects dental defects and bad positions, improves function, aesthetics, and everything that refers to oral health. This treatment produces an important impact on the soft tissues of the TMJ, which is why they manifest pain, the literature shows some alternatives to reduce the associated pain. [3] There are such as that relate orthodontics to TMJ alterations, as a cause of this, but also to be the solution for the treatment of these alterations [1], making a diagnosis with tools such as diagnostic indices; like the map of pain [4], the assembly of the articulated models in semi-adjustable articulators, in this way our treatment will be carried out based on the findings of our patients with alterations in the TMJ joint, a multidisciplinary treatment with stomatological and medical specialties. Demonstrate that patients with signs and symptoms of the temporomandibular joint, prior to orthodontic treatment, should be treated multidisciplinary
A female patient, 31 years old, Latino origin, student of the orthodontic specialty at the Mexican Center in Stomatology Campus Veracruz, with personal and family health history and orthodontic treatment who came to the consultation for presenting symptoms of pain in the face over the region of the bilateral temporomandibular joint, which radiated to the neck and back for several months of evolution. Upon questioning, he referred, in addition to the aforementioned symptoms, stiffness when walking and pain in his hips and knees. Anteroposterior, lateral skull and lateral lumbosacral spine radiographic studies were requested, as well as extraoral and intraoral photographs. As a treatment plan, the orthodontic appliances were removed. The need for interconsultations with the physiotherapist and chiropractor was explained to him, in order to start a multidisciplinary treatment and thus reduce the symptoms of pain that occur in the posterior region of the neck, back, hips and knees.
Clinical Findings.
The diagnosis of the proportions of the face and face; Vertical as well as horizontal, as well as the midface alignment by means of the extraoral photographs from the front shows us that there is a very marked asymmetry, where the right side of the patient is less developed than the left side. (Figure. 1)

In the photos standing from the front, scapular asymmetry is observed, the right shoulder is higher than the left shoulder, the right side and the left side show a very marked lordosis, (Figure. 2) corroborated with the spinal radiographs that the physiatrist requested.
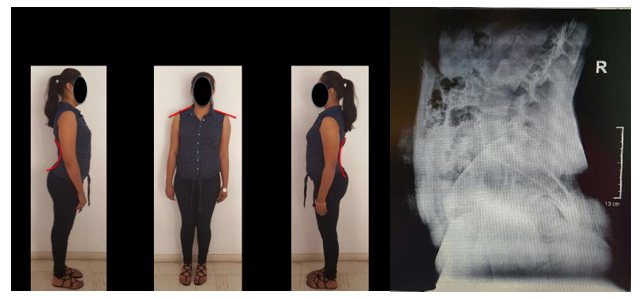
B. X-ray (very marked lordosis).
In the occlusal analysis, it is observed that the patient presented wear of the cusps of the upper canines on the right and left sides, the midline deviated to the right, with the absence of the lower right first molar, there is a discrepancy where there is not a good occlusion from the incisors central to the second molars on the right side, with Angle class II of canines and molars. On the left side, a good usual Angle class I occlusion is maintained. (Figure. 3). This analysis was carried out in habitual occlusion and reported very different data in the models mounted on a semi-adjustable articulator in Centric Relationship (CR).

In the occlusal analysis of models mounted in centric relation (CR) in a semi-adjustable articulator, it is observed that there are only contact points in the second molars; type B contacts on the right side and type C contacts on the left side, canine and molar class II on both sides, deviation from the midline to the right (Figure. 4).
In the record of the condylar position (CPI) it is observed that the condyle on the right side 5 mm downwards and on the left side 4 mm down and 3 mm backwards. With this diagnosis, it is confirmed that temporomandibular disorders (TMD) are the cause of pain in the chewing muscles and muscle stiffness in the head, neck and back that the patient presents (Figure. 4B).

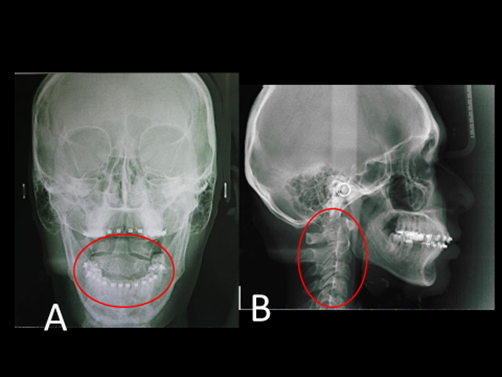
In the posteroanterior radiography (PA) we observed that there is a rotation of the second cervical downward on the left side and upward on the right side, which corroborates the asymmetry and more marked facial development on one side than the other. Figure. 6A In the lateral radiograph of the skull, rectification of the cervical vertebrae is observed, which is the cause of pain in the posterior region of the neck. Figure. 6B
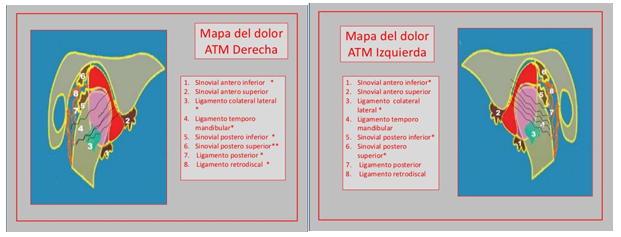
When palpating the chewing muscles; temporal in its anterior portion, superficial and deep masseter, the posterior parts of the neck and the upper trapezius on both sides, the symptoms were of intense pain, as well as in the TMJ pain map [4] five pain points on the right side; inferior and superior anterior synovium, lateral collateral ligament, temporomandibular ligament, superior posterior ligament and four pain points on the left side, inferior anterior synovium, lateral collateral ligament, temporomandibular ligament and inferior postero-mandibular synovium, they had severe pain, therefore, With the condylar distraction marked by the ICC of the semi-adjustable articulator of five mm on the right side downwards, four mm downwards and three mm backwards on the left side, we found that the patient had a very severe temporomandibular dysfunction. [4]
Therapeutic intervention
Stomatological therapy was started with the prior consent of the patient, who expressed his disposition through informed consent, for this treatment with neuro-muscular rehabilitation (MRI), using a stabilizing upper 4.5 mm occlusal guard. thick in the anterior part, made of heat-cured acrylic, the use of the occlusal guard is recommended for 24 hours for 4 months, with monthly adjustment of the contact points.
Adjustments were made to obtain bilateral contact points of the same intensity in posterior teeth and anterior teeth with soft contact points with sliding of the articulating role.
The symptoms decreased month by month until they disappeared, a map of muscle and joint pain [4] was made at each monthly appointment to obtain information and thus be able to evaluate the decrease in pain in the chewing muscles and TMJ. A diet free of sugar, caffeine, alcoholic beverages or any stimulant of the central nervous system (CNS) is also recommended [2,4]. Reduced use of cell phones and computers, so as not to maintain bad posture for a long time and to trigger muscle pain in the posterior muscles of the neck and upper trapezius [2,4]. Therefore, specialists in the medical area of physiotherapy are referred to attend and continue with their therapy until giving the patient quality of life.
From the point of view of physiotherapy, this patient begins with global postural re-education and education that includes a soft diet, avoiding wide yawning, as well as singing and chewing gum.
All these treatments were performed on a daily basis for 2 weeks. It was suggested to maintain self-massage, stretching, and self-assisted exercises for 4 weeks to achieve changes in posture, asymmetries, muscle dominance, increase joint range, and improve biopsychosocial well-being [7, 8].
Clinical outcomes
With the use of the occlusal guard, the patient manifested from the first month of therapy, decreased pain and muscle stiffness in the posterior region of the neck and back, in addition to mobility and pain in the TMJ, with neuromuscular rehabilitation and Physiotherapy is obtained the total remission of the symptoms, during the treatment there were no complications or adverse effects.
Among the most common symptoms in TMJ disorders is pain over the region of the temporomandibular joint, in our patient bilateral pain and its radiation to the neck and back with alteration of her posture is evidenced. It is proven that a posture with a shoulder push and neck flexion promotes propulsion of the jaw. [9] In a study carried out, it was shown that women with TMJ disc displacement presented pain and postural alterations in the pelvis, lumbar spine, thoracic spine, head and mainly pain in the jaw, [10] which coincided with our patient.
In another study it was shown that there are interactions between locomotion and occlusion after studying 30 adult women, a cotton roll was placed unilaterally in each dental arch while they were walking. It was the percentage and the load surface of the foot (right and left) significantly lower than in the usual occlusion. [11] In a last study, in which occlusal alterations and their relationship with TMJ dysfunctions were treated, it was observed how headaches and neck pain decreased, which coincided with our patient. It is the alignment of said joint important in the postural alterations of the body since ergonomics is influenced by the relationship that the chewing muscles maintain with the head and neck. [11]
Gallardo (12) and other collaborators carried out a study to evaluate the results obtained in patients treated with occlusal guards who present signs or symptoms of some TMD; a study in which the sample comprised 10 patients with limitations in their jaw movements and treated with occlusal splints showed that of the total sample, 80% had some kind of pain. The end of the treatment only 10% reported pain, the mean maximum initial opening was 35.7 mm and the final average was 44.8 mm for desoclusiones and contact the occlusal splint. [12] Obtaining improvement in pain relief as in our patient.
The treatment of these disorders is conservative, where the results obtained in this clinical case agree with those reflected by these authors Shousha and others, [13] van Grootel and others, [14] Calixtre and others, [15] Ucar and others, [7] Gil-Martínez and others, [8] used physiotherapy techniques (US, mobilizations, neuromuscular techniques, stretching, massage therapy, laser and therapeutic exercise), and the use of occlusal splints [5, 6] in the treatment of temporomandibular disorders, improvement is obtained in his patients.
In addition, some authors take into account in their results some less common variables such as Viana and others [5] and Kraus and Prodoehl, [17] who evaluate the quality of life after a physiotherapy treatment and van Grootel and others [14], the duration of the treatments either with physical therapy or with splints. All of them obtain good results in favor of physiotherapy, despite the fact that the authors consider that there is not much literature with which to compare them, therefore, it is suggested to carry out more research in this field to confirm the results presented.
There was improvement in the symptoms that the patient manifested, after carrying out the multidisciplinary treatment of occlusal guard and the combination of physical agents, massage therapy, Kinesiology and manual therapy. Multidisciplinary treatment proved to be an excellent alternative in this patient, which allowed her to improve her expectations and provide her with a better quality of life.
Appendix 1
Map of joint pain by Dr. Mariano Rocabado Seaton
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
